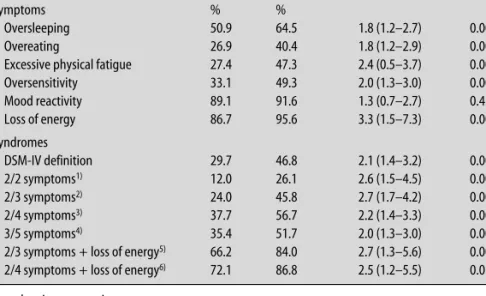
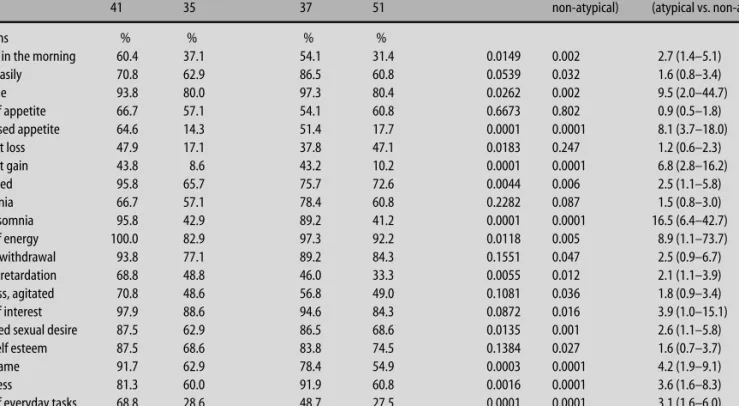
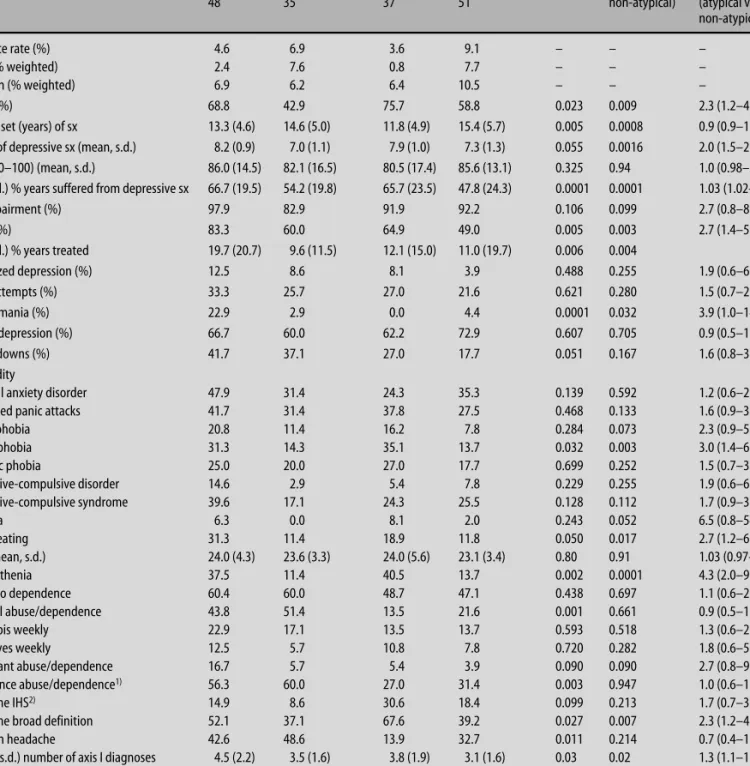
Atypical depressive syndromes in varying definitions
Texte intégral
Figure


Documents relatifs
As shown in Table 3, the results of the second regression model showed that Facebook surveillance was greater in people whose relationship status indicated lower commitment, and as
Clémence Beauruelle, Hervé Le Bars, Nolwenn Astruc, Didier Tandé, Rozenn Le Berre, Geneviève Héry-Arnaud.. To cite
In this regard, we observe that depressed patients of our sample declared a significantly poorer global health status than non-depressed patients as well as higher levels of
To achieve a normally-off HEMT with high forward gate voltage, using a relatively low p-doping concentration, an hybrid normally-off HEMT was proposed using two p-GaN
For the chemical model, we considered both the un- certainties in the rate coefficients and in the physical con- ditions, using Model 2 for both clouds. To compare the observed
More generally, a change in the shape of the model SED will help to get better residuals, either by using more than a single-ISRF environment, or by changing the dust grain size
Les membres sont tenus, dans l’exercice de leurs fonctions, de respecter les règles de déontologie et les principes d’éthique prévus par la loi et par le Règlement sur
This 4-year follow-up provides evidence that long-term participation to a music-based multitask exercise program can prevent physical decline and reduce falls in commu-
