Cut-resistant protective gloves in pathology—effective and cost-effective
6
0
0
Texte intégral
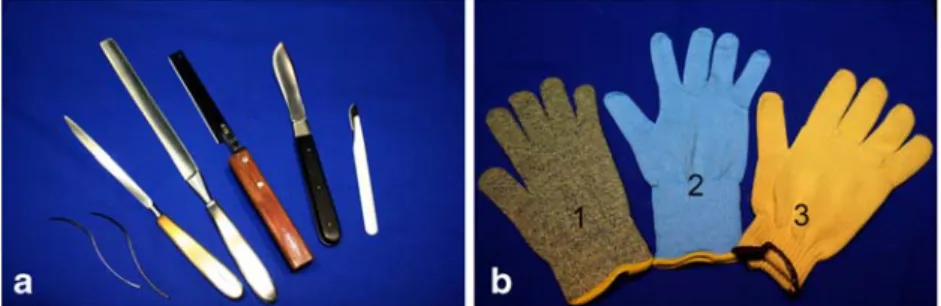
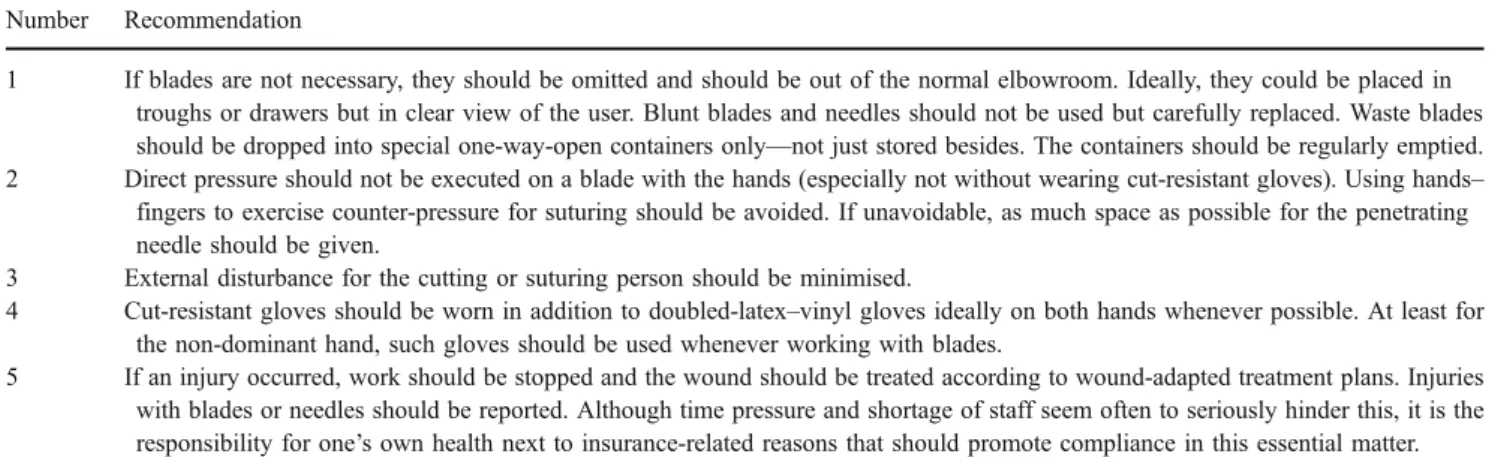
Figure
Documents relatifs