Acoustic radiation force impulse imaging—normal values of liver stiffness in healthy children
Texte intégral
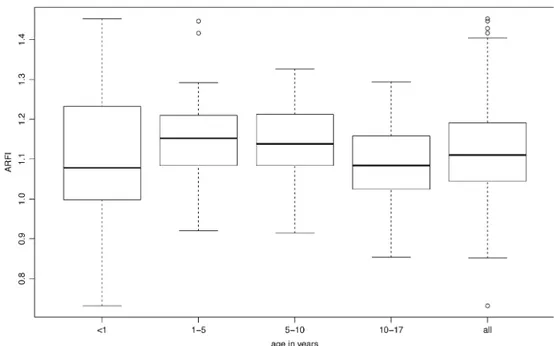
Figure
![Table 1 Characteristics of acoustic radiation force impulse (ARFI) [m/s]](https://thumb-eu.123doks.com/thumbv2/123doknet/14846572.627664/3.892.263.816.74.411/table-characteristics-acoustic-radiation-force-impulse-arfi-m.webp)
Documents relatifs
ﺔﻣدﻘﻣ : نﯾﺛﺣﺎﺑﻟا نﻣ رﯾﺛﻛﻟا مﺎﻣﺗھﺎﺑ ىرﺧﻷا نﻣ هرﯾﻐﻛ ﺔﯾﺟرﺎﺧﻟا ﺔﺳﺎﯾﺳﻟا عوﺿوﻣ ﻰظﺣﯾ ﺔﯾﺎﮭﻧ تﺑﻘﻋأ ﻲﺗﻟا ةرﺗﻔﻟا لﻼﺧﻓ،مھرﺎﻛﻓأو مﮭﻣﯾﻗو مﮭﺑرﺎﺷﻣ فﻼﺗﺧا
However, comparison of Nanos3 protein levels in mouse tumor- derived LuTDNA3 cell lines and Nanos3 overexpressing human NSCLC cell lines did not show higher Nanos3 protein levels in
3 (LM86), and the contents of the box are vented completely out of the box in the time required for the mean wind speed to cross the box from one side to the other, with a series
Leaf water potential can be shifted more than 1 MPa, by exposing the whole plant to dry or moist air, but stomata close independent of the water potential in the leaf by a response
It is listed in UIrich's Intenwtional Periodicals Directory, abstracted by Sociology of Education Abstractsand Canadian Social Science Abstracts, and isavailable on
Scaling characteristics of the time series were calculated by using three methods of data processing: spectral analysis (FFT), the Burlaga-Klein (BK) method and the Higuchi (H)
[r]
[r]
