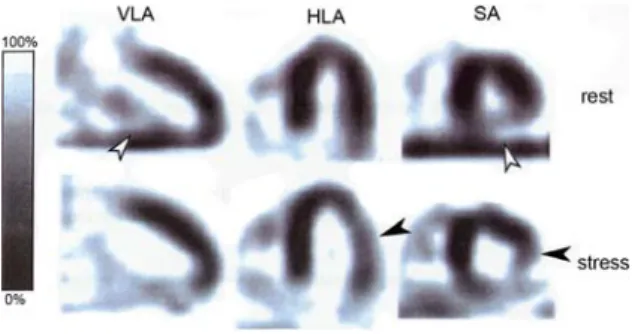
Diagnostic accuracy of myocardial perfusion imaging with single photon emission computed tomography and positron emission tomography: a comparison with coronary angiography
Texte intégral
Figure

Documents relatifs
Purpose: In yttrium‑90 (Y‑90) single‑photon emission computed tomography (SPECT) imaging, the choice of the acquisition energy window is not trivial, due to the
CT: X-ray computed tomography; MRI: magnetic resonance imaging; PET: positron emission tomography; SPECT: single photon emission computed tomography; 18 F: fluorine--18, 15
Aims Several studies reported on the moderate diagnostic yield of elective invasive coronary angiography (ICA) regarding the presence of coronary artery disease (CAD), but limited
Background: This study assesses the accuracy of the new dual-source computed tomography (DSCT) for detection of coronary artery disease (CAD) compared with invasive coronary
A cardiac positron emission tomography – computed tomography (PET – CT) was performed and disclosed enhanced fluor-18 fluorodeoxyglucose (FDG) uptake in the wall of the aortic
Positron emission tomography –computed tomography scan helps decision making in cardiac surgery Sanjay Cherian a , René Nkoulou b , Afksendiyos Kalangos a and Mustafa Cikirikcioglu
• This paper reports a rare case of primary mucosal melanoma of the middle ear, imaged with fluoro- deoxyglucose positron emission tomography /.. computed tomography
Rest Tc-99 m sestamibi myocardial perfusion single photon emission computed tomography (SPECT) has been used to exclude acute coronary syndrome in ED patients presenting with chest
