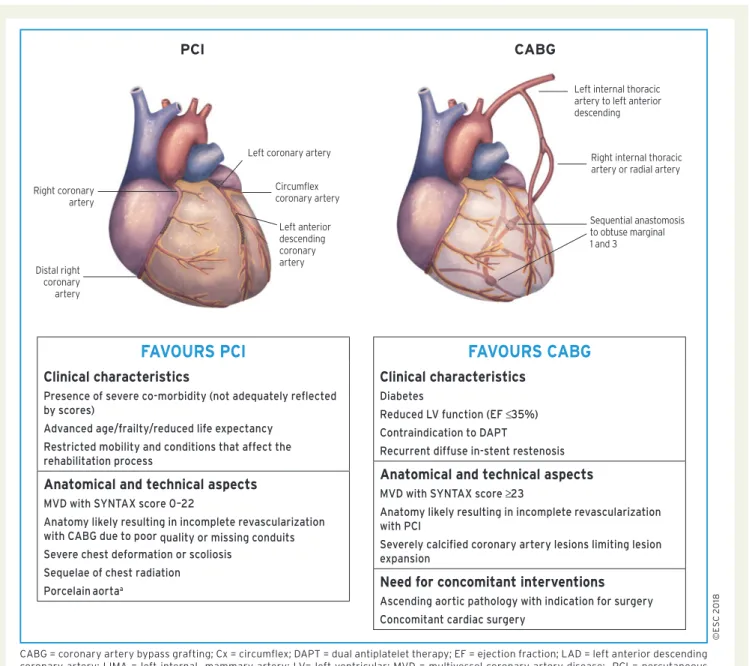
2018 ESC/EACTS Guidelines on Myocardial Revascularization
Texte intégral
Figure
Documents relatifs
A Parallel Adaptive Vlasov Solver Based on Hierarchical Finite Element Interpolation Michel Mehrenberger, Eric Violard, Olivier Hoenen, Martin Campos Pinto, Eric Sonnendrücker.. To
In this paper, we consider the movement of a rigid body immersed in a perfect incompressible fluid in the plane.. The solutions that we will consider are weak solutions in the spirit
Then, five members are selected from the super-ensemble and used to provide initial and boundary conditions for the integrations with a limited-area model, whose runs generate
Qui est toute puissante qui a toujours raison La France dominée par les aristocrates Devra privilégier le pouvoir démocrate Le peuple est le seul à devoir s'exprimer Par un exécutif
Dans le réflexe myotatique, l’étirement du muscle extenseur est détecté par les fuseaux neuromusculaires (FNM), récepteurs proprioceptifs sensibles à
A broad overview of current research activities in reliability theory and its applications is provided with coverage on reliability modeling, network and system
Deux enfants montent dans le
