Chronic pain and pain processing in Parkinson’s disease
Pierre J. Blanchet, MD, FRCP(C), PhD
Department of Stomatology, Faculty of Dental Medicine, Université de Montréal; Service de neurologie, CHU Montréal, Montréal (QC), Canada
E-mail: [email protected] Phone: (514) 343-7126
Christine Brefel-Courbon, MD
Service de Pharmacologie Clinique, Faculty of Medicine, University Hospital, Toulouse, France; Service de neurologie B8, Pierre Paul Riquet Hospital, University Hospital, Toulouse,
France
E-mail: [email protected] Phone: 33 5 61 14 59 62
Summary (250 words maximum)
Pain is experienced by the vast majority of patients living with Parkinson’s disease. It is most often of nociceptive origin, but may also be ascribed to neuropathic (radicular or central) or miscellaneous sources. The recently validated King’s Parkinson’s Disease Pain Scale is based on 7 domains including musculoskeletal pain, chronic body pain (central or visceral), fluctuation-related pain, nocturnal pain, oro-facial pain, pain with discolouration/oedema/swelling, and radicular pain. The basal ganglia integrate incoming nociceptive information and contribute to coordinated motor responses in pain avoidance and nocifensive behaviors. In Parkinson’s disease, nigral and extra-nigral pathology, involving cortical areas, brainstem nuclei, and spinal cord, may contribute to abnormal central nociceptive processing in patients experiencing pain or not. The dopamine deficit lowers multimodal pain thresholds that are amenable to correction following levodopa dosing. Functional brain imaging with positron emission tomography following administration of H215O revealed abnormalities in the sensory discriminative processing of pain (insula/SII), as well as in the affective motivational processing of pain (anterior cingulate cortex, prefrontal cortex). Pain management is dependent on efforts invested in diagnostic accuracy to distinguish nociceptive from neuropathic pain. Treatment requires an integrated approach including strategies to lessen levodopa-related response fluctuations, in addition to other pharmacological and non-pharmacological options such as deep brain stimulation and rehabilitation.
Highlights
Pain is common at all stages in Parkinson’s disease, even as a premotor manifestation. It is heterogeneous and falls under nociceptive, neuropathic, and miscellaneous
sources.
Nigral and extra-nigral pathology may contribute to abnormal information processing in medial and lateral pain systems.
Dopamine deficit lowers multimodal pain thresholds that may be corrected following levodopa dosing.
Treatment requires an interdisciplinary approach in addition to strategies to lessen motor response fluctuations.
Introduction
Patients living with Parkinson’s disease (PD) can literally suffer from the condition. Long before the advent of levodopa, various pain manifestations, dysesthesias, and cramps had been described in one-half of patients (Sigwald and Solignac, 1960). Pain was recognized long ago as a possible premotor symptom, and its intensity could be severe enough to become the chief complaint. The pre-levodopa literature suggested that pain may be revealed or aggravated by therapeutics. In the last 30 years, increased awareness of pain as a nonmotor symptom in a large fraction of PD patients with levodopa-related fluctuations has generated an extensive body of research into the causative mechanisms and management strategies. Nonetheless, the mechanisms of abnormal nociceptive processing and modulation by supraspinal mechanisms, as well as the influence of levodopa replacement therapy, remain unclear. The pain threshold, brain network of regional changes associated with pain in PD, and relationship of pain with depression, sleep deprivation, and quality of life, have been examined. Pain in PD may be difficult to treat and may require an interdisciplinary approach for proper management and wise prescription of analgesic drugs.
Prevalence and types of chronic pain
Chronic pain is prevalent with age in the general population, but figures vary according to the criteria used for duration and level of pain intensity. Moderate to severe pain lasting at least 6 months is reported by 19% of the general population (Breivik et al., 2006), but more inclusive criteria raise the prevalence rates up to 40% (Verhaak et al., 1998), further doubling amongst nursing home residents (Fox et al., 1999). Pain is highly heterogeneous in the PD population, and many syndromes have been delineated (Ford, 1998; Wasner and Deuschl, 2012). The
reliance on clinical judgment alone, lack of standardized tools to determine whether or not a given pain source is considered a feature of PD, and disparity in pain descriptions, have complicated the subclassification of pain as directly related (caused by PD only), indirectly related (aggravated by PD), or unrelated (attributed to any other health problem) to PD (Lee et al., 2006; Nègre-Pagès et al., 2008) (Table 1).
Pain in PD has been assessed by different methods, including home-made surveys, clinical interview and evaluation, Short Form McGill Pain Questionnaire, Leeds Assessment of Neuropathic Symptoms and Signs, Brief Pain Inventory, the body pain items of the 36-Item Short Form (SF-36) Health Survey, and the pain item of the Non-Motor Symptoms Scale (Chaudhuri et al., 2007). Recently, the specific King’s PD Pain Scale (KPPS) was validated to assess pain (Chaudhuri et al., 2015). Fourteen items in 7 domains encompass recognized categories of pain in PD, including musculoskeletal pain, chronic body pain (central or visceral), fluctuation-related pain, dyskinetic-dystonic pain, nocturnal pain (linked to immobility or restless legs), oro-facial pain, discolouration/oedema/swelling, and radicular pain. This classification falls into the broad nociceptive, neuropathic, and miscellaneous sources of chronic pain in PD proposed by others (Wasner and Deuschl, 2012), but does not allow a physiopathological classification of pain. The Movement Disorder Society’s review in pain rating scale in PD does not recommend this scale for syndromic classification and suggests it only (Perez Lloret et al., 2016).
Since Souques (1921), central parkinsonian pain has been accepted as a separate entity. The following criteria have been applied (Ford, 1998): emergence of pain before the onset of motor symptoms; first appearance of pain on the side the motor symptoms appeared; unexplained abdominal or genital pain; pain unexplained by other causes, either related or unrelated to PD (arthritis, musculoskeletal or dystonic pain). Its prevalence is estimated between 4.5% and 22% of cases (Defazio et al., 2008; Valkovic et al., 2015; Buhmann et al.,
2017). Other unusual and uncommon pain descriptions involving the oral area have also been thought to have a central origin (Ford et al., 1996). Central Parkinsonian pain is probably underestimated because the diagnostic criteria are not well defined and overlap with those of musculoskeletal pain.
Pain is highly prevalent in PD and occurs in 30-95% of patients (Beiske et al., 2009; Broen et al., 2012; Valkovic et al., 2015; Buhmann et al., 2017). In a dataset of 198 PD patients (Bonenfant et al., 2016), the prevalence of body pain regardless of distribution and type was 74.2%. In a cross sectional French survey conducted in 278 PD patients experiencing chronic pain, 65% had PD-related pain (Nègre-Pagès et al., 2008). In comparison, chronic pain occurs in 30% (11-55%) of stroke victims (Paolucci et al., 2016). A pharmacoepidemiological approach has also been used to estimate the prevalence of pain in PD patients from the chronic consumption of analgesic drugs collected from a French Health Insurance database (Brefel-Courbon et al., 2009). This study, carried out in more than 11,000 patients with PD, showed that the chronic analgesic prescription was higher in PD patients compared to the general population (33% versus 20%) and was remarkably identical to that of patients with osteoarthritis. Pain assessed through the SF-36 was experienced much more commonly in PD patients (83%) than in controls (30%) (Beiske et al., 2009). In one study, the prevalence (%) of the different pain types was as follows: musculoskeletal (70), central (10), dystonic (40), radicular-neuropathic (20) (Beiske et al., 2009). In another, prevalence figures were: musculoskeletal (41), central (22), dystonic (17), radicular-neuropathic (27), or others (31) (Valkovic et al., 2015). In comparison, neuropathic pain (often radicular in origin) is estimated to affect 7-10% of the general population (Colloca et al., 2017). Nearly 30% of patients reported more than one pain type (Beiske et al., 2009), a proportion found to be 51.5% in our dataset, and as high as 71% in another report (Valkovic et al., 2015). Musculoskeletal pain is common in PD. Patients may experience unexplained, non-traumatic
shoulder pain as a presenting feature of the illness, before motor symptoms become apparent in the ipsilateral arm. In retrospective reports, this was the case in 2% (Stamey et al., 2008) and 8% (Riley et al., 1989) of patients diagnosed with PD. Back pain is nearly 3-fold more prevalent in PD affecting 74% of patients, is more intense, and more commonly associated with radicular pain and deficits than in the general population (Broetz et al., 2007), possibly due to changes in posture and muscle tone. Using clinical assessment, others have concluded that only dystonic and central pain types distinguished PD patients from age-matched healthy volunteers (Defazio et al., 2008). Of note, BMS is infrequent in PD according to a dedicated survey on the issue, with a prevalence of nearly 4% comparable to that reported in the general population, and its occurrence does not correlate with PD duration and severity, or levodopa equivalent daily dosing (Bonenfant et al., 2016).
Pain can appear early in the course of PD, even as a pre-motor symptom (before the onset of motor symptoms). Anatomo-clinical study in 433 PD patients showed that 21% of patients had exclusive non-motor symptomatology during the prodromal phase, and pain was the most frequently reported symptom (O’Sullivan et al., 2008). A study based on a Taiwanese cohort follow-up reported that subjects with moderate to severe pain had a higher incidence of developing PD with a hazard ratio of 2.88 (Lin et al., 2013). According to Braak's hypothesis, lesions of Parkinson's disease follow a caudo-rostral progression within the central nervous system. Early documented pathology in the locus coeruleus and nuclei of the raphe, before substantia nigra involvement and clinical onset of motor symptoms, could play a role in the pre-motor occurrence of pain in PD (Hawkes et al., 2010). Another study, based on a questionnaire proposed to newly diagnosed untreated PD patients (N=109) and controls (N=107), found unexplained pain reported by 20% of patients in a time period of 2 to 10 years before the onset of motor symptoms (Pont-Sunyer et al,, 2015). Pain is not only an early
symptom and even a pre-motor in PD, but it is also more prevalent with disease progression (Barone et al,, 2009).
Predictive factors for pain development in PD have been examined in few studies reaching no consensus. Differences in sample size, patient population, assessment methods, and study design, may underlie these discrepant results. In a survey (N=123), pain did not correlate with age, disease stage or duration, or depression (Lee et al., 2006). In other studies, female gender (Beiske et al., 2009), younger age (Goetz et al., 1986; Nègre-Pagès et al., 2008), presence of motor response fluctuations (Goetz et al., 1986; Quinn et al., 1986; Nègre-Pagès et al., 2008), longer disease duration (Valkovic et al., 2015), and depression (Starkstein et al., 1991; Nègre-Pagès et al., 2008; Ehrt et al., 2009), have been proposed as significant predictors.
Pathological predisposition
Basal ganglia and pain
Unlike components of the medial pain (medial thalamus, anterior cingulate cortex, anterior insula) and lateral pain (lateral thalamus, S1 and S2 somatosensory cortex, posterior insula) systems, basal ganglia functions and disorders have not been traditionally associated with nociceptive inputs processing and central pain. An enriched body of literature published since the 1970’s, and important contributions from Chudler and Dong (1995) and Borsook et al. (2010), have supported the concept that the basal ganglia integrate incoming nociceptive information to contribute to coordinated, graded motor responses in complex, spatially-guided, pain avoidance and nocifensive behaviors. Single neurons in the substantia nigra, neostriatum, and pallidum may selectively respond to nociceptive stimuli, many of them encoding stimulus intensity, but they often display multisensory properties, large bilateral
receptive fields, and lack somatotopic arrangement (Chudler and Dong, 1995). For instance, certain caudate neurons discharge early after a cue in a pain avoidance task in rat (White and Rebec, 1993) and macaque (Koyama et al., 2000). Nociceptive signals may reach the basal ganglia through direct or indirect inputs from the sensorimotor cortex, medial and posterior thalamus, parabrachial area, raphe nuclei, superior colliculus, hypothalamus, and amygdala (Chudler and Dong, 1995). Dopamine is a key neurotransmitter in the modulation of pain perception, and rodent experiments showed that dopamine is involved in the descending antinociception mediated in the rostral agranular insular cortex (Burkey et al., 1999).
Lesions of the rat caudate nucleus impaired the behavioral response in a pain avoidance task (Kirkby and Kimble, 1968). Deep pain may arise in humans following focal lenticular infarction, but the integrity of nearby pathways is difficult to ascertain in such cases (Russmann et al., 2003). Opiate receptor-mediated mechanisms could contribute, since evidence for analgesia was documented in rats following intrapallidal morphine injections, particularly in the dorsomedial sector (Anagnostakis et al., 1992). In fact, many opioid receptors are present both in the pain matrix and in the striatum (Borsook et al., 2010). Several behavioral studies have shown that the opioid system in the basal ganglia was involved in nociception (Chudler and Dong, 1995). For example, intranigral injection of a toxin (6-OHDA) destroying the dopaminergic system blocked opioid-induced analgesia (Morgan et al., 1990). Similarly, the systemic administration of dopaminergic antagonists decreased morphine analgesia while the administration of dopaminergic agonists potentiated it (Gupta et al., 1989; Morgan et al., 1991). All these results suggest that dopaminergic deficiency may reduce analgesia induced by the opioid system.
The midbrain dopamine systems clearly contribute to pain-related responses. The SN and VTA send ascending dopaminergic projections to these subcortical targets and various limbic cortical areas (mainly septal area, prefrontal cortex and cingulate gyrus). Nociceptive stimuli
increase the activity of mesocortical and mesolimbic neurons, and the local release of dopamine (Mantz et al., 1989; Cenci et al., 1992; Altier and Stewart, 1999). Enhancement of dopamine concentrations in the nucleus accumbens through local infusions of amphetamine provides analgesia in rats (Altier and Stewart, 1999). Extracellular recordings of SN (presumably dopaminergic) neuronal discharges to nociceptive stimuli in anesthetized rats showed intensity-dependent, mixed (inhibitory and excitatory) responses (Gao et al., 1990). In animal models, SN stimulation produced analgesia and inhibition of polysynaptic spinal reflexes (Jurna et al., 1978), as well as inhibition of dorsal horn neurons (Barnes et al., 1979) and thalamic parafascicular neurons (Li et al., 1992) activated by noxious stimuli. In contrast, local dopamine denervation in the SN/VTA or striatum in rats decreased latencies of nociceptive reflexes from the contralateral hindlimb and caused hyperalgesia (Saadé et al., 1997), but changes in ipsilateral limb responses have also been observed (Carey, 1986; Takeda et al., 2005).
Nigral pathology and parkinsonian pain
In PD, no focal lesions are found along the somatosensory pathways or basal ganglia outside the substantia nigra. Instead, neuronal loss occurs at multiple levels of the nervous system and the ensuing neurochemical deficits produce far-reaching functional alterations (Table 2). The best characterized pathological circuits in PD are the ascending midbrain dopaminergic pathways projecting to the striatum, nucleus accumbens, and cerebral cortex. The A9 (substantia nigra pars compacta) neurons at the origin of the nigrostriatal motor pathway bears the brunt of the disease, but A10 (ventral tegmental area) neurons at the origin of the mesolimbic pathway are not spared. Accordingly, the putamen is most depleted in dopamine synthesis and storage capacity in [18F]fluorodopa PET studies. Other targets, such as the
medial nucleus accumbens, dorsolateral prefrontal cortex, and anterior cingulate cortex, may show focal hot spots of increased [18F]dopa utilization in early disease, probably due to compensatory mechanisms to maintain dopamine transmission in a partially denervated circuit (Kumakura et al., 2010).
Extra-nigral pathology and parkinsonian pain
Together with the parabrachial nuclei, the periaqueductal gray, and the anterior cingulate area, the midline thalamic nuclei constitute the medial pain system, which generates the autonomic, nocifensive, and emotional reactions evoked by painful stimuli. It is underappreciated that intralaminar thalamic nuclei (central lateral, central medial, paracentral, limitans-suprageniculate complex, parafascicular nucleus, paraventricular nuclei, reuniens nucleus) are not only severely affected in PD (Rüb et al., 2002), but they also receive a complex bilateral dopaminergic innervation from midbrain, periaqueductal gray, and hypothalamus cell groups. Subcortical structures contributing to descending analgesia systems, including the periaqueductal gray, parabrachial area, serotoninergic nuclei of the lower raphe system, magnocellular portions of the reticular formation, and hypothalamus, are involved early in the disease process at stages 2 of Braak pathological classification, before substantia nigra involvement at stages 3-4 (Del Tredici and Braak, 2016). These projections regulate medullary and spinal cord centres, and may propagate a synuclein-immunoreactive axonopathy to the spinal cord at stage 2 that proceeds along a rostrocaudal gradient (Del Tredici and Braak, 2012). Select types of projection neurons in the spinal cord gray matter then display synuclein-immunoreactive inclusions, particularly nociceptive, medium-sized multipolar neurons of the dorsal horn in layer 1, sympathetic and parasympathetic preganglionic neurons in layer 7, and motoneurons in layer 9.
The main cutaneous afferents to the neurons of layer 1 are the unmyelinated and sparsely myelinated A-delta and C fibres that have been found to degenerate in PD, even in early stages (Kanda et al., 1996; Nolano et al., 2008, 2017). Neurodegeneration of the primary afferent nociceptors by the disease process has been hypothesized to play a key role in PD pain (Reichling and Levine, 2011). The concept that cutaneous denervation due to a generalized distal axonopathy as part of the PD pathology is associated with the development of peripheral neuropathic pain deserves further exploration, in order to correlate these nerve changes with other functional and pharmacological considerations.
With the progression of the disease into pathological stages 5-6, many cortical areas, including those subserving pain processing functions, become severely affected (Hawkes et al., 2010). The cortical morphological alterations implicated in the development of PD pain have also been examined in 40 patients (half with chronic pain) using structural diffusion tensor imaging (Polli et al., 2016). The subjects with pain showed relative cortical thinning in several areas associated with the descending pain modulatory system, emotional evaluation of painful stimuli, and the lateral pain system, including the dorsolateral prefrontal cortex, orbitofrontal cortex, and posterior cingulate cortex.
Functional considerations
The concept of abnormal nociceptive input processing as an intrinsic part of PD gained support in the last 10 years owing to the very high prevalence of pain in PD, consistent demonstration of Lewy-type pathology in autonomic and pain system centres, both at supraspinal and spinal levels (Del Tredici and Braak, 2012), and intensified research testing the integrity of nociceptive pathways following stimulation of polymodal C-fibre (heat pain), or Aδ-fibre (CO2 laser, cold water, and electric stimuli) afferents, examined in PD patients
experiencing spontaneous pain or in pain-free conditions (Defazio et al., 2013 for review). Protocols have included quantitative sensory testing to measure subjective pain thresholds for different pain modalities, objective spinal cord pain thresholds through nociceptive flexor reflex (NFR) studies, as well as an experimental paradigm of heterotopic noxious conditioning stimulation to assess diffuse noxious inhibitory control (DNIC)-like effects (currently known as conditioned pain modulation). The functional status in cerebral structures part of the medial and lateral pain systems has also been assessed by a few research teams using evoked potentials and cerebral activation patterns with positron emission tomography. Differences in sample size, inclusion criteria, patient populations (disease stage, presence of pain or not), sensory modalities, and statistical analysis, have potentially contributed to produce some conflicting results, but key points may be drawn. No consistent relationship between peripheral nerve involvement and pain has been reported.
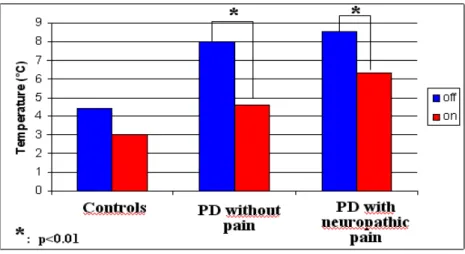
Previous experiments conducted in Toulouse repeatedly found reduced cold pain threshold in PD patients with or without pain, relative to matched controls (Brefel-Courbon et al., 2005, 2013). Similarly, reduction in multimodal pain thresholds has been documented in PD off-state, both in pain-free subjects and with pain (Defazio et al., 2013). In addition, spinal nociception with reduced NFR threshold to electrical stimuli was found to be altered in pain-free patients (Gerdelat-Mas et al., 2007) or with pain (Mylius et al., 2009), thereby raising the importance of the spinal level of signal integration. In one study, no alteration of the DNIC system was apparent in 15 PD patients (8 with pain) relative to controls (Mylius et al., 2009). These results strongly argue in favor of a genuine abnormality in nociceptive information processing in PD off-state predisposing to pain, and available evidence suggests either no difference or lower pain thresholds in PD patients with pain relative to pain-free subjects (Defazio et al., 2013). Levodopa normalized cold pain thresholds in PD patients with pain or pain-free (Brefel-Courbon et al., 2005, 2013) (Fig. 1).
Few protocols have used evoked potentials whereby CO2 laser stimulation of the skin Aδ fibres generates a negative N2 potential followed by a positive P2 response at vertex at a latency of approximately 200 and 300 ms, respectively. The origin and significance of these potentials remain uncertain, but available evidence implicates several brain structures involved in nociceptive input processing, such as the cingulate gyrus and insula (Tinazzi et al., 2008). PD patients and normal subjects showed comparable N2 and P2 latencies, whereas the N2/P2 peak-to-peak amplitude was significantly lower in PD patients (regardless of the clinically affected body side) than in controls. This has been interpreted as reflecting reduced inhibitory control. However, increased amplitude in PD patients with central pain has also been reported (Schestatsky et al., 2007). Methodological considerations and paucity of data do not allow drawing conclusive statements about the usefulness of scalp CO2 laser-evoked potentials in PD. Since levodopa administration yielded no change in N2/P2 amplitude as compared to the off state (Tinazzi et al., 2008), this may argue in favor of a preferential modulation of the spinal component of central nociceptive processing by amines.
Functional brain imaging with PET scanning is another sophisticated tool to address physiopathological mechanisms of abnormal pain perception in PD. In Toulouse, pain-induced activation profiles in cerebral structures have been examined following administration of H215O-PET to measure regional cerebral blood flow. Pain-free PD subjects OFF-levodopa showed overactivation in ipsilateral prefrontal cortex, ipsilateral insula, and contralateral anterior cingulate in comparison with normal subjects (Brefel-Courbon et al., 2005). Thus, both sensory discriminative processing of pain (insula/SII) as well as affective motivational processing of pain (anterior cingulate cortex, prefrontal cortex) are abnormal in PD. Interestingly, levodopa normalized the activation profiles. Subsequent work revealed distinct activation profiles in subjects with central pain relative to pain-free subjects, with overactivation of the medial pain system (emotional affective) in the former group, and
preferential activation of the lateral pain system (sensory discriminative) in the latter group (Brefel-Courbon et al., 2013) (Fig. 2). Levodopa improved the pain activation profiles in both systems. Since administration of the short-acting D1/D2 dopamine agonist apomorphine showed no effect on pain processing in PD nor any effect on pain threshold, other transmitters such as noradrenalin or serotonin could be implicated (Dellapina et al., 2011).
Another method of analysis addresses the correlates of chronic pain associated with PD using a functional magnetic resonance imaging-based approach to examine regional changes in spontaneous activity and the resting state signal coherence within the pain map regions of interest (Polli et al., 2016). Patients with or without pain were tested in the medicated “ON” state and compared to age-matched controls. Interestingly, decreased activity in the left orbitofrontal cortex was seen specifically in PD patients with pain, along with greater activity in the cerebellum and right inferior temporal areas. The pain group also showed a disconnected pattern of resting-state activity between the right nucleus accumbens and left hippocampus. Thus, accumulating brain imaging evidence supports the existence of morphological and dysfunctional regional changes in several cortical areas that could contribute to the development of chronic pain in PD, in addition to brainstem and spinal cord mechanisms.
Pain management in PD
Pharmacological approaches
Surveys on PD pain have suggested that it is a neglected and under-treated issue (Lee et al., 2006; Kim et al., 2013), with one-half of subjects receiving no treatment (Beiske et al., 2009). Individual preference for non-pharmacological approaches, reluctance to increase the pill
burden, fear of drug interactions, absence of disabling pain in many, and poor tolerability or response to analgesics, may hide behind such statistics. Efforts in diagnostic accuracy to distinguish nociceptive (musculoskeletal, dystonic) from neuropathic pain, and awareness of the taxonomy of PD pain and of central pain as a separate entity, should improve the pharmacological treatment of pain.
Pharmacological options have been reviewed previously (Perez-Lloret et al., 2012). Subsequently, the Verona group proposed an algorithm for the management of PD pain (Geroin et al., 2016). Based on physiopathology, we suggest that acetaminophen/paracetamol or anti-inflammatory drugs, and antiparkinsonian drugs (levodopa and dopamine agonists), would provide a beneficial effect on nociceptive pain, while opioids, levodopa, and gabapentinoids, would be more effective in central pain. Up to now, limited clinical trials carried out in PD pain have evaluated the effect of drugs on overall pain regardless of type. The RECOVER study (Trenkwalder et al., 2011) evaluating the motor effect of rotigotine (dopaminergic agonist) versus placebo in PD patients had pain as an exploratory criterion (evaluated on a Likert scale), which decreased in the rotigotine group. The results of the DOLORES study, a randomized controlled study evaluating the antalgic effect of rotigotine versus placebo in patients with PD pain, confirmed the results of the previous study, although the absolute improvement on the scale did not reach statistical significance between groups (Rascol et al., 2016). An opioid drug (oxycodone in combination with naloxone) has also been evaluated in PD patients with severe pain (Trenkwalder et al., 2015). This clinical trial demonstrated significant pain reduction in patients under oxycodone-naloxone at 4, 8, and 12 weeks, but not at 16 weeks. Beside these clinical trials, up to 45% of PD patients report less intense pain during the ON state (Stacy, 2010). One open-label study with duloxetine reported benefit in two-thirds of cases. Finally, Localized pain may be managed with botulinum toxin injections.
Non-pharmacological approaches
These approaches include deep brain stimulation, rehabilitation, and alternative medicine (Geroin et al., 2016). Severe dopamine denervation has a profound impact on subthalamo-pallidothalamic connections and motor control, which is normalized following deep brain stimulation (DBS) of the subthalamic nucleus in PD. This strategy has been convincingly shown to improve the pain experience in PD patients (Kim et al., 2008), reducing both the sensory and affective components of pain associated with the lateral and medial pain systems, respectively (Pellaprat et al., 2014), Interestingly, the level of pain alleviation did not correlate with improvement in motor score, mood, or changes in dopaminergic replacement therapy (Pellaprat et al., 2014), but was associated with raised pain thresholds in those DBS patients with pain (Dellapina et al., 2012). Functional cerebral imaging showed that deep brain stimulation of subthalamic nuclei could exert a direct effect by modulating the discriminatory lateral system in PD patients with pain (Dellapina et al., 2012). All pain types seem to benefit, dystonic pain in particular, and disability from low back pain is improved (Smith et al., 2015). Of note, unilateral pallidotomy also yielded lasting bilateral benefit on nociceptive (dyskinetic, dystonic, musculoskeletal) pain, beyond its effect on muscle rigidity (Honey et al., 1999). Pallidal DBS is also effective (Loher et al., 2002). These results suggest that changes in inhibitory outflow of the basal ganglia may modulate non-motor symptoms such as pain.
The contribution of spinal cord pathways to pain was raised from the experience of one PD patient with fluctuating severe leg pain in whom spinal anesthesia, but neither sympathetic nerve block nor epidural block, abolished the pain (Sage et al., 1990). Modulation of descending analgesia systems has been posited to explain the antinociceptive effect afforded
by STN DBS (Gee et al., 2016). Spinal cord stimulation at low thoracic level has also improved lower limbs pain in one PD patient (Fénelon et al., 2012). The procedure appears safe in individual patients with refractory pain.
Other approaches familiar to PD patients have been formally evaluated in a small number of subjects and found to benefit pain. These have included exercise-based programs, massage therapy, and acupuncture (Geroin et al., 2016). Exercise may contribute to reducing postural abnormalities and stiffness in part responsible for musculoskeletal pain, and growing evidence suggests that it may also recruit dopaminergic and non-dopaminergic (opioid, serotonin) pain inhibitory pathways (Allen et al., 2015). The potential impact of exercise on the neuroplasticity and neurorestoration along nociceptive pathways remains speculative. In one study (Reuter et al., 2011), different 6-month exercise programs reduced baseline pain level, particularly musculoskeletal pain, and pain regressed in 30% of participants. Pain relief in the back and extremities was better achieved with walking exercise compared to flexibility and relaxation sessions. These results definitely warrant further studies.
Conclusion
Pain is an increasingly recognized, intrinsic feature of PD and a topic of renewed interest in the last two decades. It is associated with overactivation in the medial pain system. PD patients, with or without pain, display lowered subjective sensory thresholds, which may rise with levodopa. For that reason, an attempt should be made at reducing levodopa-related response fluctuations and “off” time. Difficulties in classifying the various pains contribute to the challenge of studying and managing pain associated with PD. Indeed, the effects of treatment were assessed on pain in general, not accounting for the diversity of clinical pain charts in PD. It is likely that the different types of PD pain respond distinctly to treatment.
One of the most effective approaches in that regard is probably subthalamic nucleus stimulation. Depending on diagnosis, consultation with a physiotherapist, or alternative medicine approaches, may also be considered.
References
Allen, N.E., Moloney, N., van Vliet, V., Canning, C.G., 2015. The rationale for exercise in the management of pain in Parkinson’s disease. J. Parkinsons Dis. 5, 229-239.
Anagnostakis, Y., Zis, V., Spyraki, C., 1992. Analgesia induced by morphine injected into the pallidum. Behav. Brain Res. 48, 135-143.
Altier, N., Stewart J., 1999. The role of dopamine in the nucleus accumbens in analgesia. Life Sci. 65, 2269-2287.
Barnes, C.D., Fung, S.J., Adams, W.L., 1979. Inhibitory effects of substantia nigra on impulse transmission from nociceptors. Pain 6, 207-215.
Barone, P., Antonini, A., Colosimo, C., Marconi, R., Morgante, L., Avarello, T.P., Bottacchi, E., Cannas, A., Ceravolo, G., Ceravolo, R., Cicarelli, G., Gaglio, R.M., Giglia, R.M., Iemolo, F., Manfredi, M., Meco, G., Nicoletti, A., Pederzoli, M., Petrone, A., Pisani, A., Pontieri, F.E., Quatrale, R., Ramat, S., Scala, R., Volpe, G., Zappulla, S., Bentivoglio, A.R., Stocchi, F., Trianni, G., Del Dotto, P., PRIAMO study group , 2009. The PRIAMO study: a multicenter assessment of nonmotor symptoms and their impact on quality of life in Parkinson's disease. Mov. Disord. 24, 1641-1649.
Beiske, A.G., Loge, J.H., Rønningen, A., Svensson, E., 2009. Pain in Parkinson’s disease: prevalence and characteristics. Pain 141, 173–177.
Bonenfant, D., Rompré, P.H., Rei, N., Jodoin, N., Soland, V.L., Rey, V., Brefel-Courbon, C., Ory-Magne, F., Rascol, O., Blanchet, P.J., 2016. Characterization of Burning Mouth Syndrome in Patients with Parkinson's Disease. J. Oral Facial Pain Headache 30, 318-322. Borsook, D., Upadhyay, J., Chudler, E.H., Becerra, L., 2010. A key role of the basal ganglia in pain and analgesia: insights gained through human functional imaging. Molec. Pain 6, 27.
Brefel-Courbon, C., Grolleau, S., Thalamas, C., Bourrel, R., Allaria-Lapierre, V., Loï, R., Micallef Roll, J., Lapeyre-Mestre, M., 2009. Comparison of chronic analgesic drugs prevalence in Parkinson's disease, other chronic diseases and the general population. Pain 141, 14-18
Brefel-Courbon, C., Ory-Magne, F., Thalamas, C., Payoux, P., Rascol O., 2013. Nociceptive brain activation in patients with neuropathic pain related to Parkinson’s disease. Parkinsonism Relat. Disord. 19, 548–552.
Brefel-Courbon, C., Payoux, P., Thalamas, C., Ory, F., Quelven, I., Chollet, F., Montastruc, J.L., Rascol, O., 2005. Effect of levodopa on pain threshold in Parkinson’s disease: a clinical and positron emission tomography study. Mov. Disord. 20, 1557-1563.
Breivik, H ., Collett, B., Ventafridda, V., Cohen, R., Gallacher, D., 2006. Survey of chronic pain in Europe: prevalence, impact on daily life, and treatment. Eur . J . Pain 10, 287-333. Broen, M.P., Braaksma, M.M., Patijn, J., Weber, W.E., 2012. Prevalence of pain in Parkinson’s disease: a systematic review using the modified QUADAS tool. Mov. Disord. 27, 480–484.
Broetz, D., Eichner, M., Gasser, T., Weller, M., Steinbach, J.P., 2007. Radicular and nonradicular back pain in Parkinson’s disease: a controlled study. Mov. Disord. 22, 853–856. Buhmann, C., Wrobel, N., Grashorn, W., Fruendt, O., Wesemann, K., Diedrich, S., Bingel, U., 2017. Pain in Parkinson disease: a cross-sectional survey of its prevalence, specifics, and therapy. J. Neurol. 264, 758-769.
Burkey, A.R ., Carstens, E., Jasmin, L., 1999. Dopamine reuptake inhibition in the rostral agranular insular cortex produces antinociception. J. Neurosci. 19, 4169-4179.
Carey, R.J ., 1986. Acute ipsilateral hyperalgesia and chronic contralateral hypoalgesia after unilateral 6-hydroxydopamine lesions of the substantia nigra. Exp. Neurol. 91, 277-284.
Cenci, M.A ., Kalén, P., Mandel, R.J., Björklund, A., 1992. Regional differences in the regulation of dopamine and noradrenaline release in medial frontal cortex, nucleus accumbens and caudate-putamen: a microdialysis study in the rat. Brain Res. 581, 217-228.
Chaudhuri, K.R., Martinez-Martin, P., Brown, R.G., Sethi, K., Stocchi, F., Odin, P., Ondo, W., Abe, K., Macphee, G., Macmahon, D., Barone, P., Rabey, M., Forbes, A., Breen, K., Tluk, S., Naidu, Y., Olanow, W., Williams, A.J., Thomas, S., Rye, D., Tsuboi, Y., Hand, A., Schapira, A.H., 2007. The metric properties of a novel non-motor symptoms scale for Parkinson's disease: results from an international pilot study. Mov. Disord. 22, 1901-1911. Chaudhuri , K . R ., Rizos , A ., Trenkwalder , C ., Rascol , O ., Pal , S ., Martino , D ., Carroll , C ., Paviour , D ., Falup-Pecurariu , C ., Kessel , B ., Silverdale , M ., Todorova , A ., Sauerbier , A ., Odin , P ., Antonini , A ., Martinez-Martin , P ., EUROPAR and the IPMDS Non Motor PD Study Group, 2015. King's Parkinson's disease pain scale, the first scale for pain in PD: An international validation. Mov. Disord. 30, 1623-1631.
Chudler, E.H., Dong, W.K., 1995. The role of the basal ganglia in nociception and pain. Pain 60, 3–38.
Colloca, L., Ludman, T., Bouhassira, D., Baron, R., Dickenson, A.H., Yarnitsky, D., Freeman, R., Truini, A., Attal, N., Finnerup, N.B., Eccleston, C., Kalso, E., Bennett, D.L., Dworkin, R.H., Raja, S.N., 2017. Neuropathic pain. Nat. Rev. Dis. Primers 3, 17002.
Defazio, G., Berardelli, A., Fabbrini, G., Martino, D., Fincati, E., Fiaschi, A., Moretto, G., Abbruzzese, G., Marchese, R., Bonuccelli, U., Del Dotto, P., Barone, P., De Vivo, E., Albanese, A., Antonini, A., Canesi, M., Lopiano, L., Zibetti, M., Nappi, G., Martignoni, E., Lamberti, P., Tinazzi, M., 2008. Pain as a nonmotor symptom of Parkinson disease: evidence from a case-control study. Arch. Neurol. 65, 1191–1194.
Defazio, G., Gigante, A., Mancino, P., Tinazzi, M., 2013. The epidemiology of pain in Parkinson’s disease. J. Neural Transm. 120, 583–586.
Defazio, G., Berardelli, A., Fabbrini, G., Martino, D., Fincati, E., Fiaschi, A., Moretto, G., Abbruzzese, G., Marchese, R., Bonuccelli, U., Del Dotto, P., Barone, P., De Vivo, E., Albanese, A., Antonini, A., Canesi, M., Lopiano, L., Zibetti, M., Nappi, G., Martignoni, E., Lamberti, P., Tinazzi, M., 2008. Pain as a nonmotor symptom of Parkinson disease. Arch. Neurol. 65, 1191-1194.
Dellapina, E., Gerdelat-Mas, A., Ory-Magne, F., Pourcel, L., Galitzky, M., Calvas, F., Simonetta-Moreau, M., Thalamas, C., Payoux, P., Brefel-Courbon, C., 2011. Apomorphine effect on pain threshold in Parkinson’s disease: a clinical and positron emission tomography study. Mov. Disord. 26, 153–157.
Dellapina, E., Ory-Magne, F., Regragui,W., Thalamas, C., Lazorthes, Y., Rascol, O., Payoux, P., Brefel-Courbon, C., 2012. Effect of subthalamic deep brain stimulation on pain in Parkinson’s disease. Pain 153, 2267–2273.
Del Tredici, K., Braak, H., 2012. Spinal cord lesions in sporadic Parkinson’s disease. Acta Neuropathol. 124, 643-664.
Del Tredici, K., Braak, H., 2016. Review: Sporadic Parkinson's disease: development and distribution of α-synuclein pathology. Neuropathol. Appl. Neurobiol. 42, 33-50.
Ehrt, U., Larsen, J.P., Aarsland, D., 2009. Pain and its relationship to depression in Parkinson disease. Am. J. Geriatr. Psychiatry 17, 269-275.
Fénelon, G., Goujon, C., Gurruchaga, J.M., Cesaro, P., Jarraya, B., Palfi, S., Lefaucheur, J.P., 2012. Spinal cord stimulation for chronic pain improved motor function in a patient with Parkinson’s disease. Parkinsonism Relat. Disord. 18, 213–214.
Ford, B., 1998. Pain in Parkinson’s disease. Clin. Neurosci. 5, 63–72.
Ford, B., Louis, E.D., Greene, P., Fahn, S., 1996. Oral and genital pain syndromes in Parkinson’s disease. Mov. Disord. 11, 421-426.
Fox
, P . L ., Raina , P ., Jadad , A . R ., 1999. Prevalence and treatment of pain in older adults in nursing homes and other long-term care institutions: a systematic review. CMAJ. 160, 329-333.
Gao , D . M ., Jeaugey , L ., Pollak , P ., Benabid , A . L ., 1990. Intensity-dependent nociceptive responses from presumed dopaminergic neurons of the substantia nigra, pars compacta in the rat and their modification by lateral habenula inputs. Brain Res. 529, 315-319.
Gee, L.E., Walling, I., Ramirez-Zamora, A., Shin, D.S., Pilitsis, J.G., 2016. Subthalamic deep brain stimulation alters neuronal firing in canonical pain nuclei in a 6-hydroxydopamine lesioned rat model of Parkinson's disease. Exp. Neurol. 283(Pt A), 298-307.
Gerdelat-Mas, A., Simonetta-Moreau, M., Thalamas, C., Ory-Magne, F., Slaoui, T., Rascol, O., Brefel-Courbon, C., 2007. Levodopa raises objective pain threshold in Parkinson’s disease: a RIII reflex study. J. Neurol. Neurosurg. Psychiatry 78, 1140-1142.
Geroin, C., Gandolfi, M., Bruno, V., Smania, N., Tinazzi, M., 2016. Integrated approach for pain management in Parkinson disease. Curr. Neurol. Neurosci. Rep. 16, 28.
Goetz, C.G., Tanner, C.M., Levy, M., Wilson, R.S., Garron, D.C., 1986. Pain in Parkinson’s disease. Mov. Disord. 1, 45-49.
Gupta, Y.K., Chugh, A., Seth, S.D., 1989. Opposing effect of apomorphine on antinociceptive activity of morphine: a dose-dependent phenomenon. Pain 36, 263-269.
Hawkes, C.H., Del Tredici, K., Braak, H., 2010. A timeline for Parkinson's disease. Parkinsonism Relat. Disord. 16, 79-84.
Honey, C.R., Stoessl, A.J., Tsui, J.K., Schulzer, M., Calne, D.B., 1999. Unilateral pallidotomy for reduction of parkinsonian pain. J. Neurosurg. 91, 198–201.
Jurna, I., Heinz, G., Blinn, G., Nell, T., 1978. The effect of substantia negra stimulation and morphine on alpha-motoneurones and the tail-flick response. Eur. J. Pharmacol. 51, 239-250.
Kanda, T., Tsukagoshi, H., Oda, M., Miyamoto, K., Tanabe, H., 1996. Changes of unmyelinated nerve fibers in sural nerve in amyotrophic lateral sclerosis, Parkinson’s disease and multiple system atrophy. Acta Neuropathol. 91, 145-154.
Kim, H.J., Paek, S.H., Kim, J.Y., Lee, J.Y., Lim, Y.H., Kim, M.R., Kim, D.G., Jeon, B.S., 2008. Chronic subthalamic deep brain stimulation improves pain in Parkinson disease. J. Neurol. 255, 1889–1894.
Kim, Y.E., Lee, W.W., Yun, J.Y., Yang, H.J., Kim, H.J., Jeon, B.S., 2013. Musculoskeletal problems in Parkinson’s disease: neglected issues. Parkinsonism Relat. Disord. 19, 666–669. Kirkby, R.J ., Kimble, D.P., 1968. Avoidance and escape behavior following striatal lesions in the rat. Exp. Neurol. 20, 215-227.
Koyama, T., Kato, K., Mikami, A., 2000. During pain-avoidance neurons activated in the macaque anterior cingulate and caudate. Neurosci. Lett. 283, 17-20.
Kumakura, Y., Danielsen, E.H., Gjedde, A., Vernaleken, I., Buchholz, H.G., Heinz, A., Gründer, G., Bartenstein, P., Cumming, P., 2010. Elevated [18F]FDOPA utilization in the periaqueductal gray and medial nucleus accumbens of patients with early Parkinson's disease. NeuroImage 49, 2933-2939.
Lee, M.A., Walker, R.W., Hildreth, T.J., Prentice, W.M., 2006. A survey of pain in idiopathic Parkinson’s disease. J. Pain Symptom. Manag. 32, 462–469.
Li,
J ., Ji, Y.P., Qiao, J.T., Dafny, N., 1992. Suppression of nociceptive responses in parafascicular neurons by stimulation of substantia nigra: an analysis of related inhibitory pathways. Brain Res. 591, 109-115.
Lin, C.H., Wu, R.M., Chang, H.Y., Chiang, Y.T., Lin, H.H., 2013. Preceding pain symptoms and Parkinson's disease: a nationwide population-based cohort study. Eur. J. Neurol. 20, 1398-1404.
Loher, T.J., Burgunder, J.M., Weber, S., Sommerhalder, R., Krauss, J.K., 2002. Effect of chronic pallidal deep brain stimulation on off period dystonia and sensory symptoms in advanced Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 73, 395–399.
Mantz, J ., Thierry, A.M., Glowinski, J., 1989. Effect of noxious tail pinch on the discharge rate of mesocortical and mesolimbic dopamine neurons: selective activation of the mesocortical system. Brain Res. 476, 377-381.
Morgan, M.J., Franklin, K.B.J., 1990. 6-hydroxydopamine lesions of the ventral tegmentum abolish D-amphetamine and morphine analgesia in the formalin test but not in the tail flick test. Brain Res. 519, 144-149.
Morgan, M.J., Franklin, K.B.J., 1991. Dopamine receptor subtypes and formalin test analgesia. Pharm. Biochem. Behav. 40, 317-322.
Mylius, V., Engau, I., Teepker, M., Stiasny-Kolster, K., Schepelmann, K., Oertel, W.H., Lautenbacher, S., Möller, J.C., 2009. Pain sensitivity and descending inhibition of pain in Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 80, 24–28.
Nègre-Pagès, L., Regragui, W., Bouhassira, D., Grandjean, H., Rascol, O., DoPaMiP Study Group, 2008. Chronic pain in Parkinson’s disease: the cross-sectional French DoPaMiP survey. Mov. Disord. 23, 1361–1369.
Nolano, M., Provitera, V., Estraneo, A., Selim, M.M., Caporaso, G., Stancanelli, A., Saltalamacchia, A.M., Lanzillo, B., Santoro, L., 2008. Sensory deficit in Parkinson’s disease: evidence of a cutaneous denervation. Brain 131(Pt 7), 1903-1911.
Nolano, M., Provitera, V., Manganelli, F., Iodice, R., Stancanelli, A., Caporaso, G., Saltalamacchia, A., Califano, F., Lanzillo, B., Picillo, M., Barone, P., Santoro, L., 2017. Loss of cutaneous large and small fibers in naïve and l-dopa-treated PD patients. Neurology 89, 776-784.
O'Sullivan, S.S., Williams, D.R., Gallagher, D.A., Massey, L.A., Silveira-Moriyama, L., Lees, A.J., 2008. Nonmotor symptoms as presenting complaints in Parkinson's disease: a clinicopathological study. Mov. Disord. 23, 101-106.
Paolucci, S., Iosa, M., Toni, D., Barbanti, P., Bovi, P., Cavallini, A., Candeloro, E., Mancini, A., Mancuso, M., Monaco, S., Pieroni, A., Recchia, S., Sessa, M., Strambo, D., Tinazzi, M., Cruccu, G., Truini, A.; Neuropathic pain special interest group of the Italian Neurological Society, 2016. Prevalence and time course of post-stroke pain: A multicenter prospective hospital-based study. Pain Med. 17, 924-930.
Pellaprat, J., Ory-Magne, F., Canivet, C., Simonetta-Moreau, M., Lotterie, J.A., Radji, F., Arbus, C., Gerdelat, A., Chaynes, P., Brefel-Courbon, C., 2014. Deep brain stimulation of the subthalamic nucleus improves pain in Parkinson’s disease. Parkinsonism Relat. Disord. 20, 662–664.
Perez-Lloret, S., Rey, M.V., Dellapina, E., Pellaprat, J., Brefel-Courbon, C., Rascol, O., 2012. Emerging analgesic drugs for Parkinson’s disease. Expert Opin. Emerg. Drugs 17, 157–171. Perez-Lloret, S., Ciampi de Andrade, D., Lyons, K.E., Rodríguez-Blázquez, C., Chaudhuri, K.R., Deuschl, G., Cruccu, G., Sampaio, C., Goetz, C.G., Schrag, A., Martinez-Martin, P., Stebbins, G., the members of the MDS committee on rating scales development, 2016. Rating scales for pain in Parkinson’s disease: critique and recommendations. Mov. Disord. Clin. Pract. 3, 1-11. DOI: 10.1002/mdc3.12384
Polli, A., Weis, L., Biundo, R., Thacker, M., Turolla, A., Koutsikos, K., Chaudhuri, K.R., Antonini, A., 2016. Anatomical and functional correlates of persistent pain in Parkinson’s disease. Mov. Disord. 31, 1854-1864.
Pont-Sunyer, C., Hotter, A., Gaig, C., Seppi, K., Compta, Y., Katzenschlager, R., Mas, N., Hofeneder, D., Brücke, T., Bayés, A., Wenzel, K., Infante, J., Zach, H., Pirker, W., Posada, I.J., Álvarez, R., Ispierto, L., De Fàbregues, O., Callén, A., Palasí, A., Aguilar, M., Martí,
M.J., Valldeoriola, F., Salamero, M., Poewe, W., Tolosa, E., 2015. The onset of nonmotor symptoms in Parkinson's disease (the ONSET PD study). Mov. Disord. 30, 229-237.
Quinn, N.P., Koller, W.C., Lang, A.E., Marsden, C.D., 1986. Painful Parkinson’s disease. Lancet 1(8494), 1366-1369.
Rascol, O., Zesiewicz, T., Chaudhuri, K.R., Asgharnejad, M., Surmann, E., Dohin, E., Nilius, S., Bauer, L., 2016. A randomized controlled exploratory pilot study to evaluate the effect of rotigotine transdermal patch on Parkinson's disease-associated chronic pain. J. Clin. Pharmacol. 56, 852-861.
Reichling, D.B., Levine, J.D., 2011. Pain and death: neurodegenerative disease mechanisms in the nociceptor. Ann. Neurol. 69, 13-21.
Reuter, I., Mehnert, S., Leone, P., Kaps, M., Oechsner, M., Engelhardt, M., 2011. Effects of a flexibility and relaxation programme, walking, and Nordic walking on Parkinson’s disease. J. Aging Res. 2011, 232473.
Riley, D., Lang, A.E., Blair, R.D.G., Birnbaum, A., Reid, B., 1989. Frozen shoulder and other shoulder disturbances in Parkinson’s disease. J. Neurol. Neurosurg. Psychiat. 52, 63-66. Rüb, U., Del Tredici, K., Schultz, C., Ghebremedhin, E., de Vos, R.A., Jansen Steur, E., Braak, H., 2002. Parkinson's disease: the thalamic components of the limbic loop are severely impaired by alpha-synuclein immunopositive inclusion body pathology. Neurobiol. Aging 23, 245-254.
Russmann, H., Vingerhoets, F., Ghika, J., Maeder, P., Bogousslavsky, J., 2003. Acute infarction limited to the lenticular nucleus: clinical, etiologic, and topographic features. Arch. Neurol. 60, 351-355.
Saadé, N.E., Atweh, S.F., Bahuth, N.B., Jabbur, S.J., 1997. Augmentation of nociceptive reflexes and chronic deafferentation pain by chemical lesions of either dopaminergic terminals or midbrain dopaminergic neurons. Brain Res. 751, 1-12.
Sage, J.I., Kortis, H.I., Sommer, W., 1990. Evidence for the role of spinal cord systems in Parkinson’s disease-associated pain. Clin. Neuropharmacol. 13, 171-174.
Schestatsky, P., Kumru, H.,Valls-Solé, J., Valldeoriola, F., Marti, M.J., Tolosa, E., Chaves, M.L., 2007. Neurophysiologic study of central pain in patients with Parkinson disease. Neurology 69:2162–2169.
Sigwald, J., Solignac, J., 1960. Manifestations douloureuses de la maladie de Parkinson et paresthésies provoquées par les neuroleptiques. Sem. Hôp. Paris 40-41, 2222-2225.
Smith, H., Gee, L., Kumar, V., Ramirez-Zamora, A., Durphy, J., Hanspal, E., Barba, A., Molho, E., Shin, D., Pilitsis, J.G., 2015. Deep brain stimulation significantly decreases disability from low back pain in patients with advanced Parkinson's disease. Stereotact. Funct. Neurosurg. 93, 206-211.
Souques, M.A., 1921. Des douleurs dans la paralysie agitante. Rev. Neurol. 37, 629-633. Stacy, M., 2010. The wearing-off phenomenon and the use of questionnaires to facilitate its recognition in Parkinson’s disease. J. Neural Transm. 117, 837–846.
Stamey, W., Davidson, A., Jankovic, J., 2008. Shoulder pain: a presenting symptom of Parkinson disease. J. Clin. Rheumatol. 14, 253-254.
Starkstein, S. E., Preziosi, T.J., Robinson, R.G., 1991. Sleep disorders, pain, and depression in Parkinson’s disease. Eur. Neurol. 31, 352–355.
Takeda, R., Ikeda, T., Tsuda, F., Abe, H., Hashiguchi, H., Ishida, Y., Nishimori, T., 2005. Unilateral lesions of mesostriatal dopaminergic pathway alters the withdrawal response of the rat hindpaw to mechanical stimulation. Neurosci. Res. 52, 31-36.
Tinazzi, M., Del Vesco, C., Defazio, G., Fincati, E., Smania, N., Moretto, G., Fiaschi, A., Le Pera, D., Valeriani, M., 2008. Abnormal processing of the nociceptive input in Parkinson’s disease: a study with CO2 laser evoked potentials. Pain 136, 117–124.
Trenkwalder, C., Kies, B., Rudzinska, M., Fine, J., Nikl, J., Honczarenko, K., Dioszeghy, P., Hill, D., Anderson, T., Myllyla, V., Kassubek, J., Steiger, M., Zucconi, M., Tolosa, E., Poewe, W., Surmann, E., Whitesides, J., Boroojerdi, B., Chaudhuri, K.R., Recover Study Group, 2011. Rotigotine effects on early morning motor function and sleep in Parkinson's disease: a double-blind, randomized, placebo-controlled study (RECOVER). Mov. Disord. 26, 90-99.
Trenkwalder, C., Chaudhuri, K.R., Martinez-Martin, P., Rascol, O., Ehret, R., Vališ, M., Sátori, M., Krygowska-Wajs, A., Marti, M.J., Reimer, K., Oksche, A., Lomax, M., DeCesare, J., Hopp, M., PANDA study group, 2015. Prolonged-release oxycodone-naloxone for treatment of severe pain in patients with Parkinson's disease (PANDA): a double-blind, randomised, placebo-controlled trial. Lancet Neurol. 14, 1161-1170.
Valkovic, P., Minar, M., Singliarova, H., Harsany, J., Hanakova, M., Martinkova, J., Benetin, J., 2015. Pain in Parkinson’s disease: A cross-sectional study of its prevalence, types, and relationship to depression and quality of life. PLoS ONE 10(8), e0136541.
Verhaak, P.F., Kerssens, J.J., Dekker, J., Sorbi, M.J., Bensing, J.M., 1998. Prevalence of chronic benign pain disorder among adults: a review of the literature. Pain 77, 231–239. Wasner, G., Deuschl, G., 2012. Pains in Parkinson disease: many syndromes under one umbrella. Nat. Rev. Neurol. 8, 284-294.
White, I.M., Rebec, G.V ., 1993. Responses of rat striatal neurons during performance of a lever-release version of the conditioned avoidance response task. Brain Res. 616, 71-82.
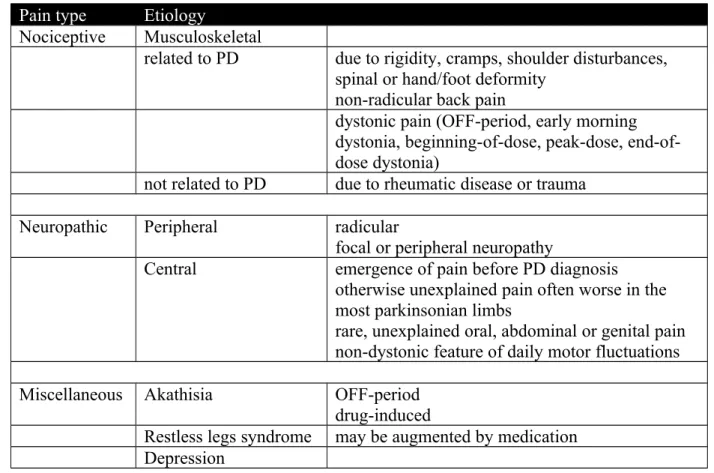
Table 1. Classification of parkinsonian pain (after Ford, 1998).
Pain type Etiology
Nociceptive Musculoskeletal
related to PD due to rigidity, cramps, shoulder disturbances, spinal or hand/foot deformity
non-radicular back pain
dystonic pain (OFF-period, early morning dystonia, beginning-of-dose, peak-dose, end-of-dose dystonia)
not related to PD due to rheumatic disease or trauma
Neuropathic Peripheral radicular
focal or peripheral neuropathy
Central emergence of pain before PD diagnosis
otherwise unexplained pain often worse in the most parkinsonian limbs
rare, unexplained oral, abdominal or genital pain non-dystonic feature of daily motor fluctuations
Miscellaneous Akathisia OFF-period
drug-induced
Restless legs syndrome may be augmented by medication Depression
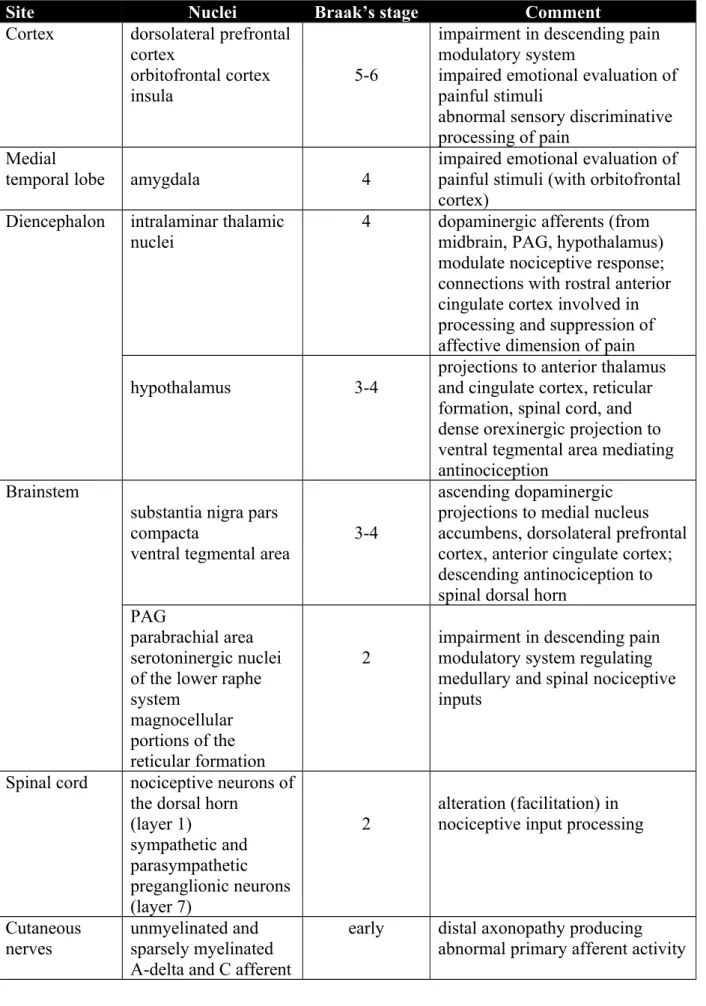
Table 2. Lewy-body pathology potentially contributing to parkinsonian pain.
Site Nuclei Braak’s stage Comment
Cortex dorsolateral prefrontal cortex
orbitofrontal cortex insula
5-6
impairment in descending pain modulatory system
impaired emotional evaluation of painful stimuli
abnormal sensory discriminative processing of pain
Medial
temporal lobe amygdala 4
impaired emotional evaluation of painful stimuli (with orbitofrontal cortex)
Diencephalon intralaminar thalamic nuclei
4 dopaminergic afferents (from midbrain, PAG, hypothalamus) modulate nociceptive response; connections with rostral anterior cingulate cortex involved in processing and suppression of affective dimension of pain
hypothalamus 3-4
projections to anterior thalamus and cingulate cortex, reticular formation, spinal cord, and dense orexinergic projection to ventral tegmental area mediating antinociception
Brainstem
substantia nigra pars compacta
ventral tegmental area
3-4
ascending dopaminergic projections to medial nucleus accumbens, dorsolateral prefrontal cortex, anterior cingulate cortex; descending antinociception to spinal dorsal horn
PAG
parabrachial area serotoninergic nuclei of the lower raphe system
magnocellular portions of the reticular formation
2
impairment in descending pain modulatory system regulating medullary and spinal nociceptive inputs
Spinal cord nociceptive neurons of the dorsal horn
(layer 1) sympathetic and parasympathetic preganglionic neurons (layer 7) 2 alteration (facilitation) in nociceptive input processing
Cutaneous
nerves unmyelinated and sparsely myelinated A-delta and C afferent
early distal axonopathy producing abnormal primary afferent activity
fibres to dorsal horn neurons (layer 1)
Figure 1 : Assessment of cold pain threshold in OFF and ON conditions in PD patients and controls
Figure 2
Figure 2 : Cold pain-induced activation corresponding to regional cerebral blood flow increases, in PD patients with