Digitized
by
the
Internet
Archive
in
2011
with
funding
from
Boston
Library
Consortium
Member
Libraries
11
I
UbWEY
Massachusetts
Institute
of
Technology
Department
of
Economics
Working Paper
Series
COUNTERVAILING
POWER
IN
WHOLESALE PHARMACEUTICALS
Sara
F.
Ellison
Christopher
M.
Snyder
Working
Paper
01
-27
July
2001
Room
E52-251
50
Mennorial
Drive
Cambridge,
MA
02142
This
paper
can
be
downloaded
without
charge from
the
Social
Science
Research Network
Paper
Collection
at
Massachusetts
Institute
of
Technology
Department
of
Economics
Working Paper
Series
COUNTERVAILING
POWER
IN
WHOLESALE PHARMACEUTICALS
Sara
F.
Ellison
Christopher M.
Snyder
Working
Paper
01
-27
July
2001
Room
E52-251
50
Memorial
Drive
Cambridge,
MA
02142
This
paper
can be
downloaded
without
charge from
the
Social
Science
Research Network
Paper
Collection
at
Countervailing
Power
in
Wholesale
Pharmaceuticals
Sara
Fisher Ellison ChristopherM.
Snyder
M.I.T.
George
Washington
UniversityJuly 19,
2001
Abstract: There
are anumber
of theories in the industrial organization literature explaining the conventionalwisdom
thatlargerbuyersmay
have
more
"countervailingpower"
than small buyers,in that they receive
lower
pricesfrom
suppliers.We
test the theories empirically using dataon
wholesale
pricesfor antibiotics soldthrough variousdistributionchannels—
chainand independent
drugstores, hospitals,
HMOs
—
in the U.S. during the 1990s. Price discountsdepend
more on
theability to substitute
among
alternative suppliers thanon
sheerbuyer
size. In particular, hospitalsand
HMOs,
which
can
use restrictive formularies toenhance
their substitution opportunitiesbeyond
those available for drugstores, obtain substantiallylower
prices.Chain
drugstores only receive a small size discount relative to independents, atmost
two
percenton
average,and
then onlyforproducts forwhich
drugstoreshave
some
substitution opportunities(i.e., notforon-patentbranded
drugs).Our
findings areroughly
consistent with collusionmodels
of countervailingpower
and
inconsistent with bargainingmodels and have
implications for recentgovernment
proposals to
form
purchasing
alliances to reduce prescription costs.JEL
Codes:
L43, L65,
D43,
C78
Ellison:
Department
ofEconomics,
M.I.T.,50
Memorial
Drive,Cambridge,
MA
02142;
tel. (617)253-3821;
fax. (617)253-1330;
email sellison@mit.edu. Snyder:Department
ofEconomics,
George
Washington
University,2201
G
StreetN.W., Washington
DC
20052,
tel. (202)994-6581,
fax. (202)994-6147,
emailcmsnyder@gwu.edu.
Ellison thanks theHoover
Institutionand
the Eli Lilly grant to theNBER
for support.Snyder
thanksMIT
and
theRSSS
at the Australian National University for support.The
authors are grateful for helpfulcomments from
Maura
Doyle,Glenn
Ellison,Werner
Guth, Margaret
Kyle,Wallace
Mullin, Ariel Pakes, LarsStole,JeffreyZwiebel,
and seminar
participants attheUniversity of Adelaide, Australian National1
Introduction
Galbraith (1952) suggested that large buyers
have
anadvantage
in extracting price concessionsfrom
suppliers.He
called thiseffectthecountervailingpower
oflarge buyersbecause
he foresaw
it as countervailingthe
market
power
oflarge suppliers. It haslong been
the conventionalwisdom
in the business press that
such
a buyer-size effectexists.'The
conventionalwisdom
was
recentlyin evidence in the
enthusiasm
over collectivepurchasing
websites, thebest-known
ofwhich
was
Mercata,
which
sold items at a pricewhich
declined asmore
customers
signedup
to purchase.As
a columnistwrote soon
afterMercata'
s launch:It's an old idea:
Round
up
abunch
ofpeople
who
promise
tobuy
an itemand
thengo
to themanufacturer
or distributorand
work
out avolume
discount.But add
theInternet, with millions of potential
customers
and
the ability tomodify
prices everysecond,
and
you've
got themakings
of a dramatic transformationin retailing(Boston
Globe, July 11, 1999).
The
subsequent
closureofMercata and
failure of other similar business ventures(MobShop,
LetsBuylt) suggests the
importance
ofunderstanding the sources of buyer-size effects ratherthansimply
accepting theconventionalwisdom
thatsuch
effects exist.The
economics
literature offersa
number
oftheorieson
thesources of buyer-sizeeffects.The
theoriescan
be roughly
dividedintotwo
categories, those involving amonopoly
supplierand
those involvingcompeting
suppliers.^The
first category includesmodels
inwhich
themonopoly
supplier bargains with buyersunder
symmetric
information as inHorn
and
Wolinsky
(1988), Stoleand Zwiebel
(1996b),Chipty
and Snyder
(1999),and
Chae
and Heidhues
(1999a,1999b)
and
inwhich
itmakes
take-it-or-'See, e.g., an article on the power of large cable operators to extract price discounts from program suppliers
(Cablevision, February 1, 1988), an article on thepower ofWal-Marttoextract price discountsfrommanufacturers
{The Guardian (London), July 25, 2000), and thescore ofother business press sources exhibiting the conventional
wisdomcited inScherer andRoss (1990) and Snyder (1998).
^Whilethiscategorizationcapturesthe theories thatturnouttoberelevanttoourparticularempirical application,
itis not exhaustive. The technology ofwarehousing and distribution
may
be such that largebuyers arecheaper tosupply perunit thansmall, inwhich caselargebuyers wouldbeexpected topaylowerprices than smallfor a broad
range ofsuppliermarketstructures (see, e.g.,Lottand Roberts 1991 andLevy 1999). Size discounts in Katz(1987)
and Scheffman and Spiller (1992) can be thought ofas involving potential supplier competition, arising from the threat ofbackward integration by a largebuyer.
leave-it offers
under asymmetric
information as inMaskin
and
Riley (1984).The
models
sharethe
common
implication that there exist conditionsunder
which
buyer-size discountsemerge
inequilibrium with a
monopoly
supplier.The
second
category suggests that competitionamong
suppliers
may
be
crucial for the buyer-size effect to emerge. In thesupergame
framework
ofSnyder
(1996, 1998), tacitly-colluding supplierscompete
more
aggressively for the business oflarge buyers
and
are forced to chargelower
prices to large buyers to sustain collusion.Buyer-size discounts
do
notemerge
with amonopoly
supplier but rather require multiplecompeting
suppliers.
The
two
classes of theories, insum, have
contrasting implications forwhether
thebuyer-size effect
emerges even
with amonopoly
supplier (as in the first class) orwhether
instead thebuyer-size effect only
emerges
if buyers are able to substituteamong
competing
suppliers (asin the
second
class).These
contrasting implications provide the basis of the empirical testswe
conduct
in thispaper
using datafrom
the pharmaceutical industry. In particular,we
studywholesale prices
charged
by
pharmaceuticalmanufacturers
to various buyers including chaindrugstores,
independent
drugstores, hospitals,and
healthmaintenance
organizations(HMOs)
forantibiotics.
Our
data provide aunique
opportunity to test the theories sincewe
observe
buyersof different sizes
—
chain drugstores are larger than independents—
purchasing
drugs providing different substitution opportunities.At
one
extreme, drugstorescannot
substituteaway
from
adrug produced
by
abranded manufacturer
withan unexpired
patent; insuch
markets, drugstoreseffectively face a
monopoly
supplier.At
the other extreme,once
a patent expireson
adrug
and
several generic manufacturers enter, drugstorescan
freely substituteamong
thecompeting
generics.
Another
source of variance in our datais in the substitution opportunities acrossbuyers.By
issuing restrictive formularies, hospitalsand
HMOs
can
controlwhich
drugs
their affiliateddoctors prescribe, effectively allowing their
purchasing
managers
to substituteamong
branded
drugs with similarindications fordrugs
on
patentand between branded and
generic manufacturersamong
multiple genericmanufacturers
and
insome
states can substitutebetween branded and
generics for off-patent drugs, but otherwise
need
to fill the prescriptions theircustomers
bringin as written.
Using
these sources of variation,we
can
identify instances inwhich
buyershave
good
substitition opportunities, large size, both, or neither,and can
therefore isolate the effectthat
each
hason purchase
price.While
we may
have an academic
interestin the sources of countervailingpower
and
may
have
been
fortunate that the pharmaceutical industry provides agood
setting to explore theacademic
question,
our
findings about countervailingpower
in pharmaceuticalshave
policy implications aswell.
The
U.S. federalgovernment
and
individual stateshave designed
anumber
ofbills with thegoal of reducing prescription
drug
costsby
aggregating buyers intolarge health careprocurement
alliances.
At
the federal level, a core proposition of the Clinton health carereform
planwas
that large savings
would
come
from
the formation ofbuyer
alliances{White
House
Domestic
Policy
Council
1993).More
recently, alaw
enacted inMaine
was
based
on
the idea that thecountervailing
power
of an intrastate alliancewould
reduce drug
costs.Maine
Governor
Angus
King
stated:If the [pharmaceutical] industry
can
consolidateand
increase itsmarket power,
socan
we.
We're
going
to bargainon
behalf of50
percent ofour
citizensand
we
think that they deserve thesame
consideration as other groups that get discountsbased
on
their
volume
{New
York
Times,May
12, 2000).Other
stateshave
considered similar legislation or are taking part in discussions about interstatepurchasing
alliances.^The
success ofsuch
proposalssucceeding
hingeson
the nature ofcoun-tervailing
power.
Ifsize alone is not sufficient forcountervailingpower
but suppliercompetitionis also required,
forming
large alliancesmay
not result in substantiallylower
prices unless thepurchasing
manager
can
induce supplier competitionby
being willing to substituteone drug
for'lowa.
New
Hampshire, Washington and West Virginia have created intrastate purchasing cooperatives for theelderly. Vermont and Maryland have considered similar programs to Maine's {New York Times, April 23, 2001).
WestVirginia, Georgia, North Carolina, South Carolina,
New
Mexico, and Washington collaboratedon a multistateanother.
Consumers
may
oppose
the resulting restriction of choice(similar to themuch-publicized
dissatisfaction with the restriction of choice
and
careby
HMOs),
as noted in the following storyabout a congressional inquiry into the cost savings
from
jointprocurement
by
theDepartment
ofDefense
and
Veterans Administration:'The
driving expectation is that, as thetwo
agenciesbuy
more
ofa particular drug,their leverage . . . will permit
them
to exact discountsfrom
drug
manufacturers,' thereport said.
VA
and Defense
officials said the auditdoes
not take into accountsome
negative consequences, including the likelihood that a joint contract with a single
drug
maker
might
forcemany
patients tochange
medications{Boston
Globe, July 5, 2000).Our
resultsshow
that largebuyers
(chain drugstores) receiveno
discount relative to smallbuyers (independent drugstores)
on
antibiotics with unexpired patents—
antibiotics forwhich
drugstores
have
no
substitution opportunitiesand
thus effectively facemonopoly
suppliers.For
off-patent antibiotics
—
antibiotics forwhich
drugstoreshave
some
substitution opportunites—
chain drugstores receive a statistically significant but small discount relative to independents,
at
most
2%.
Much
larger discounts areobserved
in thecomparison
of hospitalsand
HMOs
to drugstores.While
it is unclearwhether
hospitalsand
HMOs
can
be
characterized asbeing
largeror smaller than drugstores
on
average, it is clear that theyhave
better substitution opportunitiesdue
to their use of restrictive formularies. Hospitals'and
HMOs'
discounts are asmuch
as athird
on
branded
drugs thathave
expiredpatents.These
aredrugs forwhich
hospitalsand
HMOs
can
substitute generics freely; drugstorescan
do
so only to amore
limited extent. Hospitalsand
HMOs
receive discounts of asmuch
as10%
forbranded
drugs with unexpired patents,presumably because
theycan
use the abilitytopurchase
a therapeuticallysimilar substitutewhile
drugstores cannot.
The
implication of our findings foreconomic
theory is that, at least for the wholesalean-tibiotics market,
models
focusingon
competitionamong
suppliers (e.g.Snyder
1996,1998)
areStole
and Zwiebel 1996b; Chipty and Snyder
1999;Chae
and Heidhues
1999a,1999b)
or othermodels
involving amonopoly
supplier(Maskin
and
Riley 1984).The
implication ofour
findingsfor policy is that absent the ability to
be
restrictive,drug purchasing
alliances are not likely togain
much
from
their increased size."*The
fact that hospitalsand
HMOs
receive substantial discounts relative to drugstores is wellknown.
Indeed, the discountswere
the focus ofa high-profile antitrust case in the 1990s.^Our
results
go
beyond
merely
documenting
the presence ofhospital/HMO
discounts:we
provide formal estimates of themagnitude
ofthe discounts,an
analysis ofhow
the discounts vary withthe
market
structure of suppliers, ameasure
of the discountsdue
tobuyer
size alone,and
acomparison
ofthe relativeimportance
ofthe various effects.Our
paper
is part of a larger empirical literaturedocumenting
the existence of buyer-sizeeffects
and
countervailing power.The
literature includes case studies,^ interindustryeconometric
studies,^
and
intraindustryeconometric
studies.^While
these papersdocument
the existence abuyer-size effect, they
do
not provide amore nuanced
test of the sources of those effects, aswe
do.
There
is also a related literatureon
bargainingbetween
buyersand
suppliers in health caremarkets.^
The
focus ofmuch
of this literature is the welfare effects of themonopsony
power
of insurers.
Two
exceptions are CongressionalBudget
Office (1998)and Sorensen
(2001).The
CBO
studieshow
ameasure
ofbuyer
discounts (thedifferencebetween
the lowest price received ''An alternative isfor states simplytoregulate drugprices ratherthan engage in voluntarynegotiations. Indeed,theMainelawcitedabovehasaprovisiontriggeringpricecontrolsifgrouppurchasing doesnotresult insubstantially lower prices. See Dranove and Cone (1985)for a study ofthe effect ofprice regulation on hospital costs.
^SeetheNovember 1997symposiumontheBrand
Name
PrescriptionDrugsAntitrust Litigationin theNovember 1997 issueofthe International Journal oftheEconomics ofBusiness (Freeh, ed., 1997).*See Adeiman (1959) and
McKie
(1959).''See Brooks (1973); Porter (1974); Buzzell, Gale, and Sultan (1975); Lustgarten (1975);
McGuckin
and Chen(1976); Clevengerand Campbell (1977); LaFrance (1979); Martin (1983); and Boulding and Staelin (1990).
^Chipty (1995) findsthat largecable operatorschargelowerprices tosubscribers,possiblyreflectinglowerinput
pricespaid toprogram suppliers.
'See Pauly (1987, 1998); Staten, Dunkelberg, and
Umbeck
(1987); Melnick et al. (1992); Brooks, Dor, andby
any non-government
buyer, reportedunder
theMedicaid
drug
rebateprogram,
and
the averageprice offered to drugstores) varies with the presence of substitution opportunities.
Our
datahave
the virtue of allowing us to identifywhich
type ofbuyer
received the discountsand
thepervasiveness of the discounts
on
average foreach
type of buyer, rather than a single reportedextreme.
More
importantly, there isno
informationon
buyer
size in theCBO
data, so theycannot conduct
the tests involving buyer-size discounts,one
of themain
focuses of our study.The
closestpaper
to ours is concurrent researchby
Sorensen
(2001).His
objective, as is ours,is totest
among
various theories of countervailingpower.
His
results arebroadly consistent withours
though
for a different class of health care expenditure: hospital services.He
findssome
evidence
that large insurers obtain discounts for hospital services, but the size effect is small.More
significantis thediscount obtainedby
insurancecompanies
that are able tochannel
patientsto lower-priced hospitals. In both
our
paper
and Sorensen
(2001), substitution opportunities area
more
important source of countervailingpower
than sheer size.One
difference isour
findingofan interaction
between
sizeand
substitution opportunities,an
interactionwhich
is insignificantin
Sorensen
(2001);however,
themagnitude
ofthe interaction effect inour
results is small.This
detail aside, our papers
can
be
viewed
asbeing
complementary,
providingsome
comfort
in therobustness of the results
and
their applicabilitybeyond
the particularmarket
studied in eitherpaper
individually.Finally, there is an experimental
paper
of relevance. Ruffle(2000)
shows
that larger buyersare
more
likely to use a strategy ofdemand
withholding
to extractlower
prices in a repeatedposted-offer market.
Our
paper
is also part of the literatureon
pharmaceuticals, specifically pharmaceuticalpric-ing.'*'
The
most
closely relatedpaper
on
pharmaceutical pricing isMoore
and
Newman
(1993),one
ofafew
studies oftheeconomic
effects ofrestrictive forrnularies."They
find that restrictive'°See,e.g..Caves,Whinston, andHurwitz(1991);Grabowski and Vernon(1992);Grilichesand
Cockbum
(1994);Baye, Maness, andWiggins (1997); Ellisonet al. (1997);Scott Morton (1997); and Ellison and Wolfram (2000).
formularies
lower
retail expenditureson
drugs butdo
notlower
overall health care expendituresbecause
of input substitution.Our
finding that restrictive formulariesappear
to allow hospitalsand
HMOs
to extract price concessions is related, but our analysis is at thewholesale
ratherthanretail level.
2
Background
2.1
Theory
As
noted in the Introduction, there are anumber
of theoretical paperswhich
show
buyer
sizeconfers countervailing
power
even
with amonopoly
supplier(Maskin and
Riley 1984;Horn and
Wolinsky
1988; Stoleand Zwiebel 1996b; Chipty
and Snyder
1999;and
Chae
and
Heidhues
1999a, 1999b).'^
While
all ofthesemodels
are ofinterestforthe general question ofthe sourcesof countervailing
power,
some
arenotrelevant for our empirical exercise.For
instance, inMaskin
and
Riley (1984), buyers differ not somuch
in size as in the intensity of theirdemand;
size isendogenously determined
by
the size of thebundle
selected.At
least in the short run, the sizeof our buyers, for
example
drugstores, isexogenous,
determined
by
thenumber
of stores inthe chain
and
thenumber
ofcustomers
ateach
store. Also, it is unreasonable toimagine
thatdrugstores, hospitals, or other distribution channels
would
integratebackward
in themanufacture
of drugs, so
Katz
(1987)and Scheffman and
Spiller (1992) are not relevant in the presentcontext.
The
models
of bargainingunder
symmetric
information ofHorn
and
Wolinsky
(1988),Stole
and Zwiebel
(1996b),Chipty and Snyder
(1999),and
Chae
and
Heidhues
(1999a,1999b)
are potentially relevant, though,
and
we
willreview
them
briefly.For
simplicity,we
willreview
Chipty
and Snyder
(1999) as representative of the literature.'^'^There is an additional literature on the effectofbuyer sizeon supplier price when downstream firms compete
(Horn andWolinsky 1988 and Tyagi 2001) which
we
will not treat indetail here.'^Hom
and Wolinsky (1988), Stole and Zwiebel (1996b), and Chipty and Snyder (1999) all share the insightConsider
amarket
with amonopoly
supplierand
three equal-sizedbuyers
having
inelasticdemand
for q units of ahomogeneous
good. LetV{Q)
be
the total joint surplus of buyersand
supplier generated
by
trade ofQ
units.Normalize
the surplusfrom
no
trade for all parties tobe
zero.Suppose
the supplierengages
in independent, simultaneousNash
bargains witheach
buyer
over the transferprice.Each
buyer
conjectures that other buyers bargain successfully withthe supplier in equilibrium. Referring to Figure 1, the object ofnegotiation
between
the supplierand
a givenbuyer
is the marginal surplusA
—
B; assume
a transfer price is agreedupon which
results in an equal division of this surplus,
A-B
Suppose
two
of the three buyersmerge
or otherwiseform
an alliance allowingthem
tobargain as a single unit.
The
unmerged
(small)buyer
continues to obtain surplus given inexpression (1).
The
merged
(large)buyer
bargainsover
surplusA
—
C,
and
obtains half of thisin equilibrium.
Assuming
an
equal division of surplusbetween
the subsidiaries of themerged
buyer, after algebraic manipulation each
can
be
seen to obtainUA-B^B-^^^
(2)
2
V
2 2 ^Merging
effectively allows the buyers to bargainover
inframarginal surplus5
—
C
as well as the marginal surplusA
—
B.
Whether
largebuyers
obtainlower
prices than smalldepends on
therelative values of expressions (1)
and
(2). Ifthe joint surplus function isconcave
as in PanelA
ofFigure 1, then the inframarginal surplus
B
—
C
exceeds
the marginal surplusA
—
B,
implying
and Wolinsky (1988) to allow for
n
buyers and decompose the change in surplus into several components. Stole and Zwiebel(1996b) assumecontracts arenon-binding, appropriate giventheirfocus on intra-firmbargainsbetween workers and managers.One
virtue ofStole andZwiebel's (1996b) framework is that equilibrium is guaranteed to exist,while itmay
not in theconvex casein Chipty and Snyder (1999), though thenon-existence problemin Chiptyand Snyder has since been resolved by Raskovitch (20(X)). The relationship between these papers and Chae and Heidhues (1999a, 1999b) isdiscussed below.
(2)
exceeds
(1), in turnimplying
a subsidiary ofthemerged
buyer
obtainsmore
surplusand pays
a
lower
price than the small.We
have
thusdemonstrated
the existence of cases—
namely
caseswith concave
surplus functions—
inwhich
largerbuyershave
countervailingpower
even
against amonopoly
supplier.The
theorydoes
not guaranteesuch
an
outcome, however;
in theconvex
case in Panel
B
a subsidiary of themerged
buyer
obtains less surplusand pays
a higher pricethan the small.
Unfortunately, the
symmetric
bargainingmodels have
notbeen extended
tomultiple suppliers,soitisdifficulttodeterminethecomparative-static effectof
an
increasein thenumber
of supplierson
price discounts for large buyers. Stoleand Zwiebel (1996a)
show
that their extensiveform
game
generates thesame
allocation as theShapley
value; soone
way
toproceed
would
be
to
compute
theShapley
value in the multiple supplier/multiplebuyer game,
recognizing thelack of
an
extensive-form foundation for theShapley
value in this extension.As
shown
in theAppendix,
theShapley
value calculationsproduce
ambiguous
results: the surpluspremium
thatsubsidiaries of large buyers obtain relative to small
may
increase or decrease as thenumber
ofsuppliers increases.
This
result leadsus to suspect thatbargainingmodels
may
notproduce
robustcomparative
statics resultsconcerning
the effect ofmore
competitive suppliermarket
structureson
the discounts offered to large buyers.Given
theexistence of countervailingpower
forlargebuyersdepends
cruciallyon
theconcavityofthe surplus function, it is
worth
askingwhat
theshape
ofthe surplus function is in themarket
for
wholesale
pharmaceuticals.The
source of concavitycan
be
eitheron
the cost side,from
diseconomies
of scale, oron
the benefit side, sayfrom
negativedemand
externalitieswhich
reduce the value of the product as
more
units are sold.''' It is unlikely that pharmaceuticalmanufacture
exhibits substantialdiseconomies
of scale. It is possible that antibioticshave
aform
of negativedemand
externality, in that resistancesmay
be
more
likely to develop forwidely
'"^SeeChipty and Snyder(1999) for adiscussion offactors producing concavity/convexity in the cabletelevision industry, and an exampleofatest forconcavity/convexity ofthe surplus function.
prescribedantibiotics,
though
we
suspectthatsuch
effectsmay
notproduce
strongconcavities.As
Chae
and Heidhues
(1999a,1999b) show, however,
bargainingmodels
withmonopoly
supplierscan
stillproduce
buyer-size effects in theabsence
of concavities ifthere are risk averse partiesinvolved in the negotiations. Therefore, there
remain a
priorigrounds
to test the bargainingmodels
in the particular context ofthe pharmaceutical industry.In the
second
category of models, theexistenceof buyer-size discounts isrelated to theprocessof competition
among
suppliers.Snyder
(1996,1998) examines
theabilityofcompeting
suppliersto sustain collusion in the presence ofbuyers of varying sizes.'^
For
expositional purposes, herewe
will consider a simplified treatment ofSnyder
(1998), inwhich
buyers
arriveon
themarket
sequentially in
each
of an infinitenumber
of periodsindexed
by
i.'^A
buyer
arriving in periodt has
demand
for St units of the good,each
unitproviding itwith
value v.Assume
StG
[s,s] isindependently
and
identically distributed according todistribution functionF.
The
homogeneous
product is
produced by
N
suppliers,which
have
constantmarginal
and
average cost c<
v,and
which
set pricespu
simultaneouslyeach
period.The
suppliersmay
sustain collusion inthe
supergame
with threats oflow
future prices aspunishment
for undercutting.The
logic ofRotemberg
and
Saloner (1986) suggests that it is difficult for suppliers to collude duringbooms
since the benefit
from
undercutting is large relative to the loss of future (average) profits.The
benefit of undercutting can
be reduced
by
colludingon
alower
price duringbooms.
The
same
intuition holds here: collusionis difficult
when
facinga largebuyer
and
priceneeds
tobe
reduced,resulting in
buyer
discounts.As
a corollary of Proposition 1 inSnyder
(1998), itcan be
shown
that if the following'^Elzinga andMills (1997) presenta staticmodelofduopolycompetitionin whichgreater substitutabilitybetween
products leads to lower prices. Unlike Snyder (1996, 1998), their model does nothave comparative statics results
on buyer size.
'*Adrawback ofthis model is that suppliers
may make
essentially simultaneous sales tobuyers of various sizeseach period in practice (although Scherer and Ross 1990, p. 307, discuss the case of government procurement
auctions fortetracycline in the mid 1950s, which
may
bebettercharacterized as sequential). Snyder (1996) showsthatthesame effects arise in amodel in which buyers of varioussizes purchase simultaneously each period.
conditions hold:
^
<
r^
(3)where
E{x)
—
J^
xdF{x)
is the expectations operatorand
5e
(0, 1) is the discount factor, thenthere exists 5*
e
(s,s)such
that the collusive price in the extremal equilibrium (the equilibriummaximizing
suppHer
profit), p*{st) equalsv
for St<
s*and
declines with St for St>
s*.That
is,buyers smaller than a cutoff are
charged
themonopoly
price; buyers largerthan the cutoff receivean
increasingly large discount. Condition (4) is clearly violated ifN
=
1; in this(monopoly)
case there is
no
problem
of sustaining collusion.The
supplier chargesv
per unit to all buyersregardlessofsize, sothere are
no
sizediscounts.At
theotherextreme, asA'^grows
withoutbound,
eventually condition (3) is violated
and
the only equilibrium involves marginal cost pricing,and
hence
no
discounts for largebuyers. Insum,
as depicted in Figure 2, the collusionmodels imply
that
buyer
sizedoes
not confer countervailingpower
when
facing amonopoly
or sufficientlycompetitive suppliers but
does
forsome
intermediatenumber
of suppliers.The
testable differencebetween
the bargainingand
collusionmodels
iswhether
large buyersreceive a discount
even
inthepresence of amonopoly
seller.An
additional testableimplication ofthe collusion
models
is that large-buyer discountsshould
increase asone
moves from monopoly
to
more
competitive suppliermarket
structures.2.2
Institutional Details
Much
of our empirical strategy hingeson
the existence of different substitution opportunitiesacross types of buyers
and
drugs,which
essentially provides us with variation in thetiveness of the supply side.
The
difference in these substitution opportunitiesstem mainly
from
two
sources: the closeness ofa drug's therapeutic indications to other drugs'and
theinstitutionalconstraints
on
certain buyers' ability to switchbetween
therapeutically similar drugs. In there-mainder
of this subsection,we
will discuss the nature ofsubstitution opportunities inwholesale
pharmaceuticals relevant to our empirical
work;
further detailcan be
found
inElzinga
and
Mills(1997)
and
Levy
(1999).Consider
an illustrativeexample.
Suppose
CVS,
a large chain of retail pharmacies, isnego-tiating with Eli Lilly over the price they will
pay
topurchase
theirdrug
Prozac at thewholesale
level.
They know
thatsome
customers
willcome
in off the street with prescriptions forProzac
that
need
tobe
filled,and
there is littleCVS
cando
at that point to alter the prescription.(The
decision has already
been
made
by
a physician at another locationwho
is difficult to contactand
over
whom CVS
hasno
control.) Eli Lillyknows
thisand views
itself(roughly) as amonopolist
in that transaction. In contrast, a hospital or
HMO
can
enter into negotiationswith
Eli Lillywith the ability to threaten credibly that they will not
purchase
Prozac.The
difference is thata hospital
can
induce or require its physicians to prescribe Paxil or Zoloft instead,drugs with
similar therapeutic properties to Prozac's, ifEli Lilly
does
not offer it favorable contract terms.In other
words,
Eli Lillywould
view
itself ascompeting
against the manufacturers of Paxiland
Zoloft inthis transaction.
Not
onlydo
hospitalsand
HMOs
have
the abilitytomake
such
threats,it is standard to carry through
on
them, resulting inwhat
isknown
as a restrictive formulary, alist of
approved
drugs that affiliated physiciansmay
prescribe.The
ability for purchasers to threatenand
make
such
substitutions varies not just with thetype of purchaser (e.g., drugstore versus hospital or
HMO),
but alsowith the drug.Some
drugs,for instance, are therapeutically
unique
and
must
be
includedon
restrictive formularies.At
theotherextreme, all purchasers
can
fairly easily substituteone
generic for another for an off-patentdrug
with multiple generics.'^ 17It
may
beslightly easier for a hospital tomake
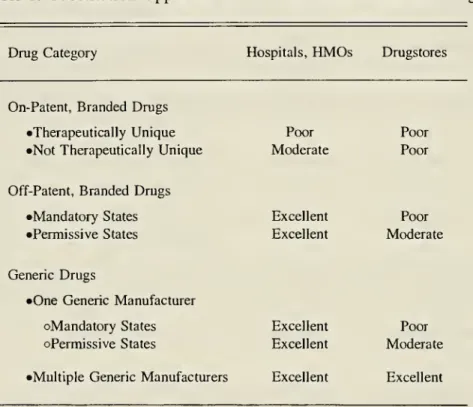
generic-genericsubstitutions over time thanadrugstorebecauseFinally, the case of substituting a generic for a
branded
drug, or vice versa, ismore
compli-cated. Hospitals
and
HMOs
have
excellent substitution opportunities, again using themechanism
of the restrictive formulary.
The
substitution opportunities for drugstores,however,
depend
on
state regulation.
Some
states("mandatory")
mandate
that the drugstoremust
fill the prescriptionwith a generic unless the
customer
specifically requests, or the doctor explicitly notes, that thebranded drug be
dispensed. Inmandatory
states, drugstores' ability to substitutebetween branded
and
generic is constrained.Other
states ("permissive") allow the drugstore tochoose
whether
todispense the
branded
or generic ifneither is explictly requested and/or prescribed. In permissivestates, the drugstore has
some
abilityto substitutebetween branded and
generics.Even
in thesestates, thereis a limit to the ability to substitute
between branded
and
generic: thebranded
pricewill typically
be
higher than the generic since the drugstoremust
carry thebranded
product toserve those
customers
who
bring in a prescription explicitly specifying thebranded
drug.'*Table
1summarizes
the variation in subsitution opportunitesby
type of purchaser, type ofdrug,
and
type of state.Since
our data are collected at the national level,we
willhave
to thinkof drugstore sales as reflecting an average across the different legal
regimes
and
cannot exploitthe variation in that dimension.'^
Note
that during the period our datawere
collected, roughlytwelve states
had
mandatory
substitution laws,and
thirty-eight stateshad
permissive substitutionlaws.
Since our study focuses
on one
therapeutic class, antibiotics, afew
words
shouldbe
saidabout
how
itmight
differfrom
other therapeutic classes. First, the product space is denselypopulated for this class
of
drugs,meaning
that it often is the case that a physician willhave
many
good
alternatives for treating a specific infection. Substitution opportunitiesabound. This
a relatively transient patientpopulationwould not
know
thatthesize,shape,and color ofa tablet wasdifferent thantheonedispensed afew months ago.
'^SeeHellerstein (1998) formore detail on the institutions involving generic substitution.
''Forthe largest chains,itwouldbeappropriatetoaverage acrossstates in anyeventsincetheynegotiate centrally
for thedrugs they retail in stores located throughoutthe country. Forchains or storesoperating in a single state (or
multiple statessharing a
common
legal regime),state-level data would be useful ifitexisted.istrue notjust acrossdifferent drugs butalso
between
branded and
generic versionssince genericpenetration is unusually high in this class.
While
some good
substitution opportunitieswere
importantforour
empiricalexercise,we
were
hoping
to identifysome
therapeuticallyunique drugs
as well, i.e.,drugs
where
even
hospitalsand
HMOs
were
essentially facingmonopoly
supply.An
exhuastive searchconvinced
us that theysimply
did not exist in the case of antibiotics.We
did identify afew
thathad
tobe
includedon most
formularies, forexample
vancomycin,
a last resort antibiotic for methicillin-resistant 5.aureus, but all
were
availablein genericform
orfrom
multiple sources.^*^We
are thereforeunableto exploit variation in substitution opportunities
from
that particular source given the category ofpharmaceutical
we
study.Finally, the issue of
drug
resistancecan complicate formulary
decisions involving antibiotics.One way
to mitigate theproblem
ofbacteriabecoming
resistant to certain antibiotics is to rotatesimilar antibiotics
through
theformulary periodically.The
effect that thispracticemight have on
our analysis is
simply
to decrease the degree towhich
a purchasercan
freely substitute relativetoother therapeutic classes
whose
substitution opportunitiesappear
similar.3
Data
The
data setwe
use toexamine
wholesale
pricing patterns covers virtually all prescriptionan-tibiotics^' sold in the
United
Statesbetween
September
1990
toAugust
1996. Itwas
collectedby
IMS
America,
a pharmaceuticalmarketing
research firm,and
it containsmonthly
wholesalequantities
and
revenuesfrom
transactionsbetween
manufacturers or distributorsand
retailers ofvarious types.
The
data are aggregatedup
to the level of type of buyer.IMS
refers to the type-°We consulted a numberof sources in an attempt to construct a measure oftherapeutic uniqueness. The most
useful was Nettleman and Fredrickson (2001), a handbook intended to teach
new
physicianshow
to prescribeantibiotics. All ofthecompounds that weresuggested to be therapeutically unique turned out tobeoffpatent and
thusto havegeneric substitutes.
^'Ourdata also contain asmall numberofantifungals and antivirals.
ofpurchaser as a "channel ofdistribution,"
and
we
will oftendo
so as well.The
data setcomes
intwo
parts.From
September 1990
toDecember
1991, the data arereported
by two
types ofbuyer: drugstoresand
hospitals, the hospital category covering allnon-federal facilities, i.e., all private
and
nonfederalgovernment
hospitals.From
January 1992
toAugust
1996, the data ismore
refined: drugstores are partitioned into chain drugstores,indepen-dent drugstores,
and
foodstores; the hospital (nonfederal facility) category is retained;and
fournew
categories are introduced—
federal facilities, clinics,HMOs,
and longterm
care—
leading toeight types ofbuyer.^^
We
used
thedata to createtwo
samples.We
createdlongsample spanning
September
1990
toAugust 1996
containing just drugstoresand
hospitalsby
aggregating chaindrugstores,
independent
drugstores,and
foodstores for theJanuary
1992
toAugust 1996
periodto
make
a consistent drugstore series.We
created a shortsample spanning January 1992
toAu-gust
1996
using five of the eightbuyer
types:HMOs,
hospitals, chain drugstores,independent
drugstores,
and
foodstores.We
also included an aggegrate drugstore category (thesum
ofchaindrugstores,
independent
drugstores,and
foodstores)in the shortsample
alongwith
thecomponent
types.
In the
dimension
of product characteristics, the data are quite disaggregated, at the level ofpresentation for
each
pharmaceutical product.A
presentation is a particular choice ofpackaging
and dosage
for a drug, forexample,
150
mg
coated tablets in bottles of 100, or25
ml
of5%
aqueous
solution in a vial for intravenous injection.A
drug
will oftenbe
sold inmany
presentations simultaneously.
Since
the prices reportedby
IMS
in these data willbe
central toour
analysis, it is important^^Federal facilitiesareall typesoffederal government hospitals,nursing homes, andoutpatient facilities. Clinics
include outpatient clinics, urgent care centers, and physician offices. The
HMO
category includes prescriptionsdispensed at
HMO-owned
hospitals and drugstores,not prescriptions dispensed elsewhere but paid forbyanHMO
drugbenefit. The
HMO
channel ofdistribution, then, reflects only a small portion oftheinfluence thatHMOs
and othermanaged care have had on pharmaceutical purchasing. Chain drugstores are in chains offour or more stores.Independent drugstores are owned independently or are in chains not qualifying for thechain drugstore category.
Foodstores aredrugstores located in a foodstore. Longterm care includes nursing homes and convalescent centers
and retail drugstores with more than halfoftheirsales to nursing homes.
Home
health care is not included in thiscategory.
to explain exactly
what
they contain.These
prices are transactions prices, not list prices.They
reflectthe deals negotiated
between
the retailerpurchasing
thedrug
and
thedrug's manufacturer,even
ifthe transaction occurs through a wholesaler. Ifa purchaser negotiates a discount with themanufacturer
and
then purchasesthrough
a wholesaler, they are given a"chargeback"
to reflecttheirdiscount.
Our
data account for chargebacks.Second,
further discounts aresometimes
giventopurchasersin the
fonn
ofrebates.Rebates
are secret, so our datado
not contain them.Such
anomission might have
the potential to seriously biasourresults,but discussion with dataspecialistsat
IMS
and
amarketing
executive at a pharmaceutical firmhave
given us confidence thatwe
understand the nature
and
direction of the bias.It is our understanding
from
these discussions that rebates are not given systematically, saybased
on
aformula depending on volume,
but rather are negotiatedon
acompany-by-company
basis.
During
the period of timecovered
by
our
data, rebates to drugstoreswere
rare.When
rebates
were
given to drugstores, theywere
given for purchasesmediated
by
apharmacy
benefitmanager.
In otherwords,
the priceswe
have
for drugstorepurchases should
be
a fairly accuratereflection of the prices paid
by
drugstores for the portion of theirpurchases
notmediated
by
apharmacy
benefitmanager.
A
biasmay
stillremain
in the drugstorerevenue
variable: omittingrebates results in an overestimate of revenue, akin to considering all drugstore sales to
be
non-mediated
sales,when
only a portion of the saleswould
be non-mediated,
the restmediated
and
possibly reflecting a discount.
Since
we
only use revenues asweights
in theweighted
leastsquares procedure,
and
our results, aswe
discuss below, are quite robust to differentweighting
schemes,
including not weighting at all,we
do
not think secret rebates substantially affectsour
results for drugstores.
Secret rebates,
however,
aremore
pervasive in hospitaland
HMO
sales.Our
prices for hospitalsand
HMOs
would
thusbe
overstatements of the true prices paidby
hospitalsand
HMOs.
This
issue will lead to a bias in our results, understating the discounts that hospitalsand
HMOs
can
extractrelative todrugstores.We
will discussthisbias again in theresultssection, butnote that despite it,
we
find very large discounts for hospitalsand
HMOs
relative to drugstores.For
our
regression analysis,we
have
defined anumber
of variablesand have
included shortdescriptions of
them
inTable
2.A
few
ofthem
need
additional explanation.BRANDED
isa
dummy
variable equalingone
formanufacturer
m
sellingdrug
i ifmanufacturer
m
is the originator ofdrug
i.ONPAT
is aduinmy
variable equalingone
ifno
genericshave
entereddrug
iat
time
t.To
be
precise, a patentcould
have
expired withno
generic entry, but forour purposes,it is generic entry, not patent expiration per se, thatis relevant.
Table
3 presents descriptive statistics for the variableswe
use in the analysis.The
tablecontains
two
sets ofdescriptive statistics,one
for the longsample
with the aggregatebuyer
typesand
one
for the shortsample
with the finerbreakdown
ofbuyer
types.Note
thatNUMGEN
and
ONEGEN
areonly defined for off-patent observations—
hence
thesmallernumber
of observations for thosetwo
variables—
and
theaccompanying
descriptive statistics are thus conditionalon
the observation being off-patent.Considering
the descriptive statistics forprices, itis interesting tonotethatcomparing
averageprices across channels,
both
in the longsample
and
the short sample,does
not reveal largedifferences. Controlling for the
mix
of productspurchased
througheach
of these channels willturn out to
be
important. In particular, hospitals tend tobe
both restrictive purchasers as well aspurchasers of
more
expensive
presentations.The
regression analysis will look at pricedifferencesacross
common
presentations to control for the different mix.Another
interesting feature of thedataisthe relativelysmall fractionof observations
(11%)
fordrugs stillon
patentand
the relativelylarge
mean
ofnumber
of generic competitors (16.8) across off-patent observations. This featureis in part an artifact of the structure of the data:
once
acompound's
patent expiresand
thereis generic entry,
each manufacturer
of thecompound
accounts for a separate observation.This
feature is also
due
to the higher generic penetration of antibiotics relative tomany
other typesof drugs.
Many
of themost
popular
antibiotics are quite old.Old
antibioticsdo
not necessarilybecome
obsolete asnew
ones
enter the market; the available variety, in fact, is an important toolfor
combating drug
resistance.4
Methods and
Results
In order to study empirically the factors that give rise to countervailing
power
and
distinguishamong
various theories,we
willwant
to seehow
priceschange
across different supplyregimes
and
with differentbuyer
sizes. In other words,we
will regress prices (insome
form)
on
a seriesof
dummy
variableswhich
identifythe fourmain
circumstancesunder
which
adrug
is purchased:the
drug
isbranded and
stillon-patent, thedrug
isbranded
but has generic competitors, thedrug
isgeneric but there is only
one
genericmanufacturer
(single-source generic),and
thedrug
is genericand
there are multiple generic manufacturers.We
includedummy
variablesand
interactions todescribe
each
of those four circumstancesand
thenomit
the constant, for ease of interpretation.One
would
alsowant
to include drug, presentation, manufacturer,and
time fixed effects;we
estimate a differenced
model which
accounts for those fixed effects as well as allcombinations
ofthem.
An
additional virtue ofthe differenced specification is that the coefficients are readilyinterpretable. In
sum,
we
estimate a base regression inwhich
thedependent
variable is thedifference in price paid by, for instance, drugstores
and
hospitalsand
the regressors aredummy
variables forcategories of
drug
as described above.To
be
precise, thedependent
variable for thehospital-drugstore regression is
A^Pm^t
=
In {PRICE,,j,m,t,H)-
In{PRICEij^m,t,D).In addition to
examining
the differencebetween
prices paidby
hospitalsand
drugstores,we
lookalso at the difference
between
chainand independent
drugstores,HMOs
and
drugstores,and
HMOs
and
hospitals.We
denote thosedependent
variables as A*^^, A'^^,A^^,
respectively.The
regressionscomparing
price differencesbetween
chainand independent
drugstores give usa fairly clean
comparison
ofthe relativeimportance
ofsizeand
restrictiveness aswe
look acrosscoefficients.
The
regressionscomparing
drugstores to hospitalsand
HMOs
areless cleanbecause
we
do
nothave
informationon
relative size, but these results will still provide informationon
the
importance
of restrictiveness.We
can, of course, control for other covariates in a regressionframework, such
as atime
trend,
which
we
do
insome
specifications. Finally, note that the observations are at the levelof presentation-drug-manufacturer,
and
we
discusshow
toaccount
for the detail of our data incomputing
standard errors below.Table
4
presents resultsfrom
our base regressions.The
firstcolumn
seeks to explain thedifference in prices
paid
by
chain drugstoresand independent
drugstores.Chain
drugstoresand
independent
drugstores should notdiffer intheir restrictiveness—
neithercan be
restrictive against on-patentbrand-name
drugsand
theycan
be
onlyslightly restrictiveagainst off-patentbrand-name
drugs or single source generics, but both
can
be
restrictive against multiple source generics.The
onlydifference is that chain drugstores will tendto
be
large-volume buyerswhereas independent
drugstores will not. Recall that the
dependent
variable is the log ofthe differencebetween
pricespaid
by
chainand independent
drugstores.The
interpretation, therefore, of the 0.002 coefficientestimate
on
ONPAT
x
BRANDED
is that chain drugstorespay
0.2%
more
forbranded
on-patentdrugs than
independent
drugstores do.The
coefficient is not significantly differentfrom
zero,and
given its small standard error,one
shouldconclude
that the effect is precisely estimated tobe
about zero.This
result takenon
itsown
would
tend to castdoubt
on
the relevance of thebargaining
models
in our market. In the face ofmonopoly
supply, large buyers are not able toextract
any
discount at all. Strikingly, the prices theypay
seem
not toeven
reflecttransactions-cost savings
from high-volume
transactions, a portion ofwhich
would
presumably be
passedthrough to the buyer.
The
nexttwo
coefficients represent supplyregimes
inwhich
drugstoresmight
have
limitedability to substitute,
depending on
the state laws.For
the off-patentbranded
drugs, the chainsreceive a small
(0.3%)
but statistically significant discount.The
discount for the single sourcegenerics is larger (1.7%), but only marginally significant.
These
results providesome
tentativesupport for the
dynamic
models
of countervailingpower
in this setting—
holding other factors fixed, as the supplyregime
becomes
slightlymore
competitive, large buyers are able to extractsmall discounts
from
the sellers relative to small buyers.Finally,
somewhat
surprisingperhaps
is the essentially zero coefficienton
the fourth interTaction, indicating that chains receive
no
discounton
multiple source generics.Our
first instinctwould
be
to believe that thedynamic
models
would
predict larger buyer-size effects in thissit-uation,
one
of greater supply competition. It is the case,however,
that if competition is fierceenough
among
suppliers toapproximate
perfect competition,which
may
be
the case for multiplesource generic drugs, then discounts given to large buyers
would
simply
reflect cost differences.The
first coefficient in thisregression implied that cost differenceswere
negligible,which
would
be
consistent with the zero coefficient here. Overall, the results of this regression indicate thatchain drugstores are not receiving substantial discounts relative to independents, either in the
presence or
absence
of restrictiveness.Small
discounts arebeing
extractedwhen
the supplyregime
is slightlycompetitive.The
second
and
thirdcolumns
ofTable4
present the results for the difference in prices paidby
hospitalsand
drugstores. In these regressions,we
have
little information about the relativesizesofthe competitors, but
we
do
know
thathospitalshave
greater substitution opportunitiesdue
totheir abilitytouserestrictive formularies.
To
reiteratethemain
pointsfrom
Section 2, certainlyfor
any
off-patent drug, hospitals, unlike drugstores,can
choose
to stock either thebranded
orgeneric
and
do
notneed
to stock both.For
on-patent drugs, hospitalsmay
have
less discretion,but they
can
choose
to eliminate adrag
from
their formularies if close substitutes existwhereas
drugstores clearly cannot. In other words, these regressions
comparing
hospitaland
drugstoreprices will provide a test of
how
important restrictiveness is.The
resultsfrom
the shortsample
(starting inJanuary
1992)and
thelongsample
(goingback
toAugust
1990)
do
not differ inany
appreciableway,
sowe
will focuson
thelong sample. All fourcoefficient estimates are highly significant
and
are negative,meaning
hospitals receive significantdiscounts relative to drugstores in all circumstances.
The
smallest discountsoccur
for on-patentdrugs,
about
10%,
consistent with hospitals being able to exercise only limdted restrictiveness inthat case.
For
off-patent drugs,where
hospitalscan always be
restrictive, discounts are steeper,including a
35%
discount for the off-patentbranded
drugs.Branded
manufacturersknow
steepdiscounts are necessary to
keep
theirdrugs
on
formularies in the presence of generics. Notably,formultisource generic drugs, hospitals still receive a sizeable discount,
15%,
despite drugstores'ability also to
be
restrictive in thatone
circumstance.One
possible explanation is that althoughdrugstores
can
be
restrictiveagainstmultisourcegenerics, they arereluctant toswitch manfacturersonce
one
ischosen because
theircustomers might complain
aboutchanges
in the size, shape,and
color of the drug.The
hospital population,being
more
transient,would
notbe
as sensitveto
changes over
time. Itseems
unlikely,however,
that this effectwould
be
importantenough
toaccount
for a15%
discount.The
fourthcolumn
ofTable
4 compares
prices paidby
HMOs
and
drugstores.HMOs
would
be
similar to hospitals in their restrictiveness despite theHMO
channel
containing datafrom
on
siteHMO
pharmacies.Not
surprisingly, then, the resultswe
obtainfrom
this regression are similar to theones
for hospitalsand
drugstores, but the discounts are not asdeep and
thecoefficients are not as significant. Interestingly, the
HMO
discount for multisource generic drugs isonly4%,
compared
with15%
for hospitals relative to drugstores.The
HMO
patient population, especiallyone
purchasingfrom
anon
sitepharmacy,
would
be
more
permanent
thanone
at ahospital, so the smaller discount is consistent with the explanation in the
above
paragraph.Recallthatifanything, theseresults are likelyto understatethe true discount given tohospitals
and
HMOs
relative to drugstoresbecause
hospitalsand
HMOs
may
receive secret price discountsnot reflected in our transactions prices.
Finally, the fifth