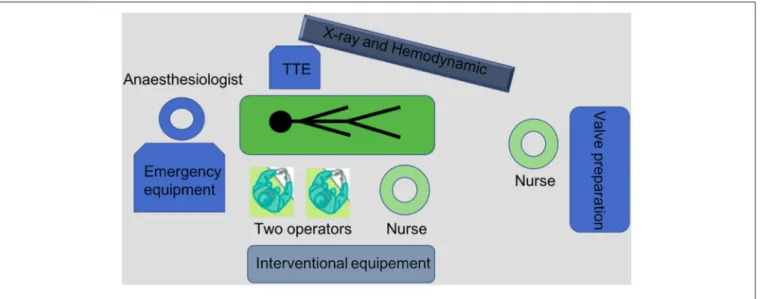
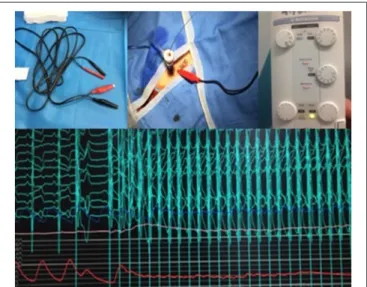
TAVI: Simplification Is the Ultimate Sophistication
Texte intégral
Figure
Documents relatifs
In patients in remission, we tested a vulnerability model in which dif ficulties in interoceptive abilities (DIA) and in awareness of feelings (DAF) could potentially
Since the TEI Dictionaries chapter was initially conceived to account for the kind of infor- mation that appears in machine-readable dictionaries, it only sparsely covers
Il s'agit maintenant de trouver pour chaque paire de phrases, la meilleure traduction de chacun des mots composés identifiés dans la phrase en français, avec la contrainte suivante
Our iterative method is based on the Time Reversal Absorbing Conditions (TRAC) approach [1] and avoids the need for a regulariza- tion strategy.. Numerical results and comparisons
La « révolution maritime », qui fait passer le navire du bois au métal et de la propulsion éolienne à la propulsion par la machine, s’est opérée au XIX e siècle dans les
In this paper we focus on the long-run Total Factor Productivity (TFP) of six Tunisian manufacturing sectors over the period 1983-2002 and investigate the
As for results of multilateral aid’s equation reported in table A7 and A8 (in appendix), we observe that pro-cyclical multilateral ODA affects positively the
We see in the diagram that for a low level of aid, the average success rate is 15 points higher in a stable country. However, in stable countries, this rate decreases sharply with
