Chronic hepatitis C virus infection, a new cardiovascular risk factor?
Texte intégral
Figure
Documents relatifs
DOI: 10.1093/cid/ciaa1014 Atherosclerotic Cardiovascular Events in Patients Infected With Human Immunodeficiency Virus and Hepatitis C Virus Boun Kim Tan,1,2,3,a, Mathieu
The development of an immunocompetent small animal model for the study of HCV infection may be achieved by two approaches: either by transplanting both human liver
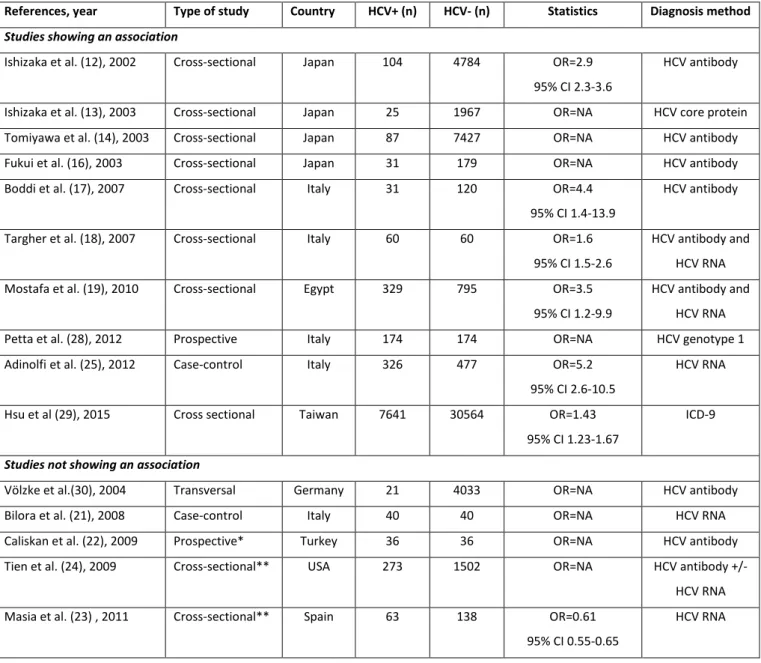
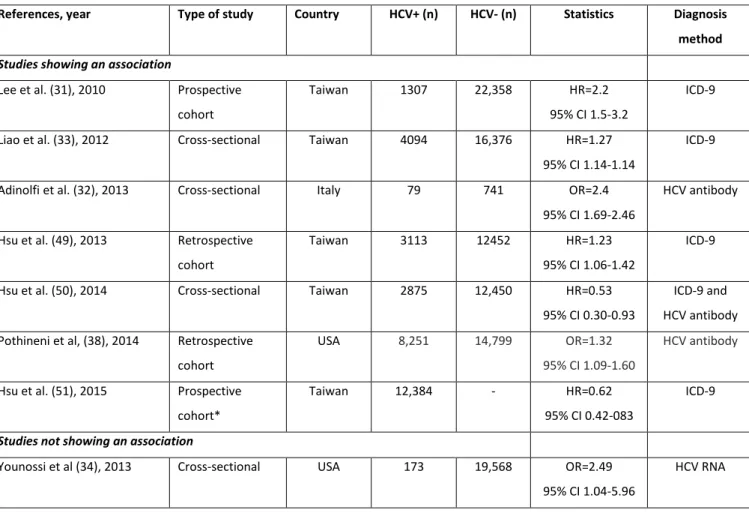
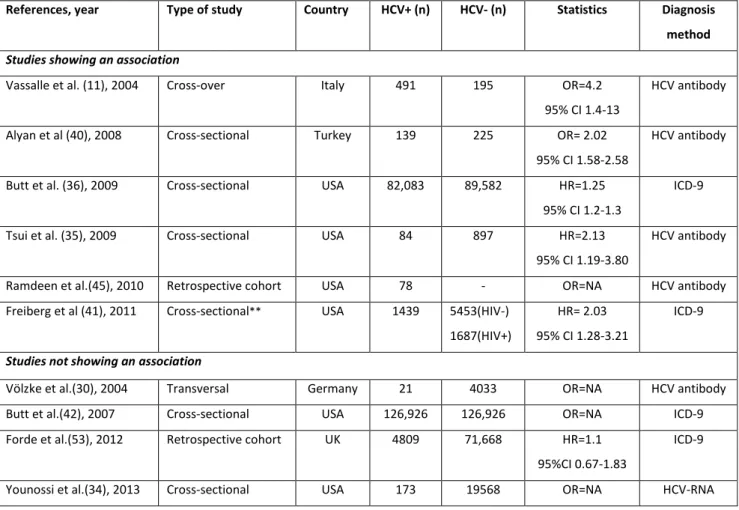
Altogether, many studies provide convincing data that suggest (i) a high prevalence of HCV infection in CKD patients, with a high risk of contamination in kidney facilities, (ii) a
Les malades ont été randomisés en trois bras : bras témoin : IFN pégylé α-2b + ribavirine pendant 48 semaines ; bras TGR : bithérapie de quatre semaines (phase de lead-in), suivie
It is recom- mended to eradicate HCV infection in dialysis patients awaiting renal transplantation and those with acute hepatitis C or significant chronic liver disease..
In this issue of PNAS, Li and colleagues uncover E-cadherin (E-Cad), a major adherens junction protein, as a novel HCV host factor that not only further advances our
Humoral response upon HCV infection was analysed using PLS-DA in correlation with various parameters used by clinicians to assess the severity of the disease: Metavir scores,
We examine whether these associations are independent of morbidities related to lipid levels, such as cardiovascular disease, stroke and hypertension, and inherited
