No posterior mandibular displacement in Angle Class II, division 2 malocclusion as revealed with electromyography and sirognathography
10
0
0
Texte intégral
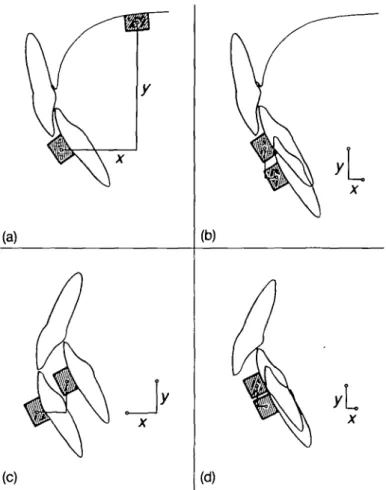
Figure



+2
Documents relatifs