Facial attractiveness of patients with unilateral cleft lip and palate and of controls assessed by laypersons and professionals
Texte intégral
Figure
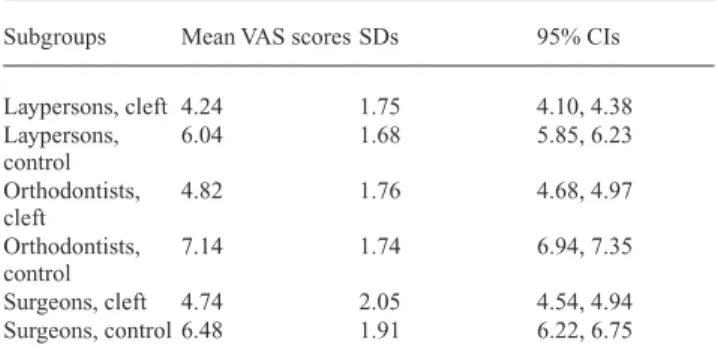
![Figure 1 Mean visual analogue scale scores by occupation, case [patients with clefts (closed diamonds), or control patients (closed circles)] and view (frontal or profile); the bars show the 95% confidence intervals (CIs) for predictive margins.](https://thumb-eu.123doks.com/thumbv2/123doknet/14888442.648048/4.918.172.749.119.541/analogue-occupation-patients-diamonds-patients-confidence-intervals-predictive.webp)
Documents relatifs
This work has led to some interesting insights into the relationship between model checking and other methods of protocol analysis based on strand spaces and Horn clauses. 1
Facial nerve aplasia is an extremely rare condition that is usually syndromic, namely, in Moebius syndrome. The occur- rence of isolated agenesis of facial nerve is even rarer,
In order to evaluate the effects of differ- ent modalities of agent on children, various dependent variables were collected: the numbers of words, phrases and words per
Parallel to the experimental study, we undertook theoretical calculations conformation of the insulated molecule of DNM by using the methods of the DFT (Density
This technique may be also used to measure velocity using signals coming from different types of sensors, for instance where a ground vibration detector has been placed along a
[r]
Graphique 4 • Part des offres sur contrat à durée indéterminée ou sur contrat de plus de 6 mois dans l’ensemble des offres d’emploi collectées par Pôle emploi, par
[r]
