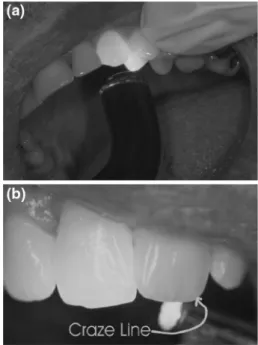
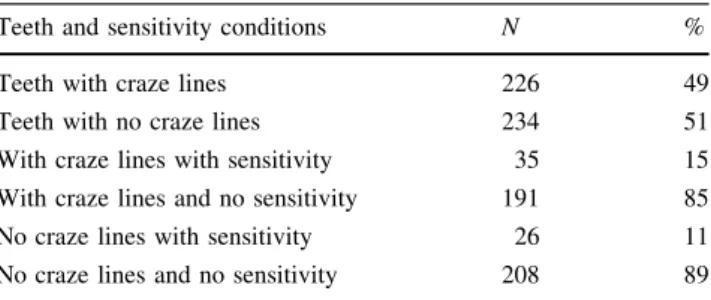
Bleaching induced tooth sensitivity: do the existing enamel craze lines increase sensitivity? A clinical study
Texte intégral
Figure
Documents relatifs
Such solutions were constructed in the context of the nonlinear Schrödinger equations, the generalized Korteweg-de Vries equations, the Hartree equation, the energy critical
s≥0 est dense dans l’ensemble non errant E du flot horocyclique si et seulement si v − n’est pas le premier point (dans le sens trigonom´etrique) d’un intervalle de S 1 \ Λ
Traço pouco comum num livro de filosofía, porém revelador do método de trabalho de Newton da Costa, a maioria destes comentários ou apêndices são redigidos
plants that another Rankine or alternative thermal cycle could operate using the waste heat from the condensor of the conventional power plant as a high
Unwed mothers who decide to place their child for adoption were compared, both pre- and post-parturition, with those who chose to keep their child.. Dependent variables included
Figure 3: Time development of the relative LSW contribution to the water samples and of the LSW source water properties potential temperature Θ (°C), salinity S, oxygen O
The MCMA-2003 field campaign included mul- tiple measurements of ambient VOC compounds from sev- eral instruments: the two DOAS instruments located at the CENICA supersite, two
Paul ne disait rien, il ne savait pas s’il était content ou triste, il ne connaissait pas ces personnes qui le recherchaient, cela lui faisait peur, il s’était habitué ici, il
