Analysis of the Forces on the Spine During a Fall with Application towards
Predicting Vertebral Fracture Risk
by
Sara E. Wilson
S.M. Mechanical Engineering, Massachusetts Institute of Technology (1994) B.S. Biomedical Engineering, Rensselaer Polytechnic Institute (1992) Submitted to the Harvard-MIT Division of Health Sciences and Technology
in partial fulfillment of the requirements for the degree of Doctor of Philosophy in Medical Engineering
At the
MASSACHUSETTS INSTITUTE OF TECHNOLOGY June 1999
© Massachusetts Institute of Technology 1999. All rights reserved.
Author
...
...
Harvard-MIT Division of Health Sciences and Technology May 21, 1999
Certified
by
.. ... ...
Certifie byElizab
Ri.
Myers
Assistant Professor .Thesis Supervisor
Accepted
by
...
...
_ _ MASSACHUSETS INMarta L. Gray FTECHNLTGE J.W. Kieckhefer Professor of Electrical E gineering Co-Director, Division of Health Sciences and Technology NOV I0 1999
Analysis of the Forces on the Spine During a Fall with Application towards
Predicting Vertebral Fracture Risk
by
Sara E. Wilson
S.M. Mechanical Engineering, Massachusetts Institute of Technology (1994) B.S. Biomedical Engineering, Rensselaer Polytechnic Institute (1992) Submitted to the Harvard-MIT Division of Health Sciences and Technology
on May 21, 1999 in partial fulfillment of the requirements for the degree of Doctor of Philosophy in Medical Engineering
Abstract
Age-related vertebral fractures are a common public health problem for the elderly with an estimated 27 percent of U.S. women aged 65 years and over thought to have at least one vertebral fracture. It is important, therefore, to characterize the "at risk" patient and to find methods of reducing that risk. Fracture risk has been defined as the ratio of applied loads to the force required to fracture a bone. Although studies have examined the force required to fracture, few studies have tried to assess the applied loads associated with fractures. Epidemiological studies have found that as many as 30 to 50 percent of vertebral fractures are associated with falls. This work examines the forces on the spine during a backward fall.
Models of a passive fall, without tension in the torso musculature, were constructed in order to examine the peak axial forces on the spine as a result of a passive fall. Muscle tension elements were added to examine the effect of pre-compression of the spine by the musculature. Three experimental and observational studies were performed to examine the input parameters of these models. This included an experimental measurement of the stiffness and damping of the spine segments, measurement and modeling of the fall dynamics in a backward fall, and measurement of the geometry of the torso musculature.
The peak axial forces on the spine were found to range from 1100 Newtons to 3500 Newtons depending on a number of factors including the fall impact dynamics (fall velocity and torso angle), the body weight of the individual, the properties of the soft tissue of the pelvis and spine, and the amount of muscle tension in the torso musculature. These forces can be compared to a mean compressive failure force around 2000 N in elderly thoracolumbar vertebrae. This puts a portion of the elderly population at risk for a fracture simply from an upright passive fall of average velocity. The highest forces were found in upright, fast falls in which the individual had a high upper body weight and very tense torso musculature and little damping in the spine. Thesis Supervisor: Elizabeth R. Myers
Acknowledgements
This work was possible through the generous support of the Whitaker Foundation and the American Association of University Women. Fellowships from these two organizations have been critical in the completion of this work and their support is greatly appreciated.
This work would not have been possible without the support, love and encouragement of many people. There were many stumbling blocks that I might not have overcome without the support of these friends. In particular I would like to acknowledge several people.
Dr. Thomas McMahon came to my rescue when things seemed the bleakest. He provided me with encouragement and a safe and protective research home when I most needed it. He worked behind the scenes many times to assure that I would not be lost or feel forced to give up. He did this, even though I was not his student, showing once again his dedication to the students and his love for the learning process.
C6cile Smeesters, soon to be Dr. Smeesters, has been my officemate, my compatriot and more. She has come to my rescue, even when I sometimes didn't want her to. She has been an understanding and sympathetic ear for any complaints and a true friend.
Dr. Elizabeth Myers has provided almost motherly support and encouragement during my
studies. She has shown, by example, that it is possible to be a compassionate human being and a high caliber researcher.
Tara Arthur, Richard Courtemanche, and Richard Donovan have been good and loyal friends. They have made sure that I don't forget to live life and have fun occasionally.
My parents and grandparents who have been proud of what I am doing, even if they really don't know what it is exactly, and sent me cookies when I was down to show they love me.
Finally, I would like to thank my many friends in the Orthopedic Biomechanics Lab and the Harvard Biomechanics Lab who have cheered my successes, encouraged me when I was down, and made life bearable.
Contents
1 Introduction 15
1.1 Vertebral Fractures 15
1.2 Fall Mechanics 18
1.3 Impact Mechanics and Spine Modeling 19
1.3.1 Pilot Ejection 19
1.3.2 Vibration 20
1.3.3 Pilot Ejection and Vibration Summary 22
1.3.3 Controlled Action Models 22
1.3.4 Stability Models 23
1.4 Summary of Literature 25
1.5 Aims of the Thesis 25
1.6 References 26
2 Impact Mechanics Modeling 33
2.1 Abstract 33
2.2 Introduction 33
2.3 Methods 36
2.3.1 Human Body Models 36
2.3.2 Selection of Input Parameters 37
2.3.3 Validation 40 2.3.4 Sensitivity 41 2.3.5 Force Prediction 41 2.4 Results 41 2.4.1 Validation 41 2.4.2 Sensitivity 42 2.4.3 Force Predictions 46 2.5 Discussion 50 2.6 References 52
Appendix 2.A Equations of Motion for the Four Models 57
3 Muscles and Impact Mechanics 61
3.1 Abstract 61
3.2 Introduction 61
3.3 Methods 63
3.3.1 Models 63
3.3.2 Validation 63
3.3.3 Stiffness Relation Sensitivity 64
3.3.4 Unequal Muscle Tension 64
3.4 Results 64
3.4.1 Validation 64
3.4.3 Unequal Muscle Tension 3.5 Discussion
3.6 References
4 Mechanical Properties of the Spine 4.1 Abstract
4.2 Introduction 4.3 Methods
4.3.1 Specimens
4.3.2 Magnetic Resonance Imaging 4.3.3 Mechanical Testing 4.4 Results 4.5 Discussion 4.6 References 5 Fall Dynamics 5.1 Abstract 5.2 Introduction 5.3 Methods 5.3.1 Human Experiments 5.3.2 Dummy Experiment 5.3.3 Models 5.4 Results 5.4.1 Human Experiment 5.4.2 Dummy Experiment 5.4.3 Models 5.5 Discussion 5.6 References 6 Cross-sectional Anatomy 6.1 Abstract 6.2 Introduction 6.3 Methods 6.3.1 Subjects 6.3.2 Anthropometric Data 6.3.3 Digitization 6.3.4 Data Analysis 6.4 Results 6.5 Discussion 6.6 References 8 66 74 76 79 79 80 82 82 83 83 86 91 92 95 95 95 96 96 98 98 105 105 105 105 107 110 113 113 114 117 117 118 118 119 119 122 129
7 Conclusion 133
7.1 Summary 133
7.2 Predicted Risk 133
7.3 Contributors to Increasing the Forces on the Spine 134
7.4 Limitations and Weaknesses of the Models 137
7.5 Strength of This Work 138
7.6 Future Directions 138
7.7 Conclusion 139
List of Figures
Chapter Number title page number
Chapter 2
2-1 Four Models to Examine Fall Dynamics 38
2-2 Relative Apparent Mass 43
2-3 Phase Shift 44
2-4 Sacral Transmissibility 45
2-5 L3 Vertebral Transmissibility 47
2-6 Seat to Head Transmissibility 48
2-7 Average Angle (,vg) Between Two Objects 59
Chapter 3
3-1 Muscle Models 65
3-2 Seat to Head Transmissibility with Increasing
Muscle Stiffness 67
3-3 Seat to Head Transmissibility with Increasing Initial
Muscle Tension 68
3-4 Axial Spine Force Over Time 69
3-5 Peak Compressive Spine Force for Several
Constant Stiffnesses 70
3-6 Peak Compressive Spine Force for Several
Stiffness-Tension Relations 71
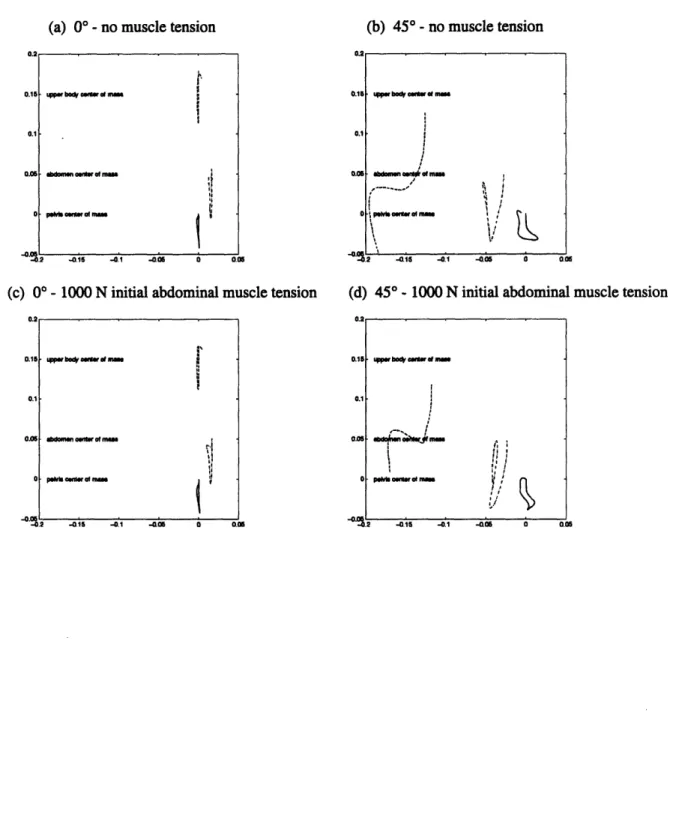
3-7a Motion of the 3 Centers of Mass 72
3-7b Motion of the 3 Centers of Mass 73
3-8 Compressive Force for the 2-dimensional Model at 45° 75
Chapter 4
4-1 The Pendulum Apparatus 85
4-2 Force Transmission After Impact Exhibits
Underdamped Oscillations 87
4-3 Stiffness Increased with Increasing Preload 88
4-4 T2 intensity of the Whole Disk 90
Chapter 5
5-1 Constants for the Joint Angle-Torque Relations 100
5-2 Static Joint Angle-Torque Plots - Ankle 101
5-3 Static Joint Angle-Torque Plots - Knee 102
List of Tables
Chapter Number title page number
Chapter 2
2-1 Input Values 39
2-2 Sensitivity of Peak Compressive Force 49
Chapter 4
4-1 Correlation Coefficients (r) Relating Stiffness Constants
with MRI Based Measurements 89
4-2 Correlation Coefficients (r) Relating Damping Constants
with MRI Based Measurements 89
Chapter 5
5-1 Input Values for a 5% Female 99
5-2 Mean Velocity and Configuration Data for Human,
Dummy and Model Falls 106
5-3 Sensitivity of Vertical Velocity and Torso Angle 108
Chapter 6
6-1 Studies of Cross-sectional Properties 116
6-2 Anthropometric Parameters Measured 120
6-3 Number of Images Available for Each Gender 121
6-4 Mean Moment Arm Lengths in the Thoracic Torso 123
6-5 Mean Moment Arm Lengths in the Lumbar Torso 124
6-6 Regressions of Major Muscle Groups 125
Chapter 7
7-1 Factors of Risk for Fracture 135
Chapter 1 - Introduction and Overview
1.1 Vertebral Fractures
Age-related vertebral fractures are a common problem for the elderly with an estimated 27 percent of U.S. women aged 65 years and over thought to have at least one vertebral fracture
(Melton et al., 1989). These fractures are characterized by a decrease in height of the vertebral body, a wedging of the anterior aspect of the vertebral body and/or a decrease in the height of the center of the vertebral body relative to the heights on the anterior and posterior sides (Smith-Bindman et al., 1991). The incidence of vertebral fractures increases with age from 0.2 per 1,000 per year at ages less than 45 to 1.3 per 1,000 per year in men and 1.2 per 1,000 per year in
women over 85 years (Cooper et al., 1992). The lifetime risk of a clinically diagnosed vertebral fracture is 16% in women and 5% in men (Melton, 1997). These fractures are thought to be due to a decrease in bone density and strength with age, commonly known as osteoporosis.
Osteoporosis is a disease characterized by a bone mineral density (BMD) of the hip, spine or forearm which is more than 2.5 standard deviations below the normal values for young adults
(Kanis, 1994). Approximately 30% of all postmenopausal white women in the United States are within this range for at least one of the three bone regions (hip, spine, or forearm) (Melton,
1997). This lowered bone mineral density in the spine has been shown to significantly increase the risk of a vertebral fracture (Black et al., 1992).
The consequences of a vertebral fracture can include pain, disability, loss of height, loss of independence and increased morbidity and mortality. The five year survival relative to age-match controls for patients with clinically diagnosed vertebral fractures is 0.81 (Cooper et al,
1993). This is comparable with a five-year relative survival of 0.82 for hip fractures. The odds of impairment in an activity such as cooking meals after a vertebral fracture is 6.9 fold that of age-matched controls (Melton, 1997). The direct cost of vertebral fractures in the United States in 1995 was 746 million dollars (Ray et al, 1997).
It is important, therefore, to characterize the "at risk" patient and to find methods of reducing that risk. A bone will break when the loads placed upon the bone exceed the loads required to break the bone. A patient can be said to be at risk when either the loads on the bone are increased or the force required to fracture the bone is decreased. Activities and events such as lifting heavy objects or falling can increase the loads on the spine. The failure load can be decreased due to age- or disease-related changes in the structure or the material properties of the bone.
The force required to fracture a vertebra has been investigated by several researchers. In studies in which the intervertebral disks remained intact to transfer load, vertebrae from younger adults were found to have compressive failure forces of approximately 8000 N. Vertebrae from the elderly were found to have compressive failure forces averaging about 2000-3000 N (Moro et al., 1995, Cody, 1985). Moro et al. (1995) found that vertebrae from cadavers with a mean age of 72 years had an average failure load of 2080 (± 1420) N for the T11 vertebrae and 2620 (± 1510) N for the L2 vertebrae. They found the compressive force needed to fail a vertebra could be as low as 500 N. These studies have also found good correlations between the failure force and densitometric measurements such as bone mineral density using dual energy x-ray
absorptiometry (DXA) or computed tomography (CT). Moro et al. (1995) found that lumbar bone mineral density of the L2 vertebra using DXA in the lateral plane correlated significantly
with L2 compressive failure force with a correlation coefficient of 0.89 and with T11
compressive failure force with a correlation coefficient of 0.94. Brinckmann et al. (1988) found a correlation coefficient of 0.80 between a CT based estimate of bone density and failure force.
While several studies have looked at the decreases in the force required to fracture a vertebra, its correlation with decreases in bone mineral density, and the effect of pharmacologic intervention, few studies have examined the forces applied to the spine and how they might be reduced. Such forces could be high both in controlled heavy loading situations such as lifting or bending and in accidental events such as falls or trauma.
Two studies, using patient reports of the events preceding vertebral fracture, have shown that a high proportion of patients associate a fall with their fracture. Ina population-based study, Cooper et al. (1992) found that 86 of 228 vertebral fracture patients (37%) whose fractures were not diagnosed incidentally and were not a result of severe trauma reported associating the onset of pain with a fall from standing height. Of the other patients, 29 (13%) patients reported lifting a heavy object and 113 (50%) patients reported no significant event associated with the onset of pain. in a survey, Myers et al. (1997) found that 56% of patients seen in the emergency room for a vertebral fracture associated falling with their fracture. In this study, 23% of the patients were involved in controlled activities such as lifting and 18% did not associate a particular activity with their injury. Of these patients 56 % reported a backward fall, 11% reported a sideways fall,
11% reported a forward fall, and 11% could not recall the fall direction (Myers, 1998).
Because falls account for as much as 56% of associated activities, it is essential therefore, to try to assess the forces on the spine during a backward fall in order to understand fully the risk of fracture.
1.2 Fall Mechanics
Several studies have examined aspects of falling and the elderly. Factors such as chronic disease, medications, environmental hazards, changes in balance or gait, and changes in mental cognition have been shown to predispose a person to fall (King et al., 1995, Tinetti et al., 1988, Tinetti et al., 1995). Studies have also shown that interventions such as exercise, behavioral instruction and reduction in sedatives decrease the likelihood of a fall (Tinetti et al., 1994, Privince et al., 1995, Lord et al., 1995).
Other researchers have looked at the initiation of a fall and mechanisms for recovery. Zhang et al. (1992) found that subjects used a combination of swaying and stepping to recover from a lateral fall. They found that foot response times were significantly slowed in the healthy elderly subjects compared with young subjects. Sprague et al. (1993) reported that older adults took larger, slower steps than young adults in response to postural disturbances.
There have been very few studies of what occurs after a fall has been initiated. Most of the work has focused on sideways falls because of the importance of side falls in the etiology of hip fractures. Kroonenberg et al. (1996) studied the descent phase of sideways falls and found average impact velocities of 3.09 ± 0.41 m/s for "relaxed" falls and 3.31 ± 0.43 m's for "active" falls. In another paper, Kroonenberg et al. (1995) modeled sideways falls using 2 and 3 link models of the human body. They found impact velocities in the models ranged from 2.47 to 4.34 m/s depending on the size of the person and torso angle at impact. Robinovitch et al. (1991, 1997) modeled the impact of a side impact fall and found forces on the hip varied between 1145 N to 8600 N depending on speed, torso angle, and stiffness properties of the pelvis soft tissue.
1.3 Impact Mechanics and Spine Modeling
While no researchers have examined the forces on the spine during a fall, researchers have tried to examine forces on the spine or the acceleration of the spine during other events and actions. These include examining pilots ejected from fighter aircraft, occupational exposure to vibration, and lifting and bending, particularly in an occupational setting.
Pilot Ejection
In the early 1970s, several investigators examined the problem of vertebral fractures in young healthy fighter pilots who were ejected from their aircraft during a crash. These fractures were thought to be due to the high vertical acceleration needed for the pilots to clear the cockpit. Models created to examine this event included lumped parameter models ranging from simple one or two degree of freedom models to complex models with many degrees of freedom. One of the earlier models (Terry and Roberts, 1968) considered the body to be a single mass over a viscoelastic element. They concluded that a viscoelastic rod more closely approximates the response of the spine acceleration of the spine due to an inpulse at the base than an elastic rod. Orne and Liu (1971) created a model in which individual vertebrae were represented as masses connected by stiffness and damping elements. They found that bending played a role in the response of the spine to an input acceleration pulse and that the time to peak loading was
approximately 0.04 s. They predicted forces as high as 7000 N in response to a 10g acceleration impulse. Prasad and King (1974) created a similar model, incorporating a second set of springs to represent facet joint action and validated this model with experimental data on the facet joint pressures. Belytschko et al. (1978) created a three-dimensional model in which the vertebrae
were represented as individual elements, the facets were represented by spring elements and the abdomen was represented as a fluid column. Belyschko predicted axial forces of up to 4270 N and moments of between -11.11 and 11.19 Nm in response to a 10g pelvis acceleration
depending on the level of the spine, angle of seat, and speed of onset of the acceleration pulse. These models, in general, suffered from a lack of experimental data on the mechanical properties of the body and from a lack of appropriate validation data. Prasad et al. (1974) were able to validate a complex model of the body including components representing the facet joints with cadaveric intrafacet force data from sled tests. They found that cadaveric intrafacet forces followed a slightly underdamped pattern with a peak at around 50 ms in response to an
acceleration pulse. They also found that facet joints showed a pattern of compression followed by tension. This pattern resembled the predicted forces seen in the model when exposed to the
same acceleration conditions.
Vibration
Models of vibrational dynamics have, in general, used simpler models than those used for pilot ejection to represent the dynamics of the human body and spine. Patil and Palaichamy
(1988) represented a person sitting on a tractor as parallel spring-dashpot pairs connecting masses representing the pelvis, abdomen, diaphragm thorax, back, torso and head. Wan and
Schimmels (1997) represented the human body with similar parallel spring-dashpot pairs separating four masses representing the lower torso, viscera, upper torso and head. This model was validated against data from several experimental studies of vibration dynamics of the torso and used to examine the effect of different seat cushions. Broman et al. (1996) examined the
gain and phase of human body vibration response using a two-dimensional model with two masses that are connected by a freely rotating rod. The first mass was connected to the ground via horizontal and transverse spring-dashpot pairs. A rotational spring-dashpot pair resisted rotation of the rod. This model was validated against an impact experiment in which the phase and gain of the lumbar spine response were measured.
Several experiments were also performed in order to assess vibrational dynamics.
Experimental studies of vibration with human subjects have generally measured acceleration of a marker attached to the body or force exerted by the body seated on a force platform when the body is subjected to a seat vibration of varying frequencies. Griffin et al. (1982) measured acceleration of a bite bar. Panjabi et al. (1986) measured acceleration of K-wires inserted in to the sacrum and L3 vertebral spinous process. Fairley and Griffin (1989) measured force on a seat platform. Kitazaki and Griffin (1998) measured modes of vibration using several
accelerometers attached to the skin over several spinous processes, a bite bar, and the skin of the abdominal wall. Broman et al. (1991) examined motion of markers attached to the lumbar spine as a result of an impact to the seat. In this experiment gain and phase of the resulting
acceleration were examined and used to validate the model by Broman et al. (1996). Gain and phase results from Panjabi et al. (1986), Griffin et al. (1982), and Fairley and Griffin (1989) were used to validate the model by Wan and Schimmels (1997).
The 5 Hz peak frequency often seen in the vibration experiments used for validation can be explained as the resonance frequency of the body mass over the pelvis soft tissue. More difficult to ascertain is the resonance characteristics of the spine and abdominal viscera. The experimental data from Kitazaki et al. (1998) are useful for determining these frequencies.
Kitazaki reported visceral frequencies of 4.9 Hz. They reported that they did not measure above 10 Hz and did no find an axial spine vibration mode. This would indicate that the in situ spine resonance is over 10 Hz.
Pilot Ejection and Vibration Model Summation
Both pilot ejection and vibration models attempt to model a dynamic motion of a seated body in order to get information about what forces or motions the spine is exposed to. While these models were developed for other applications, similar models could be used to examine the forces on the spine during a fall. While some of the earlier models were more complex, the later models, which were more often validated against experimental data, showed that a simpler model with a few key elements could model the system dynamics. They also showed the importance of validation in confirming the models. The variety in the predictions of force as a result of a 10g acceleration impulse in the early, less validated models, also illustrates the need for good validation of the models. Another limitation of most of these models is the lack of attention to the sensitivity of final predictions to the input values chosen and often a lack of good input data.
Controlled Action Models
Controlled actions are slower, more deliberate actions such as lifting and bending, which are often studied in order to analyze safety in the workplace. Many studies have examined these types of actions using experiments and models (Cappozzo, 1985, Lee, 1989, McGill, 1985, Schultz, 1982, McGill, 1986, Schultz, 1987, Hughes, 1991, Wilson, 1994). The models have, in general, been quasi-static models in which the forces and moments of the upper or lower body
are balanced against the forces in a cross-section of the torso. The forces considered in this cross-section include the compressive load on the spine and tensile forces of the muscle groups. The simplest models consider only the erector spinae and rectus abdominous muscles in
sagittally symmetric flexion and extension tasks and erector spinae and oblique muscles in lateral bending and flexion tasks (Cappozzo, 1985, Lee, 1989, Schultz, 1982). More sophisticated models incorporate other muscles including the latissimus dorsi, psoas and quadratus lumborum muscles (McGill, 1986, Schultz, 1987, Hughes, 1991). Because these models are indeterminant,
various techniques are used to determine the configuration of muscle activation. These techniques, include: EMG based configuration, compressive force optimization, compressive force optimization with incremented maximum stress and minimization of the maximum stress followed by compressive force optimization.
These models are less helpful in the modeling of a fall because they are quasi-static. However, they do illustrate the complexity of the torso musculature activity in even simple controlled acitivites and the difficulties involved in estimating muscle tension.
Stability Models
Recent efforts in the low back pain literature have focused on the stability of the spine (Bergmark, 1989, Crisco, 1991, Cholewicki, 1997, Gardner-Morse, 1998, Cholewicki, 1999). Unlike the other models described here, stability models use the dynamic characteristics of the torso musculature. Bergmark (1989) developed the first lumbar stability model with a model of the spine as a single inverted pendulum held in place by several variable stiffness springs
(1977) who reported that stiffness (K) was proportional to active muscle tension (F) with the function:
K=qF
where 1 is the length of the muscle and q is a constant. Morgan (1977) estimated the constant q to be around 40. Crisco (1991) used several sources to estimate the q at between 0.5 and 42 with
a mean value of 10. Cholewicki (1997) used a q of 30. Also difficult to assess is the length of the torso musculature and the contribution of a tendonous attachment. Cholewicki (1997) used a
length of 20 cm for abdominal and extensor musculature, giving an overall q/l of 150 m'. Crisco (1991) commented that although the relationship is noteworthy, it has not been sufficiently researched experimentally for the human lumbar torso musculature.
The main purpose of these models has been to assess the potential for buckling in the lumbar spine and the effect of antagonistic muscle activity. It is believed that antagonistic muscle activity provides stability to the spine. For the purposes of this dissertation, the most interesting aspect of these models is the use of muscle stiffness and tension in dynamic
modeling. The linear relationship between tension and stiffness found in animal studies and used in these stability models can be used to examine the relationship of muscle tension and stiffness to the peak compressive force on the spine.
1.4 Summary of Literature
In summary, vertebral fractures are a significant public health problem. While studies exist examining the forces required to fracture a vertebra, few have tried to assess the force that may be applied to the spine. Epidemiological data have shown that many of these fractures are
associated with backward falls, so it is important to examine what happens to the spine during a backward fall in order to assess risk of a fracture. Previous work that aided in this investigation included previous work done examining fall dynamics and work done examining the loads on the spine during pilot ejection, controlled actions, or as a result of vibration.
1.5 Aims of the Thesis
The aim of this thesis was to answer the research question: What are the forces on the spine during a fall? and Is the magnitude of the compressive force on the vertebra high enough to put the osteoporotic subject at risk of fracture? This question was divided into several topics. First, the impact phase of the fall and the resulting forces on the spine were modeled. Second, the effect of variations in anthropometric parameters, soft tissue stiffness, and spine curvature on the applied forces was investigated. Finally, the dynamics of a backward fall were explored.
This thesis is divided into 5 chapters. These include:
Chapter 1 - Introduction - A literature review and introduction to the
problem
Chapter 2 - Impact Mechanics Modeling - Modeling of the dynamics of the human body
and estimation of the forces on the spine
Chapter 3 - Active Muscle Modeling - Adaptation of the impact models to examine the
effect of active torso musculature on the impact forces
Chapter 4 - Dynamic spine properties - Experimental assessment of dynamic spine
Chapter 5 - Fall modeling
Chapter 6 - Cross-sectional Anatomy
Chapter 7 - Conclusion
and analysis of the effect of disc degeneration on these properties
- Analysis of fall dynamics and evaluation of the impact configuration and velocity
- Measurement of torso musculature geometry for input into models of spinal loading
- Summation of findings and general conclusions
1.6 References
1. Belytschko, T., Schwer, L., Privitzer, E., "Theory and Application of a Three-Dimensional Model of the Human Spine", 49(1), pp. 158-165, 1978.
2. Black, D.M., Cummings, S.R., Genant, H.K., Nevitt, M.C., Palermo, L., and Browner, W., "Axial and appendicular bone density predict fractures in older women", J Bone Miner Res, 7, pp. 633-638, 1992.
3. Broman, H., Pope, M.H., Benda, M., Svensson, M., Ottosson, C., Hansson, T., "The Response of the Seated Subject", J Orthop Res, 9, pp. 150-154, 1991.
4. Broman, H., Pope, M., Hansson, T., "A Mathematical Model of the Impact Response of the Seated Subject", Med Eng Phys, 18(5), pp. 410-419, 1996.
5. Cappozzo, A., Felici, F., Figura,F., and Gazzani, F., "Lumbar Spine Loading During Half-squat Exercises," Med. Sci. Sports Exerc., 17(5), pp. 613-620, 1985.
6. Cody, D.D., Goldstein, S.A., Flynn, M.J., and Brown, E.B., "Correlations between vertebral regional bone density (rBMD) and whole bone fracture load", Spine, 16, pp. 146-154, 1991.
7. Cooper, C. Atkinson, E.J., Jacobsen, S.J., O'Fallon, W.M., and Melton, L.J., "Population-Based Study of Survival after Osteoporotic Fractures", Amer. J. Epidem., 137(9), pp. 10011005, 1993.
8. Cooper, C., Atkinson, E.J., O'Fallon, W.M., Melton, L.J., "Incidence of Clinically Diagnosed Vertebral Fractres: A Population-Based Study in Rochester, Minnesota, 1985-1989", 7(2), pp. 221-227, 1992.
9. Brinkmann, P. Biggemann, M., Hilweg, D., "Prediction of the Compressive Strength of Human Lumbar Vertebrae", Spine, 14:6, p. 606-610, 1989.King, M.B., Tinetti, M.E., "Falls in Community-Dwelling Older Persons", J Amer Geriatrics Soc, 43, pp. 1146-1154, 1995. 10. Fairley, T.E., Griffin, M.J., "The Apparent Mass of the Seated Human Body: Vertical Vibration", 22(2), pp. 81-94, 1989.
11. Greendale GA, Barrett-Connor E, Inlges S, Haile R, "Late Physical and Functional Effects of Osteoporotic Fracture in Women: The Rancho Bernardo Study", J Am Geriatr Soc 43, pp. 955-961, 1995.
12. Griffin, M.J., Whitman, E.M., Parson, K.C., "Vibration and Comfort. I. Translational Seat Vibration", Ergonomics, 25(7), pp. 603-630, 1982.
13. Hughes, R.E., "Empirical Evaluation of Optimization-Based Lumbar Muscle Force Prediction Models," Ch. 4, Ph.D. dissertation, University of Michigan, 1991.
14. Kanis, J.A., Melton, L.J., Christiansen, C., Johnston, C.C., Khaltaev, N., "The Diagnosis of Osteoporosis", J. Bone Min. Res., 9, pp. 1137-1141, 1994.
15. Kitazaki, S., Griffin, M.J., "Resonance Behaviour of the Seated Human Body and Effects of Posture", J Biomechanics, 21, pp. 143-149, 1998.
16. Kroonenberg, A.J.vd, Hayes, W.C., McMahon, T.A., "Hip Impact Velocities and Body Configuration for Voluntary Falls from Standing Height", J. Biomechanics, 29(6), pp. 807-811, 1996.
17. Kroonenberg, A.J.vd, Hayes, W.C., McMahon, T.A., "Dynamic Models for Sideways Falls from Standing Height", J Biomech Eng, 117(3), 309-318, 1995.
18. Lee, K.S., Chaffin, D.B., Waikar, A.M., and Chung, M.K., "Lower Back Muscle Forces in Pushing and Pulling", Ergonomics, 32(12), pp. 1551-1563, 1989.
19. Lord, S.R., Ward,J.A., Williams, P. Strudwick, M., "The Effects of a 12-Month Exercise Trial on Balance, Strength, and Falls in Older Women: A Radomized Controlled Trial", J Amer Geriatrics Soc, 32, pp. 1198-1206, 1995.
20. McGill, S.M., and Norman, R.W., "Partitioning of the L4-L5 Dynamic Moments into Disc, Ligamentous, and Muscular Components During Lifting", Spine, 11(7), pp. 666-678, 1986. 21. McGill, S.M. and Norman, R.W., "Dynamically and Statically Determined Low Back Moments During Lifting," J. Biomech., 18(12), pp. 877-885, 1985.
22. Melton, L.J., Kan, S.H., Frye, M.A., Wahner, H.W., O'Fallon, W.M., and Riggs, B.L., "Epidemiology of Vertebral Fractures in Women", Amer. J. Epidem., 129 (5), pp. 1000-1011, 1989.
23. Melton, L.J., "Epidemiology of Spinal Osteoporsis", Spine, 22(24S), pp. 2-11, 1997. 24. Myers, E.R., private communication, 1998.
25. Moro, M., Hecker, A.T., Bouxsein, M.L., Myers, E.R., "Failure Load of Thoracic Vertebrae Correlates with Lumbar Bone Mineral Density Measured by DXA", Calcif Tissue Int, 56, pp. 206-209, 1995.
26. Myers, E.R, Wilson S.E., "Biomechanics of Osteoporosis and Vertebral Fracture", Spine, 22(24S), pp. 25S-31S, 1997.
27. Orne, D., and Liu, Y.K., " A Mathematical Model of Spinal Response to Impact", J Biomechanics, 4, pp. 49-71, 1971.
28. Panjabi, M.M, Andersson, G.B.J., Jorneus, L., Hult, E., Mattsson, L., "In Vivo
Measurements of Spinal Column Vibrations", J Bone Joint Surg, 68-A(5), pp. 695-702, 1986. 29. Patil, M.K., Palanichamy, M.S., "A Mathematical Model of Tractor-Occupant System with a New Seat Suspension for Minimization of Vibration Response", Appl Math Modeling, 12, pp. 63-71, 1988.
30. Prasad, P., King, A.I., "An Experimentally Validated Dynamic Model of the Spine", J Applied Mechanics, pp. 546-550, September, 1974.
31. Province, M.A., Haley, E.C., Hornbrook, M.C., Lipsitz, L.A., Miller, J.P., Mulrow, C.D., Ory, M.G., Sattin, R.W., Tinetti, M.E, Wolf, S.L., "The Effects of Exercise on Falls in Elderly Patients", JAMA, 273(17), pp. 1341-1347, 1995.
32. Ray, N.F., Chan, J.K., Thamer, M. and Melton, L.J., "Medical Expenditures for the Treatment of Osteoporotic Fractures in the United States in 1995: Report from the National
Osteoporosis Foundation", J. Bone Min. Res., 12(1), pp. 24-35, 1997.
33. Robinovitch, S.N., Hayes, W.C., McMahon, T.A., "Distribution of Contact Forces during Impact to the Hip", Annals Biomed Eng, 25, pp. 499-508, 1997.
34. Robinovitch, S.N., Hayes,W.C., McMahon, T.A., "Prediction of Femoral Impact Forces in Falls on the Hip", J Biomed Eng, 113, pp. 366-374, 1991.
Standing Isometric Heavy Exertions", J. Orthop. Res., 53, pp. 320-329, 1987.
36. Schultz, A., Andersson, G.B.J., Ortengren, R., Bjtrk, R., and Nordin, M., "Analysis and Quantitative Myoelectric Measurements of Loads on the Lumbar Spine when Holding Weights in Standing Postures," Spine, 7(4), pp. 390-397, 1982.
37. Smith-Bindman, R., Cummings, S.R., Steiger, P., Genant, H.K., "A Comparison of Morphometric Definitions of Vertebral Fracture", J Bone Min Res, 6 (1), pp. 25-34, 1991.
38. Soechting, J.F., Paslay, P.R., "A Model for the Human Spine During Impact Including Musculature Influence", J Biomechanics, 6, pp. 195-203, 1973.
39. Sprague, J.K., Ashton-Miller, J.A., Schultz, A.B., "A BIomechanical Analysis of the Use of Stepping to Maintain Balance", 1993 ASME Bioengineering Conference, Vol. 24, pp. 412-414,
1993.
40. Terry, C.T. and Roberts, V.L., "A Viscoelastic Model of the Human Spine Subjected to +gz Accelerations", J Biomechanics, 1, pp. 161-168, 1968.
41. Tinetti, M.E., Baker, D.I., McAvay, G., Claus, E.B., Garrett, P., Gottschalk, M., Koch, M.L., 42. Tinetti, M.E., Doucette, J., Claus, E., Marottoli, R., "Risk Factors for Serious Injury During Falls by Older Persons in the Community", J Amer Geriatrics Soc, 32, pp. 1214-1221, 1995. 43. Tinetti, M.E., Speechley, M., Ginter, S.F., "Risk Factors for Falls Among Elderly Persons Living in the Community", The New England J of Medicine, 319(26), pp. 1701-1707, 1988. 44. Trainor, K., Horwitz, R.I., "A Multifactorial Intervention to Reduce the Risk of Falling Among Elderly People Living in the Community", The New England J of Medicine, 331(13), pp.
821-827, 1994.
45. Wan, Y., Schimmels, J.M., "Optimal Seat Suspension Design Based on Minimum
'Simulated Subjective Response"', J Biomech Eng, 119, pp. 409-416, 1997.
46. Wilson, S.E., "Development of a Model to Predict the Compressive Forces on the Spine Associated with Age-Related Vertebral Fractures", Master's thesis, Mechanical Engineering, Massachusetts Institute of Technology, 1994.
47. Zhang, X., Ashton-Miller,J.A., Schultz, A.B., Alexander, N.B., "A Biomechanical Study of the Effects of Age on Recovery from Impending Lateral Falls", Proceedings of the 16th Annual Meeting of the American Society of Biomechanics, pp. 49-50, 1992.
Chapter 2 - Impact Mechanics Modeling
2.1 Abstract
With an estimated 27 percent of women over 65 years thought to have at least one vertebral fracture, age-related vertebral fractures are a significant public health concern. Recent surveys of patients entering the emergency room have shown that as many as half associated their fracture with a fall. In this work, the impact phase of a backward fall was modeled in order to estimate the maximum forces on the spine during a fall. These forces were found to vary depending on the speed of impact, the angle of the torso and weight of the faller. The highest forces on the spine were for upright falls with high impact speeds. Forces were found to be as high as 2630 N for a woman of average height and weight in an upright fall at an impact speed of
2.53 m/s. Previous studies of the failure force of cadaveric vertebra have shown that this force is enough to elderly vertebra of average or below average bone mineral density. This work shows that falls put many elderly people at risk for vertebral fractures, suggesting that prevention efforts be addressed at preventing falls as well as increasing bone strength.
2.2 Introduction
Age-related vertebral fractures are a growing public health problem. In the United States, an estimated 27 percent of women aged 65 years and over are thought to have at least one
vertebral fracture (Melton et al., 1989). Patients with age-related vertebral fractures can suffer pain, loss of height, and loss of independence. The mortality over five years of patients with vertebral fractures relative to age-matched controls is 19 percent. The direct costs of vertebral
fractures in the United States in 1995 were 746 million dollars (Ray et al, 1997).
Recent studies have shown that falls may play a role in the etiology of vertebral fractures. Cooper et al. (1992) found that 86 of 282 patients with vertebral fractures not resulting from severe trauma reported associating the injury with a fall from standing height. In another study, 56 percent of patients diagnosed with a vertebral fracture and presenting at the emergency room reported associating a fall with the onset of pain (Myers et al., 1996). Among these patients, preliminary data suggests that backward falls are the most common type of fall (Myers, 1998).
While several studies exist looking at the forces required to fracture a vertebra (Moro et al., 1995, Biggemann et al., 1995), no study to our knowledge has examined the forces on the spine during a fall from standing height. The forces transmitted to the spine under such an impact are not well understood.
While the propagation of force during the impact from a fall has not been assessed, the propagation of force from the pelvis to the spine has been studied in the context of examining pilot ejection and vibration dynamics. Modeling efforts in these two areas have included several lumped parameter models of the human body. Experimental efforts have included several
studies with human subjects on the vibrational characteristics of the body.
The earliest models, developed for pilot ejection, included those by Orne, Prasad and Belytschko (Orne and Liu, 1971, Prasad and King, 1974, Belytschko et al., 1978). These were complex lumped parameter models of an upright seated human exposed to an acceleration pulse.
Later models of vibration dynamics of the body, including those by Patil, Broman and Wan, modeled an upright seated human exposed to sinusoidal vibrations using simpler lumped parameter models (Patil and Palanichamy, 1988, Broman et al., 1996, Wan and Schimmels,
1997). These models showed that it was possible to use lumped parameter techniques to model the dynamics of the torso. The variety of different force predictions in the pilot ejection models demonstrated the need for appropriate experimental validation and for good input data. Similar models could be used to examine the forces on the spine during a fall.
Experimental studies of vibration with human subjects have generally measured acceleration of a marker attached to the body or force exerted by the body seated on a force platform when the body is subjected to a seat vibration of varying frequencies. Griffin et al. (1982) measured acceleration of a bite bar. Panjabi et al. (1986) measured acceleration of K-wires inserted in to the sacrum and L3 vertebral spinous process. Fairley and Griffin (1989) measured force on a seat platform. Kitazaki and Griffin measured modes of vibration using several accelerometers attached to the skin over several spinous processes, a bite bar, and the skin of the abdominal wall. These experiments have analyzed the propogation of the force and acceleration through the body and can be used to validate models of the dynamics of the spine and torso such as a model of fall impact mechanics.
There is a need to examine backward falls in order to understand the potential risk for vertebral fracture in elderly individuals. While the dynamics of the torso and spine have been examined in the context of pilot ejection and vibration exposure, no one has examined the dynamics of the torso as a result of impact from a fall. Lumped parameter techniques have been demonstrated to be successful in modeling the dynamics of the torso. However, such models require accurate input data and careful validation.
The present study will use lumped parameter techniques to examine the forces on the spine during the impact phase of a backward fall. The sensitivity of the model to changes in
input parameters and the validity of the models relative to previous experimental studies of whole body vibration will also be assessed. With this model, the maximum compressive force on the spine during a backward fall will be estimated and compared to the fracture force of the vertebrae measured by other researchers.
2.3 Methods
Human Body Models
Four lumped parameter models were created to represent a human body in an impact configuration. The simplest model was a one-dimensional model of a upright fall (Figure 2.1). In this model the thorax, head and arms were represented by one mass, the abdominal viscera by a second mass and the pelvis and upper legs as a third mass. The soft tissues of the pelvis, the spine and the abdominal viscera were represented by a spring and dashpot in parallel (Appendix A).
The second model was a two-dimensional version of the simple model. In this model, the spine and pelvis soft tissue were represented by transverse (anterior-posterior), axial (caudal-inferior) and torsional (flexion-extension) pairs of springs and dashpots. The abdominal viscera was represented by a point mass connected to the pelvis and thorax by transverse and axial stiffnesses. This model allowed consideration of angled impact configurations (Appendix A).
In the third and fourth models, the lumbar spine was represented by five masses connected by parallel spring and dashpot pairs. The third model was a one-dimensional
representation of the upright impact and the fourth model was a two dimensional version. The fourth model allowed for the consideration of spine curvature as well as angulation of the torso.
Selection of Input Parameters
Input parameters including the spring stiffness and damping coefficients of the soft tissues, the masses of the body segments, and the impact velocity and configuration were taken from a variety of sources (Table 2.1). The distribution of mass was based on data collected by Dempster and reanalyzed by Winter (1979). The mass of the arms, head, neck, and thorax were lumped into the upper body mass. The mass of the pelvis and thighs was lumped into the lower mass. The abdominal mass was divided into the viscera and the spine. In the models in which the spine was modeled as one element the mass of the spine was added to the upper body mass. In the segmented spine models, the spine mass was divided amongst the spine segments. For the initial runs of the model data, a female of average height and weight was used. Average total height and weight for elderly women were obtained from a previous study with 120 women over the age of 60 (Greenspan et al., 1996). Inertial properties of the upper body and pelvis in the two dimensional models were determined based on data from the Anthropometric Source Book (1978). The geometry of the two dimensional models was calculated from data by Contini (1972) and by Lui (1971). The lumbar curvature in the two dimensional model with a segmented spine was obtained from Bernhardt (1989).
In Chapter 5, impact velocity and configuration of subjects under self-initiated backward falls are reported. The mean impact velocities and torso angles from this study were used in this model. The vertical impact velocities found in Chapter 5 were 2.18 + 0.34 m/s and the impact torso angles were 47° + 24° .
To estimate the stiffness of the spine segments, instantaneous stiffness of spine segments from creep studies and stiffness from studies of the vibrational properties of the spine were
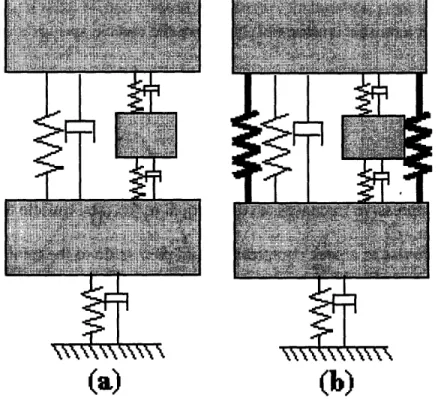
(a) 1-dimensional model
(c) 2-dimensional model
(b) l-dimensional model with a segene d spine
(d) 2-dimensional model with a segment d spine Figure 2.1
Four models of fall dynamics were created to examine fall dynamics. Models were either one-dimensional, (a) and (c), or two-dimensional, (b) and (d), with either a single element spine,
(a) and (b), or a five segment spine (c) and (d). A solid bar represents axial, transverse and rotational elements in the two-dimensional models.
38
I
___r
IT
4
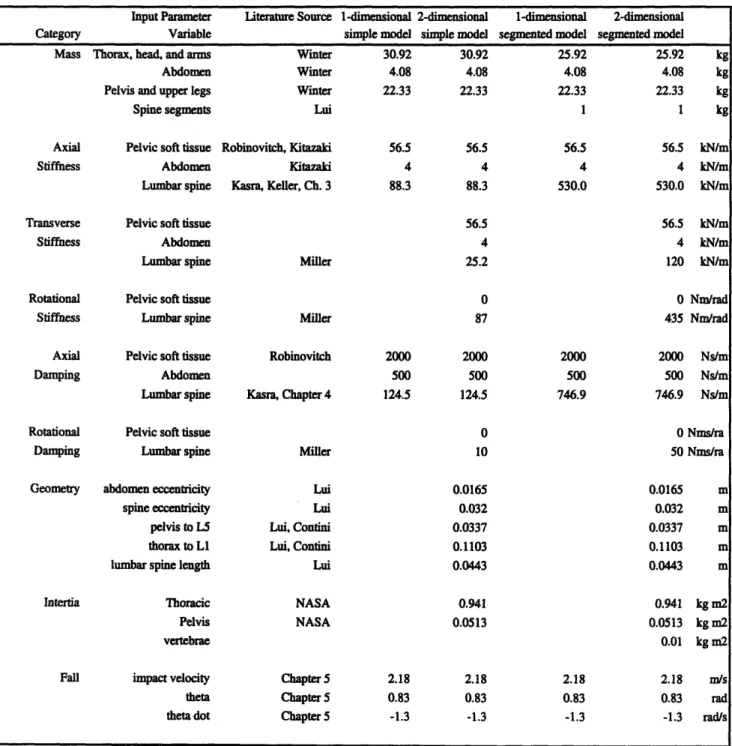
Table 2.1 - Input Values
Input values used in the four models were obtained from a variety of literature sources. These sources included anthropometric data, experimental data from mechanical tests, and whole
body data from experiments with volunteers.
Input Parameter Literature Source 1-dimensional 2-dimensional 1-dimensional 2-dimensional
Category Variable simple model simple model segmented model segmented model
Mass Thorax, head, and arms Winter 30.92 30.92 25.92 25.92 kg
Abdomen Winter 4.08 4.08 4.08 4.08 kg
Pelvis and upper legs Winter 22.33 22.33 22.33 22.33 kg
Spine segments Lui 1 1 kg
Axial Pelvic soft tissue Robinovitch, Kitazaki 56.5 56.5 56.5 56.5 kN/m
Stiffness Abdomen Kitazaki 4 4 4 4 kN/m
Lumbar spine Kasra, Keller, Ch. 3 88.3 88.3 530.0 530.0 kN/m
Transverse Pelvic soft tissue 56.5 56.5 kN/m
Stiffness Abdomen 4 4 kN/m
Lumbar spine Miller 25.2 120 kN/m
Rotational Pelvic soft tissue 0 0 Nnm/rad
Stiffness Lumbar spine Miller 87 435 Nm/rad
Axial Pelvic soft tissue Robinovitch 2000 2000 2000 2000 Nstm
Damping Abdomen 500 500 500 500 Ns/m
Lumbar spine Kasra, Chapter 4 124.5 124.5 746.9 746.9 Ns/m
Rotational Pelvic soft tissue 0 0 Nms/ra
Damping Lumbar spine Miller 10 50 Nms/ra
Geometry abdomen eccentricity Lui 0.0165 0.0165 m
spine eccentricity Lui 0.032 0.032 m
pelvis to L5 Lui, Contini 0.0337 0.0337 m
thorax to L Lui, Contini 0.1103 0.1103 m
lumbar spine length Lui 0.0443 0.0443 m
Intertia Thoracic NASA 0.941 0.941 kg m2
Pelvis NASA 0.0513 0.0513 kg m2
vertebrae 0.01 kg m2
Fall impact velocity Chapter 5 2.18 2.18 2.18 2.18 mn/s
theta Chapter 5 0.83 0.83 0.83 0.83 rad
compared (Keller et al., 1987, Kasra et al., 1991, Miller et al., 1986). Damping of the spine segments was estimated based on damping ratios reported in vibration studies (Kasra et al.,
1991).
The pelvis soft tissue would include muscle, fat, and skin tissue under the bony pelvis. Whole body vibration studies report natural frequencies of around 5 Hz regardless of size or gender (Fairley and Griffin, 1989, Kitazaki and Griffin, 1998). This is generally attributed to the pelvis soft tissue. With the masses for an average woman, this would give a pelvis soft tissue stiffness constant of 56.6 kN/m. Robinovitch et al. (1997) measured the stiffness and damping coefficients of pelvis soft tissue over the greater trochanter to be in the range of 14 to 70 kN/m for the stiffness constant and 13 to 1380 Ns/m for the damping constant. Stiffness of 56.6 kN/m and damping of 2000 Ns/m were chosen.
Validation
To validate the models, we compared model predictions to the results of several
experimental studies of vibration dynamics of the human body from the literature (Figure 2.2-2.6). Fairley and Griffin used a hydraulic vibrator to expose volunteers to random vibrations in a frequency range of 0.25 to 20 Hz. In that experiment, a force platform was placed over the vibrator to measure the force exerted by the volunteer seated on the platform. Panjabi et al. inserted Kirschner wires into the spinous process of two lumbar vertebrae and into the sacrum.
They measured the acceleration of these wires relative to the acceleration of a seat
vibrated at frequencies of 2 to 15 Hz. Griffin et al. measured the vibration of an accelerometer in a bite bar relative to a acceleration of a seat vibrated at frequencies of 1 to 100 Hz.
The models were setup to replicate these experimental conditions. The two-dimensional models were set to a torso angle of 0 degrees. Pelvis rotational stiffness in the two dimensional models was set to 1000 kN/m in order to maintain an upright position. Axial ground vibrations
of varying frequencies were applied to the models. The output of the upper body mass, L3 vertebra and lower body mass motion as well as the force in the axial pelvis soft tissue elements, were compared to the data reported by the three authors.
Sensitivity
The sensitivity of the models to changes or errors in the input parameters was analyzed by varying, individually, each of input parameters by ±5 percent and calculating the change in predicted maximum axial force in the L3-L4 intervertebral disk.
Force Prediction
Once the models were validated and the sensitivity was examined, the predicted forces on the spine were assessed. Several input parameters were varied to examine the effect of altered impact conditions and increased or decreased total weight and height. The forces at different levels of the spine were also compared.
2.4 Results
Validation
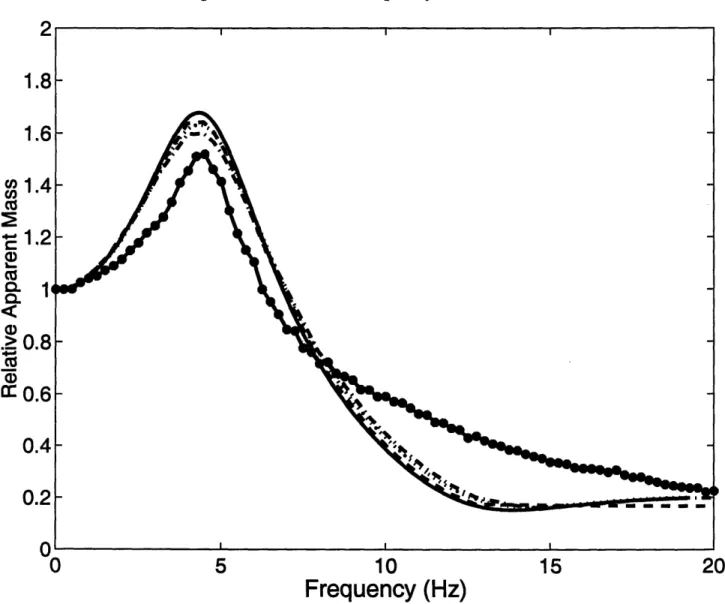
All of the models were found to agree closely with experimental vibrations data (Figures 2.2-2.6). The relative apparent mass response to varying frequencies predicted by the model closely
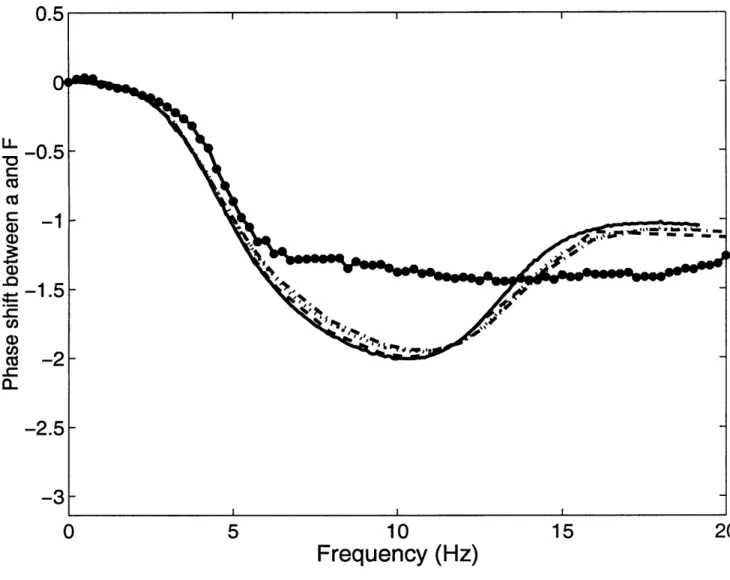
followed that measured by Fairley et al. (1989) with a peak around 5 Hz at approximately 1.5 followed by a decline to approximately 0.2 at high frequencies (Figure 2.2). The phase shift of
the force response to acceleration input was also found to follow the same pattern as that
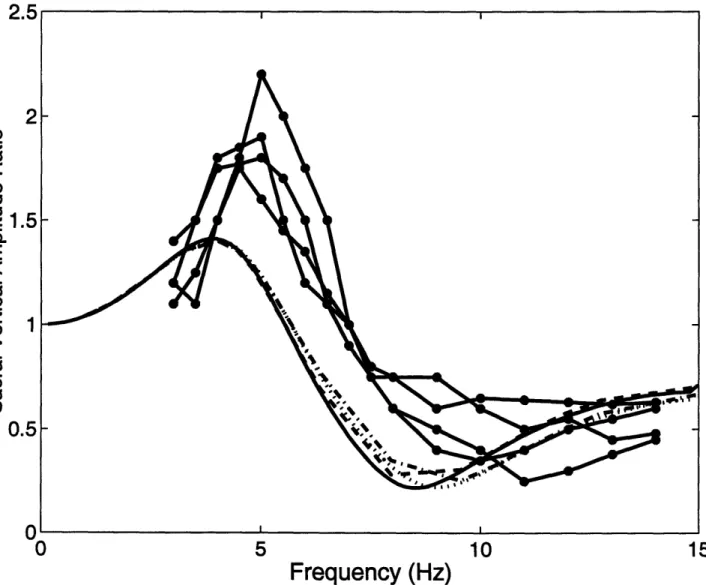
measured by Fairley et al. with a slightly greater phase lag in the mid-frequency (8-12 Hz) range (Figure 2.3). The amplitude ratio of the vibrations at the sacral level was found to peak at approximately 5 Hz with a ratio slightly under that measured by Panjabi et al. (1986) (Figure 2.4). At the L3 vertebral level, the amplitude ratio of the vibrations was found to be within experimental measurements by Panjabi et al., with the segmented models predicting slightly lower amplitudes than the non-segmented models in which the upper body vibration is compared (Figure 2.5). The upper body vibrations in the model compared well with bite bar vibration data from Griffin et al. (1982) (Figure 2.6). The upper body vibrations of the model were found to peak higher than experimental data at frequencies of approximately 5 Hz and attenuate lower than experimental data at frequencies around 10 to 30 Hz.
Sensitivity
The predicted compressive forces from the models were found to be the most sensitive to changes in the impact velocity, impact angle, upper body mass, and axial stiffness of the spine and pelvic soft tissue (Table 2.2). Changes in velocity and angle of impact had the greatest effect on the predicted force with a 10 percent change in the predicted force if either value is varied 10 percent. Changes in upper body mass also had a substantial effect on the predicted force, with a 1 to 2 ratio of change in the predicted force to change in the mass. Other variables with a lower but still noticeable effect on the predicted force included the axial stiffness of the pelvic soft
Figure 2.2 - Relative Apparent Mass
The amplitude of the force on the seat relative to the amplitude of the seat acceleration divided by the resting force (the relative apparent mass) was measured by Fairley and Griffin (1989) and the mean values or each frequency are indicated by *. Vibration of the upper body mass relative to the seat for the four models is indicated by a solid line for the 1-dimensional simple model, a dashed line for the 2-dimensional simple model, a dotted line for the 1-dimensional segmented
model and a dash-dot line for the 2-dimensional segmented model. The four models behave similarly to each other in response to vibration. The models also behaved similarly to the experimental data with a peak frequency of approximately 5 Hz. A lower apparent mass was
predicted in the mid-frequency (10-15 Hz).
uc, C, a) CZ .>
a
0
5
10
15
20
Frequency (Hz)
Figure 2.3 - Phase shift
The phase shift between the force on the seat and the the seat acceleration was measured by Fairley and Griffin (1989) and the mean data for each frequency are indicated by *. Vibration of
the upper body mass relative to the seat for the four models is indicated by a solid line for the 1-dimensional simple model, a dashed line for the 2-1-dimensional simple model, a dotted line for the 1-dimensional segmented model and a dash-dot line for the 2-dimensional segmented model.
The four models behave similarly to each other in response to vibration. The models had a greater phase shift in the mid-frequency (5-15 Hz) region but otherwise followed the
experimental data. U LL -0 cu C a) CD -
a--2
0
5
10
15
20
Frequency (Hz)
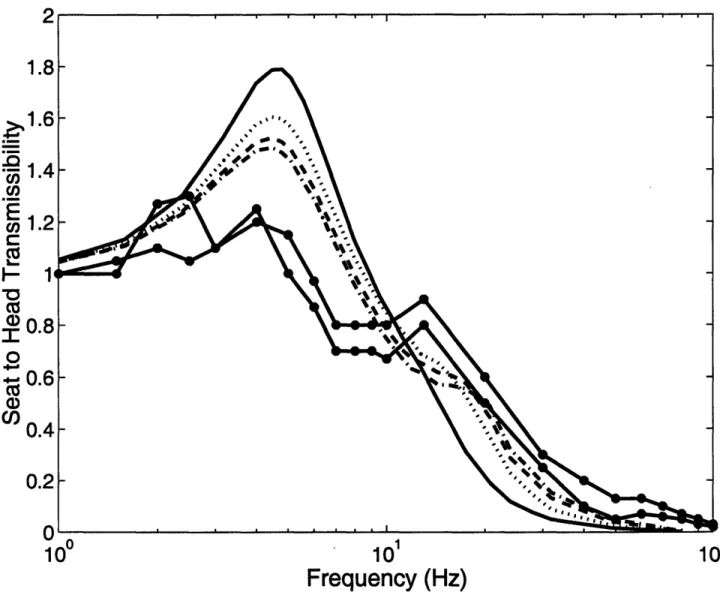
44Figure 2.4 - Sacral Transmissibility
The amplitude of the sacral acceleration relative to the amplitude of the seat acceleration (the transmissibility) was measured by Panjabi et al. (1986) for four subjects and is indicated by *. Vibration of the upper body mass relative to the seat for the four models is indicated by a solid
line for the 1-dimensional simple model, a dashed line for the 2-dimensional simple model, a dotted line for the 1-dimensional segmented model and a dash-dot line for the 2-dimensional segmented model. The four models behaved similarly to each other in response to vibration. The models also behaved similarly to the experimental data with slightly less transmissibility in
the mid-range frequency region and with approximately the same frequency at peak and minimum transmissibility. ^
I-2
2
0
5
10
15Frequency (Hz)
O1.5
'= 1.5
E c70
L. O0.5
0.5
ntissue and the axial stiffness of the lumbar spine. Changes in most of the other variables had very little effect on the final force predictions.
Force predictions
For an average woman (height of 1.59 meters and weight of 65.3 kilograms) impacting upright (0 degrees) at a velocity of 2.18 m/s, the one and two-dimensional single element spine models predicted peak forces of 2505 N and 2461 N. For the segmented spine models, the peak force transmitted from the L3 vertebra to the upper body was 2376 N for the 1-dimensional model and 2165 for the 2-dimensional model. The two-dimensional models predicted lower forces due to rotation of the upper body.
Using the two-dimensional segmented spine model, a 50th percentile woman was found to impact with a maximum axial force on the L3 vertebra of 1404 N for a fall with an impact velocity of 2.18 m/s and an impact angle of -48 degrees. As expected, a larger body size resulted in a larger force with the 95th percentile woman having a maximum impact force of 1567 N for the same fall and a 5th percentile woman having a maximum impact force of 1223 N.
Upright, high impact velocity falls were found to have the highest impact forces. The maximum axial force on the L3 vertebra for a 50th percentile woman varied from 2165 N for an upright fall to 1046 N for a fall with the torso angle at 60 degrees. Increasing impact velocities from 2.18 m/s to 2.5 m/s increased the predicted axial force on the L3 vertebra from 1404 N to
1585 N at an impact angle of 48 degrees.
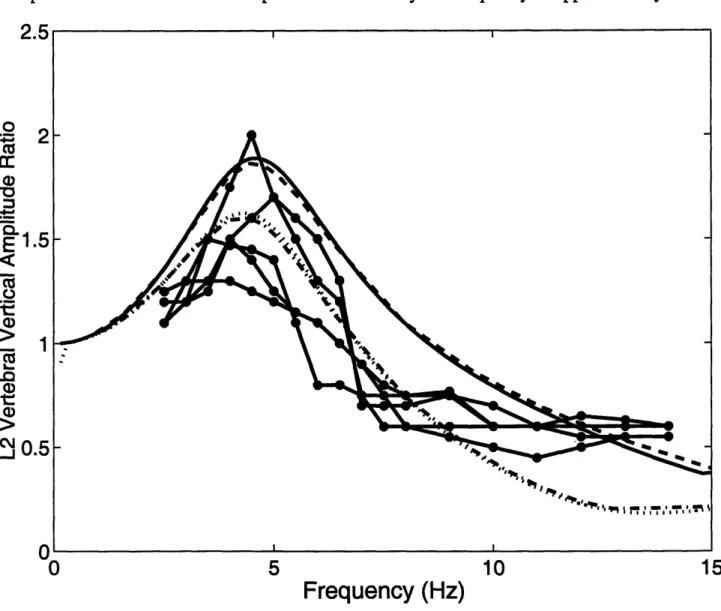
Figure 2.5 - L3 Vertebral Transmissibility
The amplitude of the L3 vertebra acceleration relative to the amplitude of the seat acceleration (the transmissibility) was measured by Panjabi et al. (1986) for five subjects and is indicated by
*. Vibration of the upper body mass relative to the seat for the four models is indicated by a solid line for the 1-dimensional simple model, a dashed line for the 2-dimensional simple model,
a dotted line for the 1-dimensional segmented model and a dash-dot line for the 2-dimensional segmented model. For the single spine segment models, the upper body motion was used instead
of the L3 motion giving a higher peak transmissibility. The models behaved similarly to the experimental data with the same peak transmissibility at a frequency of approximately 5 Hz.
O Cr ci)
.0
E
1 O>
0
5
10
15
Frequency (Hz)
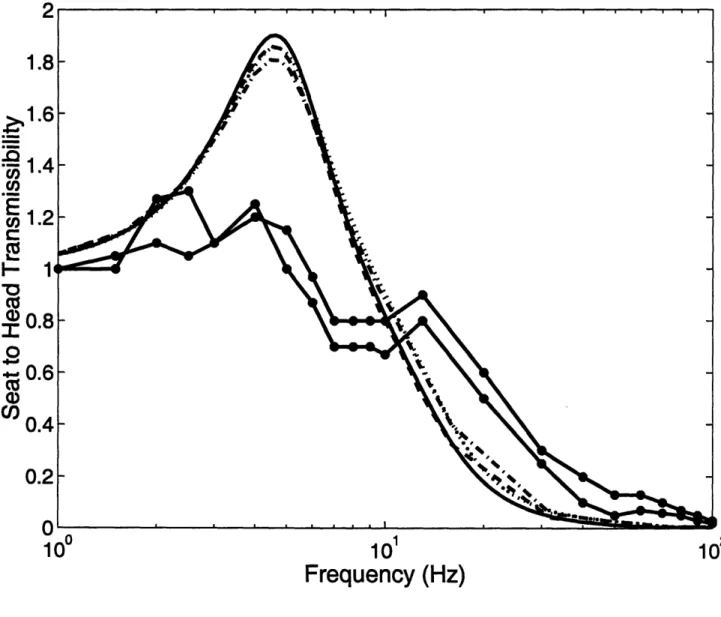
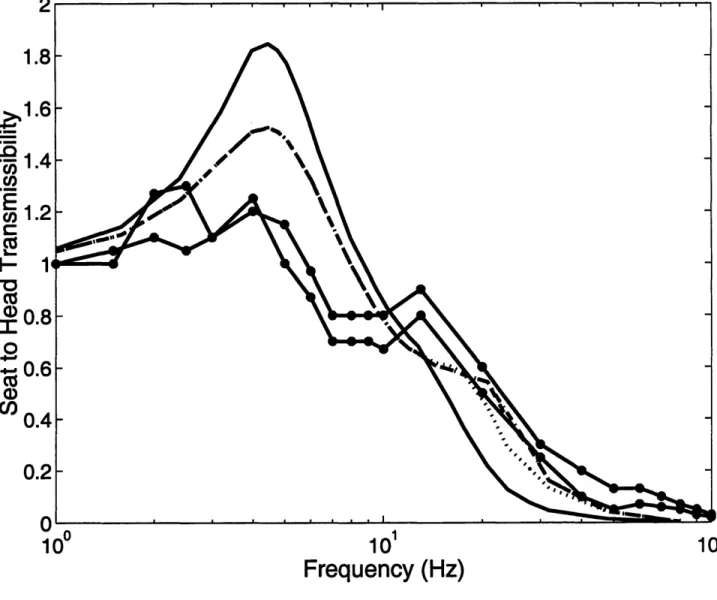
UFigure 2.6 - Seat to Head Transmissibility
The amplitude of the head acceleration relative to the amplitude of the seat acceleration (the transmissibility) was measured by Griffin et al. (1982) and the mean female and male values are
indicated by *. Vibration of the upper body mass relative to the seat for the four models is indicated by a solid line for the 1-dimensional simple model, a dashed line for the 2-dimensional simple model, a dotted line for the 1-dimensional segmented model and a dash-dot line for the
2-dimensional segmented model. The four models behaved similarly to each other in response to vibration. The models also behaved similarly to the experimental data with a slightly higher
peak transmissibility and no secondary peak at 15 Hz.
1.8
1.6
1 .4
coE
u) 1.2 Cm1
i'
I 0.8
"r
o- 0.6
C)C)
0.4
0.2
A 10 0 101 102Frequency (Hz)
48Table 2.2
Sensitivity of the peak compressive force on the spine to changes in input parameters in percent. The input parameters that the peak compressive forces are most sensitive to are highlighted. Changes in the fall dynamics (torso angle and impact velocity) had the greatest effect on the
predicted peak compressive force on the spine.
Input Parameter 1-dimensional 2-dimensional 1-dimensional 2-dimensional
Category Variable simple model simple model segmented model segmented model
Mass Thorax, head, and arms:r: : s 9:
Abdomen 0.1 0.0 0.2 0.1
Pelvis and upper legs -0.5 1.1 -0.2 0.3
Spine segments 0.5 1.9
Axial Pelvic soft tissue 2.2 1.7 2.0 1.8
Stiffness Abdomen -0.1 -0.1 -0.2 0.3
Lumbar spine .. : :i.iri
Transverse Pelvic soft tissue 0.3 0.5
Stiffness Abdomen 0.0 0.1
Lumbar spine 0.0 -1.1
Rotational Pelvic soft tissue 0.0 0.0
Stiffness Lumbar spine 0.0 0.0
Axial Pelvic soft tissue 1.9 1.6 1.6 2.4
Damping Abdomen -0.5 -0.8 -1.0 -2.3
Lumbar spine -1.4 -1.4 -0.6 -0.7
Rotational Pelvic soft tissue -0.1 0.0
Damping Lumbar spine 0.3 0.0
Geometry abdomen eccentricity -0.4 -0.5
spine eccentricity 0.0 0.0
pelvis to LS -0.1 0.1
thorax to L1 -0.1 0.4
lumbar spine length -0.2 0.2
Intertia Thoracic 0.1 0.0
Pelvis 0.0 0.0
vertebrae 0.0
Fall impact velocity
theta
theta dot -0.3 0.11
With the two-dimensional segmented spine model, small differences were seen in the forces in the lower and upper lumbar vertebrae. For an average woman with a velocity of 2.18 m/s and an angle of 48 degrees, the T12/L1 compressive force peaked at 1215 N and the L5/S1
force peaked at 1482 N. The spinal curvature imposed on this model had the effect of making the L4AL5 intervertebral peak compressive force (1669 N) slightly higher than that at the other levels. L1L2, L2/L3, and L3/L4 intervertebral peak forces were 1172, 1293, and 1401 N, respectively.
Pelvis rotational stiffness and damping are a function of the muscular resistance to the pelvis rotating backward. A completely relaxed fall would have a low pelvis rotational stiffness and damping. Increased pelvis stiffness from 0 to 500 N/m increased spine loads less than 10%.
2.5 Discussion
This paper describes efforts to model the human body using lumped parameter
techniques, in order to predict the forces on the spine during the impact phase of a backward fall. Four models were created adding a segemented spine and two-dimensional movement to the simplest one-dimensional model. These models predicted forces of between 880 N and 2630 N depending on the body configuration at impact, the velocity at impact, and the height and weight of the body. This can be compared to experimental studies that have found the fracture forces for thoracolumbar and lumbar vertebrae to vary from as low as 500 N (Moro et al., 1995) to 8000 N (Biggemannn et al., 1995). One study from elderly cadaveric vertebrae had an average axial failure force of approximately 2000 N, below that predicted by these models for an upright fall (Moro et al., 1995).