UOJM |www.uojm.ca April 2021 - Volume 10 - Issue 2
47
RESEARCH
Diagnostic Utility of Creatine Kinase in Patients Presenting
to the Emergency Department with Chest Pain
Keywords: Chest Pain, Creatine Kinase, Non-ST Elevated Myocardial Infarction
Introduction: Creatine Kinase (CK) is routinely performed in some emergency departments (ED) for
Non-ST-elevation myocardial infarction (NSTEMI) workup. Its diagnostic utility is not well understood. The objectives of this study were to assess the value of CK in NSTEMI diagnosis in the troponin era and the association between the highest CK/Troponin values and ejection fraction (EF) during NSTEMI follow-up.
Methods: A prospective cohort study conducted at the two EDs of The Ottawa Hospital from March 2014 to
March 2016 enrolled adults (≥18 years) for whom troponin I (TnI) and CK were ordered for NSTEMI symptoms. We excluded those with ST-Elevation Myocardial Infarction (STEMI). The primary outcome was a NSTEMI within 30 days. We used descriptive statistics and report test diagnostic characteristics with 95% confidence intervals (CI). We compared the highest median CK/Troponin values using Wilcoxon test.
Results: Of the 2,153 patients enrolled, 99 (4.6%) suffered a NSTEMI. The sensitivity and specificity were: CK
(cutoff >250U/L) 31.3% (95%CI 22.2, 40.5) and 91.1% (95%CI 89.9, 92.4) respectively; TnI (cutoff >0.045µg/L) 98.0% (95%CI 95.2, 100) and 86.2% (95%CI 84.7, 87.7) respectively. The median CK values were not significantly different between those with normal (n=267) and abnormal EF (n=55) on follow-up (107 U/L and 118 U/L respectively; p=0.31), whereas the median TnI values were significantly different (0.02 µg/L and 0.1 µg/L respectively; p<0.0001).
Conclusions: CK measurements do not provide any value in the ED work-up of NSTEMI and is not associated
with EF on follow-up. Discontinuing routine CK measurements would improve resource utilization.
Brandon Lam1,2, Hina Chaudry2, Muhammad Mukarram2, Marie-Joe Nemnom2, Soo-Min Kim2, Aline Christelle Ishimwe2, Monica Taljaard2,3, Robert S. Beanlands4, Ronald Booth5,6, Guy Hebert7, Ian Stiell2,3,7, Ven-katesh Thiruganasam-bandamoorthy2,3,7
1Faculty of Medicine,
University of Ottawa, Ottawa Canada
2Ottawa Hospital Research
Institute, Ottawa, Canada
3School of Epidemiology and
Public Health, University of Ottawa, Ottawa, Canada
4Division of Cardiology,
University of Ottawa, Ottawa, Canada
5Division of Biochemistry,
The Ottawa Hospital, Ottawa, Canada
6Department of Pathology &
Lab Medicine, University of Ottawa, Ottawa, Canada
7Department of Emergency
Medicine, University of Ottawa, Ottawa, Canada
ABSTRACT
Introduction: Le dosage de la créatine kinase (CK) est couramment effectué dans certains services d’urgence
pour le bilan de l’infarctus du myocarde sans sus-décalage du segment ST (NSTEMI). Son utilité diagnostique n’est pas bien comprise. Les objectifs de cette étude étaient d’évaluer la valeur de la CK dans le diagnostic de l’infarctus du myocarde sans sus-décalage du segment ST à l’ère de la troponine et l’association entre les valeurs les plus élevées de CK/Troponine et la fraction d’éjection (FE) pendant le suivi de l’infarctus du myocarde sans sus-décalage du segment ST.
Méthodes: Une étude de cohorte prospective menée dans les deux urgences de l’Hôpital d’Ottawa de mars
2014 à mars 2016 a recruté des adultes (≥18 ans) pour lesquels la troponine I (TnI) et la CK ont été prescrites pour des symptômes de NSTEMI. Nous avons exclu les personnes présentant un infarctus du myocarde avec surélévation du segment ST (STEMI). Le résultat primaire était un NSTEMI dans les 30 jours. Nous avons utilisé des statistiques descriptives et rapporté les caractéristiques diagnostiques des tests avec des intervalles de confiance (IC) à 95%. Nous avons comparé les valeurs médianes les plus élevées de CK/Troponine en utilisant le test de Wilcoxon.
Résultats: Sur les 2153 patients recrutés, 99 (4,6 %) ont souffert d’un NSTEMI. La sensibilité et la spécificité
étaient : CK (seuil >250U/L) 31,3% (95%CI 22,2, 40,5) et 91,1% (95%CI 89,9, 92,4) respectivement ; TnI (seuil >0,045µg/L) 98,0% (95%CI 95,2, 100) et 86,2% (95%CI 84,7, 87,7) respectivement. Les valeurs médianes de CK n’étaient pas significativement différentes entre ceux qui avaient une FE normale (n=267) et anormale (n=55) lors du suivi (107 U/L et 118 U/L respectivement ; p=0,31), alors que les valeurs médianes de TnI étaient significativement différentes (0,02 µg/L et 0,1 µg/L respectivement ; p<0,0001).
Conclusions: La mesure de la CK n’est d’aucune utilité dans l’évaluation de la NSTEMI aux urgences et n’est
pas associée à la FE lors du suivi. L’abandon de la mesure systématique de la CK améliorerait l’utilisation des ressources.
UOJM | www.uojm.ca April 2021 - Volume 10 - Issue 2
48
RESEARCH
INTRODUCTION
Chest pain is the second most common emergency department (ED) presenting complaint with an estimated 600,000 patients presenting annually across Canada.1 The etiology of chest pain varies from musculoskeletal
to cardiac causes such as acute coronary syndrome (ACS). ACS encompasses unstable angina (UA), Non-ST Elevated Myocardial Infarction (NSTEMI), and ST- Elevated Myocardial Infarction (STEMI).2 STEMI is diagnosed by electrocardiogram (ECG) and UA is diagnosed clinically in absence of elevated cardiac biomarkers. NSTEMI is defined as a rise and/or fall in cardiac troponin (cTn) with at least one value above the 99th percentile upper reference limit with clinical symptoms of ischemia such as chest pain or shortness of breath.2 As STEMI and UA constitute only 30% of patients with ACS, it is patients with a suspected NSTEMI that take up a significant proportion of ED resources.3 Currently, cTn is considered the standard biomarker for NSTEMI diagnosis.4 However, CK (creatine kinase) is also released into the blood stream as myocardial cells become infarcted and is one of the first cardiac biomarkers available in history to assess for NSTEMI.5 Hence, clinicians in several centers have been measuring serial CK levels in addition to cTn to rule-out NSTEMI. Additionally, in our center, patients hospitalized with NSTEMI have serial CK measurements performed and the peak CK levels documented on discharge.
The primary objective of this study was to assess the value of CK in NSTEMI diagnosis among ED patients with MI symptoms in the troponin era. The secondary objective was to evaluate the association between the highest CK or troponin I (TnI) values and ejection fraction (EF) on follow-up after NSTEMI hospitalization.
METHODS
We conducted a prospective cohort study at two EDs of The Ottawa Hospital (Civic and General Campuses) from March 2014 to March 2016 with the primary objective of developing a pathway for optimal use of the conventional troponin assay. The secondary objective of this prospective study is to assess the role of CK in NSTEMI diagnosis. We enrolled adults (age ≥ 18) for whom cTn and CK tests were ordered for NSTEMI symptoms within the past 24 hours. We excluded patients with STEMI. The study was approved by
the Ottawa Health Science Network Research Ethics Board. Emergency physicians obtained consent and enrolled patients into the study. We collected patient demographics, medical history, cTn and CK values, disposition, final ED diagnosis, and EF on follow-up echocardiogram among patients hospitalized with an NSTEMI. The EF was reported as intervals, >65%, 55%-65%, 45%-54%, 30%-44%, and <30%. EF ≥45 was considered normal while EF <45 was classified as abnormal.6 Both ED academic centers use a conventional Siemens Vista TnI assay.
The primary outcome was an NSTEMI within 30 days of the index ED visit. The outcomes were assessed by an adjudication committee comprised of two physicians who were blinded to the study data. A third physician adjudicated the outcome if there were any disagreements.
Data analysis
We described our patient population using mean with standard deviation (SD), or median with interquartile range (IQR) for continuous variables based on the distribution, and frequency with proportion for categorical variables respectively. We used 250U/L, the upper reference range limit for CK and 0.045 µg/L, the 99th percentile for the normal population for TnI as the cut-point thresholds. We report sensitivity and specificity for the two biomarkers for NSTEMI diagnosis. We report 95% confidence intervals (CI) for the point estimates using either the large sample approximation or the exact binomial distribution where appropriate. We compared the median CK and TnI values between patients in the EF categories (normal vs abnormal) using the Wilcoxon test. We used SAS (version 9.4) software for data analysis. As the primary objective was to develop a troponin pathway, the sample size was guided by this primary objective.
RESULTS
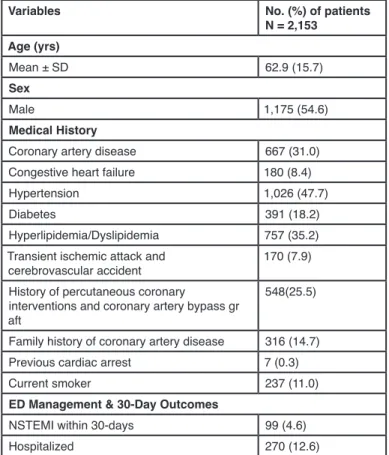
During the study period, of the 2,319 patients enrolled, 25 (1.1%) patients did not have CK measured and we were unable to achieve 30-day follow-up among 141 (6.1%) patients. The remaining 2,153 patients were included in the final analysis. Table 1 shows the baseline characteristics, medical history, ED management and outcomes among study patients. Ninety-nine or 4.6% (95% CI 3.8% to 5.6%) of patients suffered a NSTEMI during the 30-day follow up period. Ninety patients were diagnosed with NSTEMI in the ED and nine patients after ED disposition.
UOJM |www.uojm.ca April 2021 - Volume 10 - Issue 2
49
RESEARCH
Table 1. Patient characteristics and outcomes.
Variables No. (%) of patients N = 2,153 Age (yrs) Mean ± SD 62.9 (15.7) Sex Male 1,175 (54.6) Medical History
Coronary artery disease 667 (31.0) Congestive heart failure 180 (8.4) Hypertension 1,026 (47.7) Diabetes 391 (18.2) Hyperlipidemia/Dyslipidemia 757 (35.2) Transient ischemic attack and
cerebrovascular accident 170 (7.9) History of percutaneous coronary
interventions and coronary artery bypass gr aft
548(25.5)
Family history of coronary artery disease 316 (14.7) Previous cardiac arrest 7 (0.3) Current smoker 237 (11.0)
ED Management & 30-Day Outcomes
NSTEMI within 30-days 99 (4.6) Hospitalized 270 (12.6)
NSTEMI: Non-ST Elevation Myocardial Infarction
There were 213 patients (9.9%) who had CK levels >250U/L and 31 of them were diagnosed with NSTEMI (Appendix 1). Conversely, 68 patients diagnosed with NSTEMI
had a normal CK level. Table 2 shows the diagnostic characteristics of CK and TnI. The sensitivity and specificity of CK for NSTEMI diagnosis was 31.3% (95%CI 22.2% to 40.5%) and 91.1% (95%CI 89.9% to 92.4%) respectively. Of the 99 patients with NSTEMI, TnI was elevated TnI among 97 patients. The sensitivity and specificity of TnI was 97.9% (95%CI 95.2% to 100%) and 86.2% (95%CI 84.7% to 87.7%). The paired agreement for CK and TnI for NSTEMI diagnosis was 0.07 (95% CI 0.03 to 0.12).
Table 2. Diagnostic characteristics of CK and TnI
Diagnostic Characteristics of CK and TnI
Sensitivity (95%
CI) CI)Specificity (95%
CK 31.3% (95% CI
22.2%-40.5%) 91.1% (95% CI 89.9%-92.4%)
TnI 97.9% (95% CI
95.2%-100%) 86.2% (95% CI 84.7%-87.7%)
CK: Creatine Kinase; CI: Confidence Interval; TnI: Troponin I
324 patients had an echocardiography performed within a mean of 22(±25.6) days after hospitalization. Table 3 shows the relationship between EF and highest median CK/TnI values. Patients with normal EF had a median CK value of 107 U/L (IQR 71 to 166) and those with abnormal EF had a median value of 118 U/L (IQR 72 to 195; p=0.31). For TnI, patients with normal EF had a median TnI value of 0.02 µg/L (IQR 0.02 to 0.13) and those with abnormal EF had a median value of 0.1 µg/L (IQR 0.03 to 0.65; p<0.0001).
Table 3. EF versus highest median CK/TnI
Post-Admission EF Versus High-est Median CK/ TnI
Highest Median
CK (IQR) (U/L) TnI (IQR) (µg/L)Highest Median
Normal EF (≥45) 107 (71-166) 0.02 (0.02-0.13) Abnormal EF (<45) 118 (72-195) 0.1 (0.03-0.65)
CK: Creatine Kinase; EF: Ejection Fraction; IQR: Interquartile Range; TnI: Troponin I
Limitations
We compared CK to a conventional TnI assay. However, if compared to high-sensitive troponin assays such as Abbott ARCHITECT, Beckman ACCESS assays, the results may be more significant. Our study enrolled a random sample of patients and hence, selection bias is plausible.
DISCUSSION
While most centers have abandoned the routine CK measurements for evaluation of patients with NSTEMI symptoms, there are still a significant number of healthcare facilities that continue the practice of CK measurements in addition to cTn for chest pain.7,8 However, our study shows evidence that CK is not useful in NSTEMI diagnosis when another cardiac enzyme assay such as TnI provides both a high sensitivity and specificity.
While the specificity of CK and TnI were similar, TnI has a markedly higher sensitivity. Due to TnI’s high sensitivity and specificity compared to CK, TnI should be the only measurement used in patients with a suspected NSTEMI. Among 2 patients that were diagnosed with NSTEMI with TnI values below the cut-off, CK was also within normal
limits and hence, had no diagnostic value.
UOJM | www.uojm.ca April 2021 - Volume 10 - Issue 2
50
RESEARCH
difference of the median CK value between normal and abnormal EF. Although EF may seem associated with CK, the CK median values do not go above the cutoff (>250U/L) meaning these values would not be considered to be abnormally elevated. Furthermore, as the TnI values show an association for future low EF, there is no added benefit from CK measurements, and it is a waste of healthcare resources.
CONCLUSION
In conclusion, our study shows that CK adds no diagnostic value in the workup of a NSTEMI among patients with negative TnI and hence should be discontinued. Our study shows no apparent association between highest median CK values and EF on follow-up echocardiogram. In contrast, TnI shows better association with lower EF. Discontinuing CK measurements will decrease costs and improve resource utilization.
REFERENCES
1. Scheuermeyer FX, Wong H, Yu E, Boychuk B, Innes G, Grafstein E, Gin K, Christenson J. Development and validation of a prediction rule for early discharge of emergency department patients with potential ischemic chest pain. CJEM. 2014;16:106-19.
2. Kumar A, Cannon CP. Acute coronary syndromes: diagnosis and management, part I. Mayo Clin Proc. 2009;84(10):917– 938. doi:10.1016/S0025-6196(11)60509-0
3. Basit H, Malik A, Huecker MR. Non ST Segment Elevation (NSTEMI) Myocardial Infarction. StatPearls. 2019.
4. Thygesen K, Alpert J S, White H D. Universal definition of myocardial infarction. Circulation. 2017; 116, 2634-2653. 5. Al-Hadi HA, Fox KA. Cardiac Markers in the Early Diagnosis
and Management of Patients with Acute Coronary Syndrome. Sultan Qaboos Univ Med J. 2009; 9(3):231-246.
6. Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L, et al. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. 2015;28(1):1-39.
7. Zhang L, Sill AM, Young I, Ahmed S, Morales M, Kuehl S. Financial impact of a targeted reduction in cardiac enzyme testing at a community hospital. J Community Hosp Intern Med Perspect. 2016; 6(5).
8. Wiens EJ, Arbour J, Thompson K, Seifer CM. Routine creatine kinase testing does not provide clinical utility in the emergency department for diagnosis of acute coronary syndromes. BMC Emerg Med. 2019; 19:37.