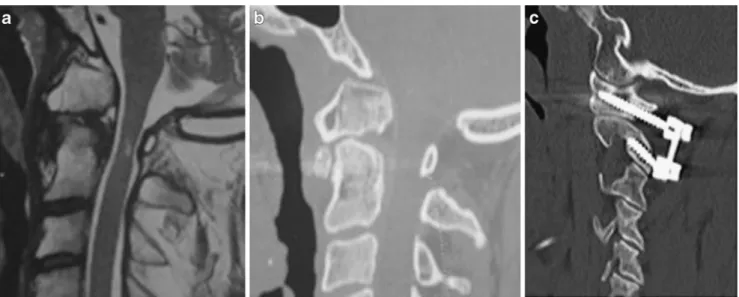
Accuracy of freehand fluoroscopy-guided placement of C1 lateral mass and C2 isthmic screws in atlanto-axial instability
9
0
0
Texte intégral
Figure

Documents relatifs