Personality and Neuropsychological Profiles in Friedreich Ataxia
Texte intégral
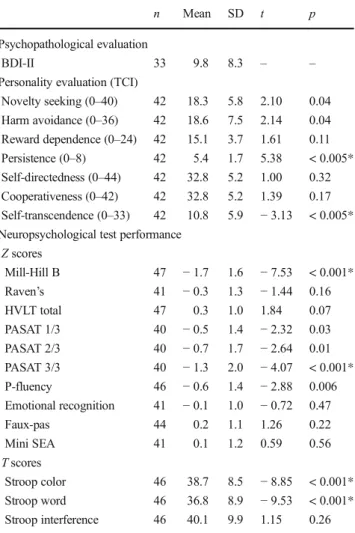
Figure


Documents relatifs
[r]
Findings are often inconsistent and difficult to summarize (for a review, see Riva, Cutica, Pravettoni, 2014); most of the early research findings are based on
In this study we trained artificial embodied neural agents equipped with a pan/tilt camera, pro- vided with different neural and motor capabilities, to solve a well
fulfilled the criteria for atypical autism accord- ing to ICD-10 research criteria: impaired development of language, impaired reciprocal social interaction and
(B) Frataxin mRNA (white) and protein (grey) levels in antisense ribozyme fibroblast clones R2C1, R2C2, R5C1 and R5C2, compared to the Frda L2+/L- non-transfected cell line..
Molecular, clinical and neuropsychological study in 31 patients with Kabuki syndrome and KMT2D mutations.. Natacha Lehman, Anne-Claire Mazery, Antoine Visier, Clarisse
On the other hand 44 percent of data breaches happen in healthcare alone [8,49]. In an evaluation of mHealth solutions and corresponding studies McKay et al. [37] point out the “lack
