Communication skills training for residents:which variables predict learning of skills?
Texte intégral
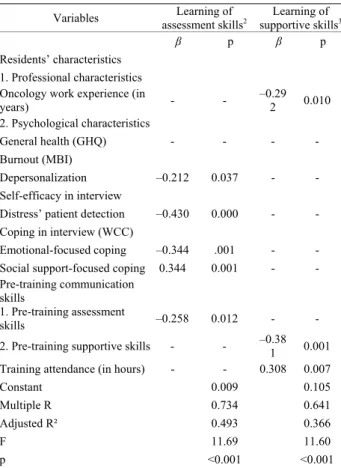
Figure
Documents relatifs
Com- mand line skills training tools can be used to teach operating systems, while in programming subjects, students may be interested in how the similar tools are created..
Thus the game may help to train the skills to choose right approach for specific ac- tor types (pure or combined categories), to recognize actor types, and choose appro- priate
The College of Family Physicians of Canada’s Standards for Accreditation of Residency Training Programs states the following: “Residents must be given
Such strategies as procedural skills clinics and referrals from family physicians to family medicine training sites could also be used to increase the opportunities for resi- dents
Anticipatory judgments of three different tennis skills were practiced across an acquisition phase in either a random or blocked practice order, with learning being measured
Each day of the workshop is divided as follows, so that three key issues are addressed in turn: identification by participants of adolescent needs and problems associated with
L’archive ouverte pluridisciplinaire HAL, est destinée au dépôt et à la diffusion de documents scientifiques de niveau recherche, publiés ou non, émanant des
On a spacetime diagram, this is indicated by the fact that particle motion is restricted to occur only inside the light cone.. The region inside the light cone is
