AJH 1991; 4:348-355
Cardiovascular Pressor Reactivity After Chronic
Converting Enzyme Inhibition
Michaela Bernasconi, Claudio Marone, Carlo Beretta-Piccoli, Giuseppe Lepori, Sidney Shaw, and
Peter Weidmann
I n a d d i t i o n to i n h i b i t i n g t h e f o r m a t i o n of a n g i o t e n s i n II, c h r o n i c c o n v e r t i n g e n z y m e i n h i b i t i o n m a y affect o t h e r b l o o d p r e s s u r e m o d u l a t i n g factors. T h e i n f l u e n c e of a n 8 w e e k t r e a t m e n t p h a s e w i t h Cilaza p r i l o n t h e a c t i v i t y of t h e r e n i n - a n g i o t e n s i n - a l d o s t e r o n e a n d s y m p a t h e t i c n e r v o u s s y s t e m s , t h e p r e s sor r e a c t i v i t y t o i n f u s e d a n g i o t e n s i n II or n o r e p i n e p h r i n e , t h e c h r o n o t r o p i c r e s p o n s e to i s o p r o t e r e n o l , a n d b o d y s o d i u m a n d p l a s m a a t r i a l n a t r i u r e t i c p e p t i d e c o n c e n t r a t i o n s w a s a s s e s s e d i n 11 n o r m a l s u b j e c t s a n d 12 p a t i e n t s w i t h e s s e n t i a l h y p e r t e n s i o n . A s c o m p a r e d t o a 4 w e e k p l a c e b o p h a s e , Cilazapril d e c r e a s e d a r t e r i a l p r e s s u r e i n b o t h s t u d y g r o u p s (from 1 2 4 / 8 3 ± 9 / 6 to 1 1 4 / 7 7 ± 9 / 5 m m H g a n d f r o m 143/102 ± 1 3 / 7 to 1 3 7 / 9 6 ± 1 0 / 1 0 m m H g ; Ρ < .025); e x c h a n g e a b l e s o d i u m (—158 m m o l a n d , r e s p e c t i v e l y , —104 m m o l ) a n d u p r i g h t p l a s m a a l d o s t e r o n e (—24% a n d —15%) a l s o t e n d e d to fall. H e a r t r a t e , t h e c h r o n o t r o p i c r e s p o n s e to p o s t u r e or i s o p r o t e r e n o l , p l a s m a n o r e p i n e p h r i n e l e v e l s , t h e c o n c e n t r a t i o n / p r e s s o r r e s p o n s e c u r v e to n o r e p i n e p h r i n e , p l a s m a a t r i a l n a t r i u r e t i c p e p t i d e c o n c e n t r a t i o n , p l a s m a a n g i o t e n s i n II a n d t h e r e s p o n s e s of b l o o d p r e s s u r e or p l a s m a a l d o s t e r o n e t o a n g i o t e n s i n II w e r e u n c h a n g e d after 8 w e e k s of Cilazapril. P l a s m a r e n i n a c t i v i t y i n c r e a s e d ( + 1 7 5 % t o + 650%). T h e s e f i n d i n g s i n d i c a t e t h a t t h e b l o o d p r e s s u r e l o w e r i n g effect of Cilazapril i n t h e s t a b l e p h a s e of p h a r m a c o l o g i c a l i n t e r v e n t i o n is n o t a s s o c i a t e d w i t h m o d i f i c a t i o n s of s y m p a t h e t i c - d e p e n d e n t p r e s s o r r e a c t i v i t y or ^ - a d r e n e r g i c s e n s i t i v i t y . P l a s m a a n g i o t e n s i n II c o n c e n t r a t i o n a n d a n g i o t e n s i n I I d e p e n -d e n t p a t h w a y s i n c l u -d i n g t h e p r e s s o r a n -d a l d o s t e r o n e r e s p o n s i v e n e s s to a n g i o t e n s i n II a r e also u n c h a n g e d . A m J H y p e r t e n s 1991;4:348-355 KEY W O R D S : C i l a z a p r i l , a n g i o t e n s i n II, a l d o s t e r o n e , n o r e p i n e p h r i n e , e s s e n t i a l h y p e r t e n s i o n .T
h e use of inhibitors of converting e n z y m e h a s b e c o m e a n established principle of a n t i h y p e r tensive p h a r m a c o t h e r a p y , b u t t h e m e c h a n i s m s relating converting e n z y m e inhibition to a d e crease of arterial pressure r e m a i n unclear. Reduction of circulating angiotensin II (All) is t h e initial e v e n t .1U n d e r chronic conditions, t h e relationship b e t w e e n vari ations in arterial pressure a n d circulating All
From the Ospedale Italiano, Viganello; Ospedale S. Giovanni, Bel-linzona; and Medizinische Universitätspoliklinik Bern, Switzerland. This work w a s supported b y a grant in aid by Hoffman-La-Roche, Basle, Switzerland.
Address correspondance and reprint requests to Prof. Dr. m e d . C. Beretta-Piccoli, Ospedale Italiano di Lugano, 6 9 6 2 Viganello, Switzer land.
is less close,2 suggesting t h a t additional m e c h a n i s m s
m a y be involved. Angiotensin II levels in tissues rather t h a n in blood m a y d e t e r m i n e arterial p r e s s u r e .3 Accu
m u l a t i o n of vasodilating k i n i n s4 or p r o s t a g l a n d i n s5 m a y
occur. S y m p a t h e t i c - d e p e n d e n t cardiovascular regula tion m a y b e modified.6 Moreover, t h e p l a s m a levels of a
pressor h o r m o n e are inversely related to t h e cardiovas cular pressor reactivity to t h e m .7 Therefore, a decrease
of circulating All will result in a net depressor effect only in t h e absence of a full c o m p e n s a t i o n by a n i n c r e m e n t e d pressor sensitivity to AIL
After t h e introduction of t h e first oral acting convert ing e n z y m e inhibitor, Captopril, m o r e p o t e n t a n d longer acting substances, such as enalapril, w e r e p r o p o s e d for clinical u s e .8 Cilazapril, o n e of t h e n e w e r substances,
h a s t h e characteristics of a nonsulfhydryl p r o d r u g , ie,
AJH-APRIL 1991-VOL. 4, NO. 4, PART 1 P R E S S O R R E A C T I V I T Y 349
after oral administration it is rapidly converted to t h e active metabolite, cilazaprilat.9 P h a r m a c o d y n a m i c in
vestigations in h u m a n s suggest that this d r u g is m o r e p o t e n t a n d longer acting t h a n b o t h Captopril a n d enala p r i l1 0 a n d does n o t a c c u m u l a t e w i t h r e p e a t e d a d m i n i s
tration despite t h e long half-life.1 1 In order to investigate
further t h e m e c h a n i s m of action of chronic converting e n z y m e inhibition, this long-acting c o m p o u n d w a s chosen; its s i m u l t a n e o u s effects o n several b l o o d p r e s sure m o d u l a t i n g systems including t h e pressor reactiv ity to angiotensin II or n o r e p i n e p h r i n e w e r e e v a l u a t e d in n o r m a l subjects a n d patients w i t h essential h y p e r t e n sion.
SUBJECTS A N D M E T H O D S
T w e n t y - t h r e e subjects aged b e t w e e n 18 a n d 70 years w e r e recruited for t h e study. They included 11 n o r m a l subjects (four w o m e n a n d seven m e n ) , aged 29 to 60 years ( m e a n ± SD age 38 ± 10 years), a n d 12 patients w i t h essential h y p e r t e n s i o n (four w o m e n a n d eight m e n ) , a g e d 26 to 58 years ( m e a n age 45 ± 12 years) w i t h a diastolic blood pressure b e t w e e n 95 a n d 115 m m H g . T h e n o r m a l subjects w e r e h e a l t h y volunteers w i t h o u t p r e v i o u s episodes of h i g h blood pressure a n d w i t h a b l o o d pressure consistently < 1 4 0 / 9 0 m m H g t h r o u g h out t h e study. T h e presence of h y p e r t e n s i o n in t h e p a tients w a s defined b y obtaining r e p e a t e d blood pressure m e a s u r e m e n t s of b e t w e e n 1 4 0 / 9 0 a n d 1 8 0 / 1 1 5 m m Hg, t a k e n u n d e r o u t p a t i e n t conditions. S e c o n d a r y forms of h y p e r t e n s i o n w e r e excluded b y t h e u s u a l tests; n o p a t i e n t h a d m a l i g n a n t h y p e r t e n s i o n ( h y p e r t e n s i v e r e t i n o p a t h y stages I I I - I V ) , e d e m a , a r r h y t h m i a , renal failure (serum creatinine > 9 5 / / m o l / L ) or h e a r t failure. All a n t i h y p e r t e n s i v e d r u g s a n d p o t a s s i u m s u p p l e m e n t s w e r e d i s c o n t i n u e d at least 3 w e e k s before t h e s t u d y b e g a n . N o n e of t h e w o m e n w a s taking h o r m o n a l con traceptives. Informed consent w a s o b t a i n e d from all subjects a n d t h e s t u d y protocol w a s a p p r o v e d b y t h e ethical committee of our institution.
T r e a t m e n t P l a n T h e subjects w e r e instructed to con t i n u e eating a n o r m a l diet, avoiding very h i g h or l o w s o d i u m i n t a k e s .1 2 A placebo (one tablet daily) w a s given
over a period of 4 w e e k s a n d w a s t h e n replaced b y a 2.5 m g dose of Cilazapril, given once daily at breakfast. After 2 w e e k s of treatment, t h e dose w a s increased to 5 m g daily if diastolic blood pressure w a s n o t decreased to 90 m m H g . T h e d u r a t i o n of t h e w h o l e t r e a t m e n t p h a s e w a s 8 w e e k s .
Blood P r e s s u r e , H o r m o n e s a n d I s o p r o t e r e n o l T e s t D u r i n g t h e r a p y , subjects h a d their blood pressure a n d h e a r t rate m e a s u r e d every 2 weeks, 24 to 26 h after their intake of t h e last Cilazapril dose, b e t w e e n 7:00 a n d 9:00 AM, after 10 m i n rest in t h e s u p i n e position a n d after 2 m i n in t h e s t a n d i n g position. D u r i n g t h e 4 last d a y s of t h e placebo a n d Cilazapril t r e a t m e n t p h a s e s , t h e follow
ing m e a s u r e m e n t s w e r e o b t a i n e d . A 24 h u r i n e collec tion w a s carried out to d e t e r m i n e s o d i u m , p o t a s s i u m , a n d creatinine excretion rates. Blood p r e s s u r e ( s t a n d a r d cuff a n d s p h y g m o m a n o m e t e r ; each v a l u e w a s t h e m e a n of three readings), h e a r t rate, e x c h a n g e a b l e s o d i u m , a n d p l a s m a s o d i u m , p o t a s s i u m , calcium, p h o s p h a t e , creati nine, uric acid, renin activity, angiotensin II (All), aldos terone, n o r e p i n e p h r i n e (NE), e p i n e p h r i n e , a n d atrial natriuretic p e p t i d e (ANP) w e r e d e t e r m i n e d after a n overnight fast a n d after 1 h of rest in t h e s u p i n e position (subjects took only t h e u s u a l m o r n i n g dose of placebo or
C i l a z a p r i l ) . Blood pressure, h e a r t rate, p l a s m a r e n i n ac tivity, All, aldosterone, NE, e p i n e p h r i n e , a n d A N P le vels w e r e m e a s u r e d again after t h e subjects h a d s p e n t 60 m i n walking. After e m p t y i n g t h e b l a d d e r , subjects rested in t h e s u p i n e position a n d a n isoproterenol sensi tivity test w a s p e r f o r m e d w i t h bolus injections accord ing to our s t a n d a r d p r o c e d u r e .1 3'1 4
N o r e p i n e p h r i n e a n d A n g i o t e n s i n II I n f u s i o n In order to test t h e subjects' pressor or a l d o s t e r o n e r e s p o n siveness, NE a n d All w e r e infused i n t r a v e n o u s l y 1 to 3 d a y s after t h e isoproterenol test according to our stan d a r d p r o c e d u r e .1 3 , 1 4
M e t h o d o l o g y P l a s m a a n d u r i n a r y s o d i u m w e r e m e a s u r e d by flame p h o t o m e t r y . Creatinine, uric acid a n d calcium concentrations w e r e m e a s u r e d b y a u t o a n a -lyzer, p h o s p h a t e b y colorimetric p h o s p h o m o l y b d a t e .
Plasma renin activity, aldosterone, All, a n d A N P w e r e d e t e r m i n e d b y r a d i o i m m u n o a s s a y1 5 - 1 8 a n d
p l a s m a NE a n d e p i n e p h r i n e concentrations w e r e o b tained using a r a d i o e n z y m a t i c m e t h o d ,1 9 as r e p o r t e d
e l s e w h e r e .2 0 Exchangeable s o d i u m w a s m e a s u r e d b y
isotope dilution t e c h n i q u e using 2 4N a .2 1 Cardiovascular
reactivity w a s a n a l y z e d b y calculation of t h r e s h o l d a n d pressor d o s e s1 3 , 1 4 a n d b y deriving d o s e - r e s p o n s e curves.
T h e chronotropic isoproterenol dose w a s derived using t h e d o s e - r e s p o n s e curve relating i s o p r o t e r e n o l - i n d u c e d i n c r e m e n t s of h e a r t rate to t h e isoproterenol d o s e s .2 2
Statistics Since t h e logarithmic transformation r a t h e r t h a n t h e absolute values followed a G a u s s i a n distribu tion, t h e n a t u r a l logarithmic transformation of p l a s m a renin activity, infused NE dosage, All or isoproterenol a n d pressor or t h r e s h o l d NE a n d All dosages, a n d chronotropic isoproterenol dosages w e r e u s e d for t h e statistical analysis. Statistical analysis included t h e paired S t u d e n t ' s two-tailed t test a n d t h e Wilcoxon test (comparison of p a i r e d values within groups), regression analysis, analyses of variance (comparison of v a l u e s a m o n g t h e groups) a n d covariance (comparison of d o s e - r e s p o n s e curves).
R E S U L T S
At t h e e n d of t h e placebo p h a s e , n o r m o t e n s i v e a n d h y pertensive subjects did n o t differ significantly in m e a n
350 B E R N A S C O N I E T A L AJH-APRIL 1991-VOL 4, NO. 4, PART 1
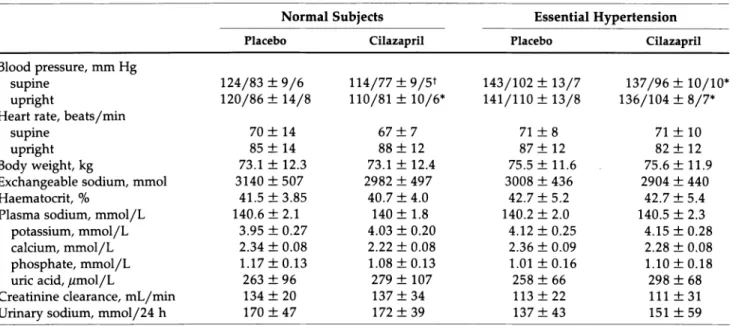
TABLE 1. CLINICAL AND BIOCHEMICAL FINDINGS BEFORE AND AFTER CILAZAPRIL IN NORMAL AND HYPERTENSIVE SUBJECTS (MEAN ± SD)
Normal Subjects Essential Hypertension
P l a c e b o C i l a z a p r i l P l a c e b o C i l a z a p r i l
Blood pressure, mm Hg
supine 124/83 ± 9 / 6 114/77 ± 9 / 5 * 143/102 ± 13/7 137/96 ± 10/10*
upright 120/86 ± 14/8 110/81 ± 10/6* 141/110 ± 13/8 136/104 ± 8 / 7 *
Heart rate, beats/min
supine 70 ± 14 67 ± 7 71 ± 8 71 ± 10
upright 85 ± 1 4 88 ± 12 87 ± 12 82 ± 12
Body weight, kg 73.1 ± 12.3 73.1 ± 12.4 75.5 ± 1 1 . 6 75.6 ± 1 1 . 9
Exchangeable sodium, mmol 3140 ± 5 0 7 2982 ± 497 3008 ± 436 2904 ± 440
Haematocrit, % 41.5 ± 3 . 8 5 40.7 ± 4 . 0 42.7 ± 5 . 2 42.7 ± 5 . 4
Plasma sodium, mmol/L 140.6 ± 2 . 1 140 ± 1.8 140.2 ± 2 . 0 140.5 ± 2.3
potassium, mmol/L 3.95 ± 0.27 4.03 ± 0.20 4.12 ± 0 . 2 5 4.15 ± 0 . 2 8
calcium, mmol/L 2.34 ± 0.08 2.22 ± 0.08 2.36 ± 0.09 2.28 ± 0.08
phosphate, mmol/L 1.17 ± 0 . 1 3 1.08 ± 0 . 1 3 1.01 ± 0 . 1 6 1.10 ± 0 . 1 8
uric acid, //mol/L 263 ± 96 279 ± 107 258 ± 66 298 ± 68
Creatinine clearance, mL/min 134 ± 20 137 ± 3 4 113 ± 2 2 111 ± 3 1
Urinary sodium, mmol/24 h 170 ± 4 7 172 ± 3 9 137 ± 4 3 151 ± 5 9
* Ρ < .025; t Ρ < .01 ν placebo values.
age (38 ± 1 0 i ? 4 5 ± 1 2 years), b o d y weight, e x c h a n g e able s o d i u m , h e a r t rate, p l a s m a or u r i n a r y electrolytes, a n d creatinine clearance (Table 1).
T h e dose of Cilazapril w a s increased after t w o treat m e n t w e e k s in n i n e of 11 p a t i e n t s ( m e a n d o s e 4.6 ± 1.0 mg); in order to h a v e a c o m p a r a b l e dosage, t h e dose w a s also increased in six of t h e n o r m a l subjects ( m e a n d o s e 3.8 ± 1 . 3 mg).
As c o m p a r e d w i t h t h e placebo p h a s e , Cilazapril d e creased s u p i n e a n d u p r i g h t arterial p r e s s u r e in b o t h s t u d y g r o u p s (Table 1). H e a r t rate, b o d y weight, p l a s m a a n d u r i n a r y electrolytes, a n d creatinine clearance w e r e u n c h a n g e d (Table 1). Exchangeable s o d i u m t e n d e d to
decrease, b u t in t h e individual g r o u p s t h e c h a n g e did n o t reach statistical significance.
R e n i n - A n g i o t e n s i n - A l d o s t e r o n e S y s t e m a n d R e a c t i v i t y to A l l As c o m p a r e d to placebo conditions, Cilaza pril caused a significant increase of s u p i n e a n d u p r i g h t p l a s m a r e n i n activity a n d a fall of u p r i g h t p l a s m a aldos t e r o n e in t h e t w o s t u d y groups; s u p i n e p l a s m a aldoster o n e decreased only in h y p e r t e n s i v e s (Table 2). P l a s m a All levels r e m a i n e d o n average u n c h a n g e d (Table 2).
As c o m p a r e d to placebo conditions, s u p i n e , preinfu sion p l a s m a All did n o t c h a n g e significantly after Cila zapril in t h e t w o s t u d y g r o u p s w h i l e p l a s m a aldosterone
TABLE 2. RENIN-ANGIOTENSIN-ALDOSTERONE SYSTEM AND REACTIVITY TO ANGIOTENSIN II BEFORE AND AFTER CILAZAPRIL (MEAN ± SD)
Normal Subjects Essential Hypertension
P l a c e b o C i l a z a p r i l P l a c e b o C i l a z a p r i l
Plasma Reinin Activity, n g / m L - h
supine 1.78
±
0.7 7.69±
5.92* 1.81±
1.31 4.95±
3.94*upright 5.29
±
2.03 31.54±
20.48t 4.20±
2.76 31.4±
34.5tPlasma Angiotensin II, pg/mL
supine 6.1
±
3.6 6.6±
2.0 8.7±
3.7 8.8±
4.7upright 13.1
±
7.9 9.9±
3.2 16.3±
10.6 13.9±
7.6Plasma Aldosterone, n g / d L
supine 7.2
±
2.9 6.2±
1.5 7.8±
2.1 6.2±
1.5*upright 13.1
±
7.9 9.9±
3.2* 16.3±
10.6 13.9±
7.6*Preinfusion plasma angiotensin II, pg/mL 7.7
±
4.5 8.3±
1.9 10.5±
2.4 8.5±
3.6 Angiotensin II threshold dose, n g / k g - m i n 1.12±
0.56 1.57±
1.45 0.83±
0.33 0.90±
0.62 Angiotensin II pressor dose, n g / k g · min 12.12±
6.5 8.92±
5.13 6.33±
2.4 7.0±
4.2AJH-APRIL 1991-VOL. 4, NO. 4, PART 1 P R E S S O R REACTIVITY 351
t e n d e d to fall slightly a l t h o u g h n o t significantly (Figure 1). After placebo, t h e pressor reactivity, as j u d g e d b y t h e All pressor a n d t h r e s h o l d doses, w a s slightly, b u t n o t significantly, lower in h y p e r t e n s i v e t h a n in n o r m a l s u b jects a n d did not c h a n g e after Cilazapril in t h e t w o s t u d y g r o u p s (Table 2). After placebo, in n o r m a l subjects, t h e increase in systolic blood pressure d u r i n g All infusion at t h e dose rate of 10 n g / k g · m i n ( + 22 ± 12 m m Hg) w a s associated w i t h a significant (P < .005) decrease of h e a r t rate (—9 ± 8 b e a t s / m i n ) ; in patients w i t h essential h y p e r t e n s i o n t h e A l l - i n d u c e d increase of systolic b l o o d p r e s s u r e ( + 3 1 ± 11 m m Hg) w a s n o t a c c o m p a n i e d b y a decrease of h e a r t rate (— 1 ± 6 b e a t s / m i n ) . T h e rela tionship b e t w e e n A l l - i n d u c e d increases in b l o o d p r e s sure a n d concomitant d e c r e m e n t s of h e a r t rate differed significantly b e t w e e n t h e t w o s t u d y g r o u p s (F = 21.2; Ρ < .01). After C i l a z a p r i l , h e a r t rate decreased d u r i n g
All infusion in n o r m a l ( + 26 ± 14 m m H g a n d —10 ± 6 b e a t s / m i n ) a n d h y p e r t e n s i v e subjects ( + 2 9 ± 16 m m H g a n d — 6 ± 4 b e a t s / m i n ; Ρ < .01) a n d t h e relation s h i p b e t w e e n A l l - i n d u c e d i n c r e m e n t s of blood pressure
a n d d e c r e m e n t s of h e a r t rate did n o t differ b e t w e e n t h e t w o s t u d y g r o u p s (F = 0.48).
T h e p l a s m a All levels m e a s u r e d at t h e e n d of each All infusion dose rate correlated closely w i t h t h e corre s p o n d i n g dose rate; t h e correlation w a s similar after placebo a n d Cilazapril in n o r m a l subjects (respectively: r = 0.87; Ρ < . 0 0 1 ; lny = 0.991nx + 2.76, a n d r = 0.87; Ρ < . 0 0 1 ; lny = 0.991nx + 2.89) a n d h y p e r t e n s i v e p a tients (r = 0.77; Ρ < . 0 0 1 ; lny = 0.891nx + 3.20 a n d r = 0.87; Ρ < . 0 0 1 ; lny = 1.061nx + 2.82). T h e relation ship b e t w e e n t h e A l l - i n d u c e d increases in diastolic arte rial pressure a n d p l a s m a All concentrations w a s n o t modified b y Cilazapril as c o m p a r e d w i t h placebo condi tions (F = 2.07 a n d 1.86; Ρ = NS) (Figure 1).
After placebo, All caused a significant increase of p l a s m a aldosterone in n o r m a l subjects a n d p a t i e n t s w i t h essential h y p e r t e n s i o n (Figure 1). After Cilazapril, t h e p l a s m a levels of aldosterone increased to a c o m p a r a b l e extent d u r i n g All infusion in n o r m a l subjects a n d in h y p e r t e n s i v e patients. T h e relationship b e t w e e n p l a s m a aldosterone a n d p l a s m a All concentration o b t a i n e d
Λ Diastolic B l o o d Pressure 3 0 η m m H g 2 0 10 N o r m a l S u b j e c t s Essential H y p e r t e n s i o n O Placebo • Cilazapril
o
J 6 10 2 0 5 0 1 0 0 2 0 0 4 0 0 6 10 2 0 5 0 1 0 0 2 0 0 4 0 0 P l a s m a A l d o s t e r o n e 3 0 2 0 1 0 n g / d l Placebo Δ Cilazapril A 7 10 2 0 ~50 1 0 0 2 0 0 4 0 0 7~10 2 0 ~FIGURE 1. Relationship between diastolic blood pressure or plasma al dosterone and plasma angiotensin II during angiotensin II infusion before and after Cilazapril in normal subjects (left panel) and patients with essential hypertension (right panel). Open sym bols indicate mean values after pla cebo; black symbols mean values after
Cilazapril. Bars indicate SEM. The
curves are not significantly different.
5 0 1 0 0 2 0 0 4 0 0 P l a s m a A n g i o t e n s i n II, p g / m l
352 B E R N A S C O N I ET AL AJH-APRIL 1991-VOL. 4, NO. 4, PART 1
d u r i n g ΑΠ infusion w a s n o t modified b y Cilazapril as c o m p a r e d to placebo conditions in t h e t w o s t u d y g r o u p s (F = 0.03 a n d 0.86; NS) (Figure 1).
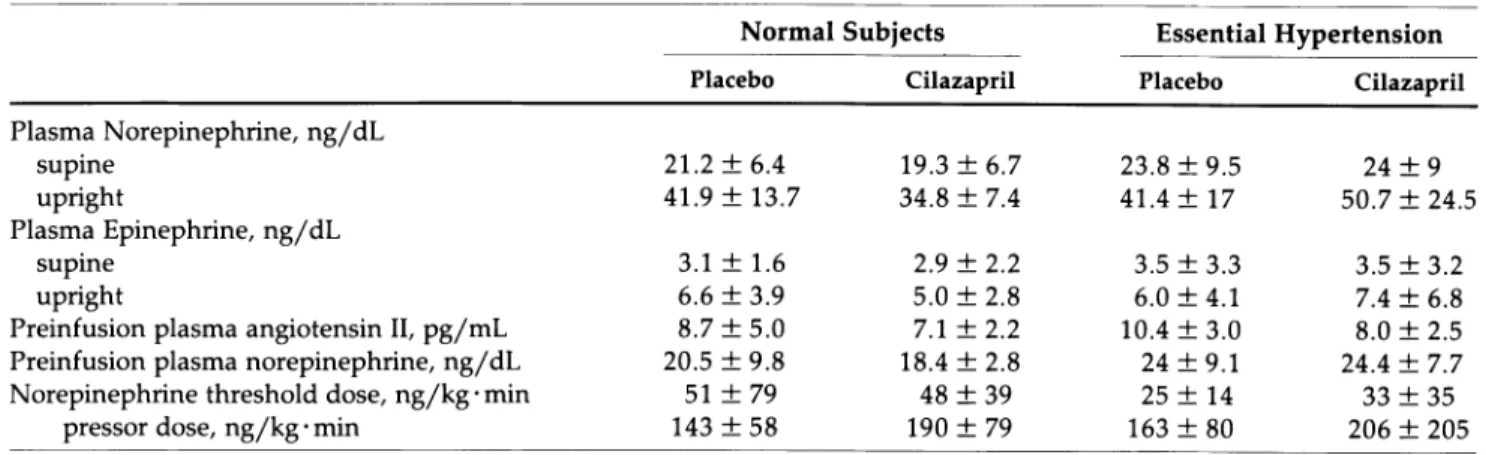
S y m p a t h e t i c N e r v o u s S y s t e m At t h e e n d of t h e pla cebo p h a s e , n o r m a l subjects a n d patients w i t h essential h y p e r t e n s i o n did n o t differ significantly in s u p i n e a n d u p r i g h t p l a s m a NE a n d e p i n e p h r i n e levels as well as in N E t h r e s h o l d a n d pressor doses (Table 3). Cilazapril did n o t modify either p l a s m a NE a n d e p i n e p h r i n e levels or t h e pressor reactivity to infused NE, as j u d g e d b y t h e NE t h r e s h o l d a n d pressor doses (Table 3).
U n d e r placebo conditions, t h e increase in systolic b l o o d p r e s s u r e d u r i n g NE infusion at t h e d o s e of 200 n g / k g · m i n w a s associated w i t h a significant d e crease of h e a r t rate in n o r m a l subjects ( + 30 ± 8 m m H g a n d — 8 ± 6 b e a t s / m i n ; Ρ < .01). H y p e r t e n s i v e patients r e s p o n d e d to a lower NE dose rate (100 n g / k g · min) w i t h a c o m p a r a b l e increase of arterial pressure a n d d e crease of h e a r t rate ( + 3 3 ± 9 m m H g a n d —6 ± 5 b e a t s / m i n ; Ρ < .025). After Cilazapril, t h e N E - i n d u c e d increase in m e a n blood pressure w a s a c c o m p a n i e d b y a similar decrease of h e a r t rate in t h e t w o s t u d y g r o u p s ( + 3 3 ± 10 m m H g a n d - 8 ± 6 b e a t s / m i n a n d + 3 6 ± 14 m m H g a n d — 5 ± 4 b e a t s / m i n , respectively). T h e relationship b e t w e e n t h e N E - i n d u c e d increases in arte rial p r e s s u r e a n d t h e c o n c o m i t a n t d e c r e m e n t s of h e a r t rate did n o t differ b e t w e e n n o r m a l a n d h y p e r t e n s i v e subjects u n d e r placebo conditions a n d it w a s unaffected b y Cilazapril (F = 0.06 to 0.46).
P l a s m a NE concentration, m e a s u r e d at t h e e n d of each NE infusion step, correlated closely w i t h t h e corre s p o n d i n g N E infusion rates a n d correlations w e r e simi lar in n o r m a l subjects before (r = 0.94; lny = 0.831nx + 1.5; Ρ < .001) a n d after (r = 0.98; lny = 0.931nx + 1.09; Ρ < .001) Cilazapril; t h e c o r r e s p o n d i n g correlations w e r e also c o m p a r a b l e in h y p e r t e n s i v e patients (r = 0.92; lny = 0 . 8 3 1 n x + 1 . 4 9 ; Ρ < .001 a n d r = 0.94;
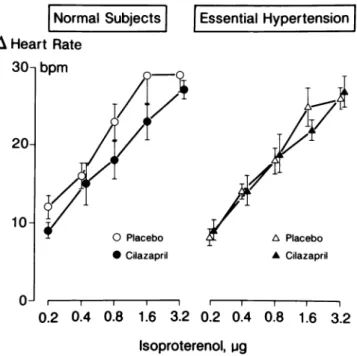
lny = 0 . 9 1 1 n x + 1 . 2 1 ; Ρ < .001). T h e concentration-r e s p o n s e cuconcentration-rve of aconcentration-rteconcentration-rial pconcentration-ressuconcentration-re a n d p l a s m a NE con centration w a s n o t modified b y Cilazapril in t h e t w o s t u d y g r o u p s as c o m p a r e d to placebo conditions (Fig u r e 2) ( F = 1 . 4 4 a n d 2.95). A t r i a l N a t r i u r e t i c P e p t i d e At t h e e n d of t h e placebo p h a s e , s u p i n e a n d u p r i g h t p l a s m a A N F levels w e r e lower (P < .05) in n o r m a l subjects (27.5 ± 19.4 a n d 18.6 ± 16.0 p g / m L ) t h a n in h y p e r t e n s i v e p a t i e n t s (52.5 ± 28.5 a n d 38.3 ± 20.5 p g / m L ) . There w a s n o c h a n g e after Cilazapril, w i t h a persistent elevation in h y p e r t e n s i v e s (30.5 ± 21.3 a n d 19.8 ± 13.3 p g / m L in n o r m a l subjects ν 62.5 ± 39.1 a n d 34.3 ± 15.1 p g / m L in h y p e r t e n s i v e patients). S e n s i t i v i t y to I s o p r o t e r e n o l C h r o n o t r o p i c effects of isoproterenol, as j u d g e d b y t h e m e a n t h r e s h o l d a n d chronotropic doses, w e r e c o m p a r a b l e b e t w e e n n o r m a l a n d h y p e r t e n s i v e subjects (0.3 ± 0.3 a n d 1.6 ± 1.5 //g ν 0.2 + 0.2 a n d 1.8 ± 1.3 //g). Both variables w e r e u n c h a n g e d after Cilazapril (0.4 ± 0.7 a n d 1.3 ± 1.1 //g in n o r m a l subjects, 0.2 + 0.2 a n d 2.0 ± 1.5 //g in h y p e r tensive patients) (Figure 3).
With respect to d o s e r e s p o n s e curves, t h e h e a r t r a t e -isoproterenol relationships w e r e similar in n o r m a l a n d h y p e r t e n s i v e subjects after placebo (Figure 3). After Ci lazapril, the d o s e r e s p o n s e curve w a s slightly, n o n s i g -nificantly displaced to t h e right in n o r m a l subjects (F = 3.47; Ρ = NS) a n d w a s u n c h a n g e d in h y p e r t e n s i v e s (F = 0.002; Ρ = NS).
S i d e Effects Side effects w e r e n o t r e p o r t e d b y n o r m a l a n d h y p e r t e n s i v e subjects, except for t h e report of mild c o u g h b y o n e h e a l t h y m a n . T h e hematological a n d bio chemical control p a r a m e t e r s did n o t c h a n g e d u r i n g the study, except for a transient slight increase of t h e s e r u m aspartate a n d alanine aminotransferase in o n e n o r m a l subject.
TABLE 3. PLASMA CATECHOLAMINES AND NOREPINEPHRINE INFUSION BEFORE AND AFTER CILAZAPRIL (MEAN ± SD)
Normal Subjects Essential Hypertension
P l a c e b o C i l a z a p r i l P l a c e b o C i l a z a p r i l Plasma Norepinephrine, n g / d L supine 21.2
±
6.4 19.3±
6.7 23.8±
9.5 24±
9 upright 41.9±
13.7 34.8±
7.4 41.4±
17 50.7±
24.5 Plasma Epinephrine, n g / d L supine 3.1±
1.6 2.9±
2.2 3.5±
3.3 3.5±
3.2 upright 6.6±
3.9 5.0±
2.8 6.0±
4.1 7.4±
6.8Preinfusion plasma angiotensin II, pg/mL 8.7
±
5.0 7.1±
2.2 10.4±
3.0 8.0±
2.5 Preinfusion plasma norepinephrine, n g / d L 20.5±
9.8 18.4±
2.8 24±
9.1 24.4±
7.7 Norepinephrine threshold dose, n g / k g - m i n 51±
79 48±
39 25±
14 33±
35AJH-APRIL 1991-VOL 4, NO. 4, PART 1 P R E S S O R R E A C T I V I T Y 353 Δ Mean B l o o d Pressure 3 0 - 1 m m Hg 20H 10 Normal Subjects O Placebo • Cilazapril Essential Hypertension Δ Placebo ι 1 1 1 — 10 2 0 3 0 5 0 100 2 0 0 6 0 0 1 0 2 0 3 0 5 0 100 2 0 0 Plasma Norepinephrine, ng/dl 6 0 0
FIGURE 2. Relationship between mean blood pressure and plasma nor epinephrine during norepinephrine infusion before and after Cilazapril in
normal subjects (left panel) and pa
tients with essential hypertension (right panel). Open symbols indicate mean values after placebo; black sym bols mean values after Cilazapril. Bars indicate SEM. The curves are not sig nificantly different.
D I S C U S S I O N
T h e findings of t h e p r e s e n t s t u d y indicate t h a t t h e b l o o d p r e s s u r e lowering effect of a n 8 w e e k converting e n z y m e inhibition w i t h t h e long acting c o m p o u n d Cilaza pril w a s n o t a c c o m p a n i e d b y modifications of t h e p h y s i ological relationship b e t w e e n t h e e n d o g e n o u s nor adrenergic activity a n d t h e cardiovascular pressor
reac-Normal Subjects Essential H y p e r t e n s i o n
Δ H e a r t Rate 30-, b p m 2 0 10 O Placebo • Cilazapril Δ Placebo • Cilazapril 1 1 1 1 ι 1 1 1 1 0.2 0. 4 0.8 1.6 3.2 0.2 0. 4 0.8 1.6 3.2 Isoproterenol, u g
FIGURE 3. Dose response curves for isoproterenol-induced in creases in heart rate before and after Cilazapril in normal subjects (left panel) and patients with essential hypertension (right panel). Open symbols indicate mean values after placebo; black symbols mean values after Cilazapril. Bars indicate SEM. The curves are not significantly different.
tivity to N E . Despite c o n c o m i t a n t r e n i n activation a n d a l d o s t e r o n e s u p p r e s s i o n , as indices of effective convert ing e n z y m e inhibition, t w o angiotensin I I - d e p e n d e n t p a t h w a y s , t h e cardiovascular pressor reactivity a n d t h e a d r e n a l release of aldosterone, w e r e u n a l t e r e d . P l a s m a levels of A N F w e r e also u n c h a n g e d . O n t h e o t h e r h a n d , a t e n d e n c y for s u p p r e s s e d p l a s m a a l d o s t e r o n e a n d b o d y s o d i u m depletion m a y identify t w o contributory factors in t h e h y p o t e n s i v e m e c h a n i s m of converting e n z y m e inhibition.
Cilazapril, given for 8 w e e k s , significantly decreased arterial p r e s s u r e in b o t h n o r m a l a n d h y p e r t e n s i v e s u b jects, w i t h o u t modification of t h e h e a r t rate, t h e c h r o n o tropic r e s p o n s e to a s s u m p t i o n of t h e u p r i g h t p o s t u r e , isoproterenol injection or, as d e m o n s t r a t e d in a p r e v i o u s study, to e x e r c i s e .2 3 T h e decrease of h e a r t rate d u r i n g
acute, N E - i n d u c e d elevation of arterial p r e s s u r e w a s also u n c h a n g e d , p o i n t i n g to a n u n a l t e r e d baroreflex s e n sitivity. In our h y p e r t e n s i v e patients, t h e bradycardie r e s p o n s e to All infusion w a s f o u n d to b e b l u n t e d after placebo a n d n o r m a l after Cilazapril. T h e m e a n i n g of this observation is unclear. A dissociation b e t w e e n a n o r m a l h e a r t rate r e s p o n s i v e n e s s to N E a n d a b l u n t e d r e s p o n s e to All is n o t a feature of h y p e r t e n s i v e patients a n d w a s n o t o b s e r v e d previously in our l a b o r a t o r y .1 3 O n t h e
o t h e r h a n d , Cilazapril did n o t alter t h e h e a r t rate re s p o n s e to All in n o r m a l subjects, despite t h e significant decrease of arterial pressure. In single dose studies, Cila zapril did n o t modify h e a r t rate, s y m p a t h e t i c n e r v o u s activity a n d baroreflex sensitivity, b u t e n h a n c e d p a r a s y m p a t h e t i c a c t i v i t y ,2 4 suggesting a w i t h d r a w a l of t h e
vagolytic actions of AIL Similar findings w e r e r e p o r t e d after administration of other c o m p o u n d s s u c h as C a p t o pril or e n a l a p r i l ,1 4 , 2 5 indicating a similar cardiovascular
354 B E R N A S C O N I ET A L AJH-APRIL 1991-VOL 4, NO. 4, PART 1
N o r a d r e n e r g i c activity a n d pressor reactivity to NE did n o t c h a n g e in b o t h n o r m a l a n d h y p e r t e n s i v e s u b jects after Cilazapril. P l a s m a NE a n d e p i n e p h r i n e levels w e r e r e p o r t e d to b e u n c h a n g e d after Captopril2 6'2 7 or e n a l a p r i l .2 8 T h e pressor effects to infused NE, studied
after s h o r t - t e r m converting e n z y m e blockade (up to 2 weeks) w a s n o t e d to b e b l u n t e d2 9 or u n c h a n g e d .3 0 , 3 1 A
limited sensitivity of t h e pressor r e s p o n s e curves w i t h o u t c o n c o m i t a n t m e a s u r e m e n t s of t h e p l a s m a NE con centration could, at least partly, explain these discrepan cies. After m o r e p r o l o n g e d t r e a t m e n t , t h e pressor reactivity r e m a i n e d u n c h a n g e d in n o r m a l subjects b u t in patients w i t h essential h y p e r t e n s i o n a decrease of t h e slope of t h e pressor r e s p o n s e curve to NE w a s r e p o r t e d .2 8 In t h e latter investigation, t h e b l u n t e d pressor
reactivity to NE e m e r g e d only at very h i g h concentra tions of p l a s m a NE, w h i l e at physiological or m o d e r ately elevated levels t h e r e s p o n s i v e n e s s of b l o o d p r e s sure to N E w a s n o r m a l .
Body s o d i u m , m e a s u r e d in patients w i t h essential or renovascular h y p e r t e n s i o n , w a s r e p o r t e d to b e u n c h a n g e d after Captopril or e n a l a p r i l .1'8 In contrast, a
slight decrease w a s r e p o r t e d in 16 h y p e r t e n s i v e patients treated for 6 w e e k s w i t h e n a l a p r i l .2 8 In t h e p r e s e n t
s t u d y , exchangeable s o d i u m t e n d e d to decrease in b o t h n o r m a l a n d h y p e r t e n s i v e subjects. It a p p e a r s possible t h a t a decrease of p l a s m a aldosterone m a y h a v e in fluenced s o d i u m metabolism. H o w e v e r , a fall in p l a s m a a l d o s t e r o n e w a s n o t o b s e r v e d in all studies w i t h con verting e n z y m e inhibitors, since after s u p p r e s s i o n in t h e early p h a s e , p l a s m a a l d o s t e r o n e t e n d s to rise in t h e chronic p h a s e of t r e a t m e n t .3 2 This p a t t e r n of a d r e n a l
r e s p o n s e m a y reflect t h e complex regulation of aldos t e r o n e secretion, since in addition to All, o t h e r m o d u l a t ing factors s u c h as s o d i u m a n d p o t a s s i u m b a l a n c e are potentially influenced b y converting e n z y m e inhibi t i o n .1
T h e profile of t h e r e n i n - a n g i o t e n s i n - a l d o s t e r o n e sys t e m after Cilazapril w a s characterized b y u n c h a n g e d All levels, a m a r k e d l y stimulated p l a s m a r e n i n activity, a n d a t e n d e n c y for decreased p l a s m a a l d o s t e r o n e concen tration. T h e failure to detect a persistent d e c r e m e n t of circulating All d u r i n g chronic converting e n z y m e inhibi tion w i t h Cilazapril or o t h e r c o m p o u n d s2 8 m a y b e at least
partly related to crossreactivity of h i g h angiotensin I levels in t h e r a d i o i m m u n o a s s a y of A I L1 O n t h e o t h e r
h a n d , activation of angiotensin I m a y partly o v e r c o m e t h e competitive inhibition of converting e n z y m e .3 3 T h e
association of u n c h a n g e d p l a s m a All levels a n d d e creased p l a s m a a l d o s t e r o n e levels m a y s u p p o r t t h e p o s sibility of a dissociation in t h e r e n i n - a n g i o t e n s i n - a l d o s t e r o n e axis. This m a y reflect t h e partly different regulation of t h e t w o h o r m o n e s a n d h a s b e e n r e p o r t e d u n d e r o t h e r circumstances, such as a rapid c h a n g e in dietary s o d i u m i n t a k e .3 4 U n c h a n g e d p l a s m a All levels
w e r e associated w i t h u n c h a n g e d pressor a n d a d r e n a l
responses to AIL T h u s , it w o u l d a p p e a r t h a t after chronic converting e n z y m e inhibition t h e r e n i n - a n g i o tensin system m a y b e able to recover, at least partly, a physiological acute regulation of t h e pressor a n d a l d o s t e r o n e regulating p a t h w a y s . This m a y also imply t h a t u n d e r these circumstances t h e All receptor n u m b e r a n d t h e receptor-agonist affinity are n o t modified. Previous data in t h e literature are consistent w i t h this h y p o t h e s i s ; after acute blockade w i t h converting e n z y m e t h e r e is a n acute fall of p l a s m a All w i t h a n e n h a n c e d r e s p o n s e of blood pressure or p l a s m a aldosterone to infused A I L2 9-3 1
U n d e r m o r e chronic conditions, 1 to 8 w e e k s of treat m e n t w i t h Captopril, t h e pressor reactivity to All w a s n o t m o d i f i e d .1 4 , 3 5 After 6 w e e k s of t r e a t m e n t w i t h enalapril,
t h e acute aldosterone r e s p o n s e to infused All w a s u n c h a n g e d in n o r m a l a n d h y p e r t e n s i v e s u b j e c t s .2 8
Plasma A N F concentration w e r e significantly ele v a t e d in the p r e s e n t g r o u p of p a t i e n t s w i t h essential h y p e r t e n s i o n . This could n o t b e explained b y differ ences in age or renal function. Cilazapril did n o t alter p l a s m a A N F levels in t h e t w o s t u d y g r o u p s . This s u g gests t h a t Cilazapril is a n effective a n t i h y p e r t e n s i v e agent, w i t h a cardiovascular profile c o m p a r a b l e to t h a t of other available converting e n z y m e inhibitors. Its m e c h a n i s m of action m a y b e partly related to s o d i u m depletion a n d aldosterone suppression, b u t n o t to m o d i fications of s y m p a t h e t i c - d e p e n d e n t p r e s s u r e regula tion, atrial natriuretic p e p t i d e concentration, or All d e p e n d e n t p a t h w a y s for acute blood p r e s s u r e or aldosterone regulation.
A C K N O W L E D G M E N T S
We acknowledge the technical assistance of Gudrun Haueter, Ruth Mosimann, Elisabeth Oldenberg, Stephanie Schwenk, Ritva Takkinen, and Jane Boden, and the secretarial assistance of Daniela Lazzaretti.
R E F E R E N C E S
1. Atkinson AB, Morton JJ, Brown JJ, et al: Captopril in clinical hypertension. Changes in components of renin-angiotensin system and in body composition in relation to fall in blood pressure with a note on measurement of angiotensin II during converting enzyme inhibition. Br Heart J 1980;44:290-296.
2. Waeber B, Brunner HR, Brunner DB, et al: Discrepancy between antihypertensive effect and angiotensin con verting enzyme inhibition by C a p t o p r i l . Hypertension
1980;2:236-242.
3. Johnston CI, Mendelsohn FAO, Cubela RB, et al: Inhibi tion of angiotensin converting enzyme (ACE) in plasma and tissues: studies ex vivo after administration of ACE inhibitors. J Hypertens 1988;6(suppl 3):S17-S22. 4. Johnston CL, Clappison BH, Anderson WP, Yasujiman
M: Effect of angiotensin converting enzyme inhibition on circulating local kinin levels. Am J Cardiol 1982;49:1401-1404.
AJH-APRIL 1991-VOL. 4, NO. 4, PART 1 P R E S S O R R E A C T I V I T Y 355
effects of angiotensin converting enzyme inhibitors and other antihypertensive drugs. Cardiovasc Drugs Ther 1987;1:39-43.
6. Antonaccio MJ, Kerwin L: Pre- and post-junctional inhi bition of vascular sympathetic function by Captopril in spontaneously hypertensive rats. Hypertension 1981;3(suppl 1):154-162.
7. Philipp T, Distler A, Cordes U: Sympathetic nervous sys tem and blood pressure control in essential hyperten sion. Lancet 1978;ii:959-963.
8. Bauer JH, Gaddy P: Effects of enalapril alone, and in combination with hydrochlorothiazide, on renin-angio tensin-aldosterone, renal function, salt and water excre tion, and body fluid composition. Am J Kidney Dis 1985;6:222-232.
9. Natoff IL, Nixon JS, Francis RJ, et al: Biological properties of the angiotensin-converting enzyme inhibitor Cilaza pril. J Cardiovasc Pharmacol 1985;7:569-580. 10. Francis RJ, Brown AN, Kler L, et al: Pharmacokinetics of
the converting enzyme inhibitor Cilazapril in normal vol unteers and the relationship to enzyme inhibition: devel opment of a mathematical model. J Cardiovasc Pharma col 1987;9:32-38.
11. Shionoiri H, Gotoh E, Takagi N, et al: Antihypertensive effects and pharmacokinetics of single and consecutive doses of Cilazapril in hypertensive patients with normal and impaired renal function. J Cardiovasc Pharmacol 1988;11:242-249.
12. Weidmann Ρ, Beretta-Piccoli C, Ziegler WH, et al: Age versus urinary sodium for judging renin, aldosterone and catecholamine levels: studies in normal subjects and patients with essential hypertension. Kidney Int 1978;14:619-628.
13. Weidmann Ρ, Beretta-Piccoli C, Link L, et al: Cardiovas cular conterregulation during sympathetic inhibition in normal subjects and patients with mild hypertension. Hypertension 1983;5:873-880.
14. Beretta-Piccoli C, Ziegler WH, Antonini P, et al: Cardio vascular regulation during converting enzyme inhibition with Captopril in diabetes-associated hypertension. J Hypertens 1990;8:671-678.
15. Sealey JE, Gerten-Banes J, Laragh JH: The renin system: variations in man measured by radioimmunoassay. Kid ney Int 1972;1:240-253.
16. Düsterdieck GO, McElwee G: Estimation of angiotensin II concentration in human plasma by radioimmunoas say: some applications to physiological and clinical states. Eur J Clin Invest 1971;2:32-38.
17. Malvano R, Gandolfi C, Gianessi D, et al: Radioimmuno assay of aldosterone in crude plasma extracts. J Nucl Biol Med 1976;20:37-44.
18. Weidmann Ρ, Gnädinger MP, Ziswiler HR, et al: Cardio vascular, endocrine and renal effects of atrial natriuretic pepetide in essential hypertension. J Hypertens 1986;4(suppl 2):S71-S83.
19. Da Prada M, Zürcher G: Simultaneous radioenzymatic determination of plasma and tissue adrenaline, nora drenaline and dopamine within the fentomole range. Life Sei 1976;19:1161-1174.
20. Beretta-Piccoli C, Weidmann P, Boehringer K, et al: Re lationship between plasma aldosterone and angiotensin
II before and after noradrenergic inhibition in normal subjects and patients with mild essential hypertension. J Clin Endocrinol Metab 1984;59:316-320.
21. Beretta-Piccoli C, Weidmann Ρ: Body sodium-blood vol ume state in non-azotemic diabetes mellitus. Miner Elec trolyte Metab 1982;7:36-47.
22. Cleaveland CR, Rango RE, Shand DG: A standardized isoproterenol sensitivity test. Arch Intern Med 1972;130:47-52.
23. White WB, McCabe EJ, Hager WD, Schulman P: The effects of the long-acting angiotensin-converting en zyme inhibitor Cilazapril on casual, exercise, and ambula tory blood pressure. Clin Pharmacol Ther 1988; 1 7 3 -178.
24. Elliott HL, Ajayi AA, Ried JL: The influence of Cilazapril on indices of autonomic function in normotensives and hypertensives. Br J Clin Pharmacol 1989;27:3035-3075. 25. Ried JL, Millar HA, Campbell BC: Enalapril and auto
nomic reflexes and exercise performance. J Hypertens 1983;l(suppl 1):129-134.
26. Niarchos AP, Pickering TG, Morganti A, Laragh JH: Plasma catecholamines and cardiovascular responses during converting enzyme inhibition in normotensive and hypertensive man. Clin Exp Hypertens [A] 1982;4:761-789.
27. Muiesan G, Alicandri CL, Agabiti-Rosei A, et al: Angio tensin-converting enzyme inhibition, catecholamines and hemodynamics in essential hypertension. Am J Car diol 1982;49:1420-1424.
28. Uehlinger D, Ferrier C, Weidmann P, et al: Antihyper tensive contribution of sodium depletion and the sympa thetic axis during chronic angiotensin II converting en zyme inhibition. J Hyperten 1989;7:901-907.
29. Imai Y, Abe K, Seino M, et al: Attenuation of pressor responses to norepinephrine and pitressin and potentia tion of pressor response to angiotensin II by Captopril in human subjects. Hypertension 1982;4:444-451. 30. Vierhapper H, Witte PV, Waldhäusl W: Unchanged
pressor effect of norepinephrine in normal man follow ing the oral administration of two angiotensin convert ing enzyme inhibitors, Captopril and HOE 498. J Hyper tens 1986;4:9-11.
31. Koletsky RJ, Gordon MB, LeBoff MS, et al: Captopril enhances vascular and adrenal responsiveness to angio tensin II in essential hypertension. Clin Sei 1984;66:299-305.
32. Staessen J, Lijnen P, Fagard R, et al: Rise of plasma aldos terone during long-term Captopril treatment (letter). New Engl J Med 1981;304:1110.
33. Giese J, Rasmussen S, Nielsen MD, Ibsen M: Biochemical monitoring of vasoactive peptides during angiotensin converting enzyme inhibition. J Hypertens 1983; 1 (suppl l):31-36.
34. Rogacz S, Williams GH, Hollenberg NK: Time courses of enhanced adrenal responsiveness to angiotensin on a low salt diet. Hypertens 1990;15:376-380.
35. Fruncillo J, Rotmensch HH, VTasses PH, et al: Effect of Captopril and hydrocholorothiazide on the response to pressor agents in hypertensives. Eur J Clin Pharmacol 1985;28:5-9.