RESEARCH ARTICLE
Persistent Correlation of Ghrelin Plasma Levels with Body
Mass Index Both in Stable Weight Conditions and during
Gastric-bypass-induced Weight Loss
J. Ybarra&E. Bobbioni-Harsch&G. Chassot&
O. Huber&Ph. Morel&F. Assimacopoulos-Jeannet&
A. Golay
Received: 22 July 2008 / Accepted: 6 October 2008 / Published online: 31 October 2008
# Springer Science + Business Media, LLC 2008 Abstract
Background Studies done on serial changes in plasma ghrelin levels after gastric bypass (GBP) have yielded contrasting results since decreased, unchanged, or increased levels have been reported in the literature. This study investigates whether or not GBP has an inhibitory effect on fasting ghrelin levels independently of weight loss. Methods Fasting ghrelin levels were measured in 115 stable body weight females, classified as normal body weight
(NW; body mass index (BMI) <25 kg/m2), overweight
(OW; BMI 25–30 kg/m2
), and obese subjects, divided in
three subgroups with increasing BMI (BMI 30–40 kg/m2
;
BMI 40–50 kg/m2; BMI >50 kg/m2).
Results Each obese subgroup showed significantly lower ghrelin levels as compared to both NW (p<0.0001) and OW subjects (p<0.05 or 0.005); however, no significant differences were observed within the three obese subgroups. Forty-nine obese patients underwent a GBP. Plasma ghrelin, measured at 3, 6, and 12 months after GBP, significantly
increased from the sixth month on (p <0.0001). When patients were classified, at each postoperative time point, according to their actual BMI, ghrelin was significantly (p=0.0002) related to postoperative BMI and not signifi-cantly different from ghrelin measured in stable body weight conditions.
Conclusions Fasting ghrelin displays an inversely significant correlation with BMI in both stable body weight conditions and after GBP. No evidence was found that GBP had an effect on fasting ghrelin levels, independent of weight loss. Keywords Ghrelin . BMI . Obesity . Body weight loss . Gastric bypass
Introduction
Obesity is becoming a major public health problem
world-wide [1] and most dietary and/or pharmacologic approaches
end up in failure and/or recidivism. Hence, weight reduction by bariatric surgery techniques have been increasingly used to prevent and reduce its comorbidities [2,3].
Gut hormone profiles following bariatric surgery favor an anorectic state, improve metabolic parameters (i.e., insulin resistance, glycemic control, dyslipidemia), convey appetite reduction, and facilitate long-term changes in body weight (BW) [4,5].
The only known peripheral hormone with orexigenic action, the gastroenteric peptide ghrelin, apparently coun-terbalances energy homeostasis in opposition to multiple
anorectic signals (NPY, AGRP, POMC, GABA, etc.) [6].
Ghrelin, which predominantly targets the same neuronal
structures on which leptin and PYY [7–9] exert their action,
even induces a positive energy balance resulting in increased adiposity. Since ghrelin is secreted in response
J. Ybarra
Instituto de Cardiología Avanzada, Centro Medico Teknon, Barcelona, Spain
E. Bobbioni-Harsch (*)
:
A. GolayService of Therapeutic Education for Chronic Diseases, Geneva University Hospital,
1211 Geneva, Switzerland e-mail: [email protected] G. Chassot
:
O. Huber:
P. MorelClinic of Digestive Surgery, Geneva University Hospital, Geneva, Switzerland
F. Assimacopoulos-Jeannet
Department of Cell Physiology and Metabolism, Geneva Medical School,
to caloric restriction and its expression and secretion are rapidly suppressed by food intake, it has been proposed to play a physiological role in meal initiation as the
endogenous“hunger hormone.” [10]
The medical literature reveals a lack of consensus regarding serial changes in ghrelin levels after gastric bypass. Hence, several studies have shown that Roux-en-Y Gastric Bypass (RYGBP) in human patients causes a decrease in circulating levels of ghrelin [11–14].
Converse-ly, other authors report unchanged [15] or even increased
ghrelin levels after bariatric surgery. [16]
Furthermore, a recently developed clinically relevant rat model of RYGBP claims that postoperative weight loss is correlated with the magnitude of the decrease in circulating ghrelin levels. This correlation provides the strongest evidence to date that altered ghrelin signaling contributes to weight loss after this operation [17].
These contradictory results tend to suggest that regula-tion of this hormone is complex and subject to genetic and other patient-related miscellaneous factors.
The present study was undertaken to: (1) measure ghrelin fasting levels in a cohort of female subjects in conditions of stable body weight and with a wide range of body mass index (BMI), (2) to analyze the postoperative evolution of ghrelin levels in the function of the concom-itant modifications of the BMI, and (3) to compare the postoperative ghrelin values with those measured in weight-stable subjects having similar age and BMI.
Materials and Methods
A cohort of 115 females (age 40±1 years old, range 18–64) participated in the study which had been previously approved by the local Ethical Committee. The subjects were examined in conditions of stable body weight and classified according to their BMI as normal body weight
(N=21; BMI<25 kg m−2), overweight (N=10; BMI 25–
29.9 kg m−2), obese (N=22; BMI 30–40 kg m−2), morbidly
obese (N=41; BMI 40–50 kg m−2), and massively obese
(N=21, BMI>50 kg m−2). The stability of body weight—
anamnestically established—was defined as no changes in body weight greater than 5% of the actual body weight, in the last 6 months. In these subjects, anthropometric parameters as well as plasma ghrelin were measured in fasting conditions. Among the 84 obese subjects, a subgroup of 49 patients underwent a gastric bypass surgery (RYGBP). In these patients, we evaluated both BMI and fasting ghrelin at 3, 6, and 12 months after surgery. At each time point, the patients were classified according to their actual BMI, as was done in stable body weight conditions. Fasting plasma ghrelin was assessed by commercial kit (Phoenix Pharmaceutical, CA, USA).
Simple regression analysis, factorial analysis of variance (ANOVA), or ANOVA for repeated measurements was utilized for statistical analysis. The percent of excess BMI lost (%EBL) and the percent of excess weight loss (%EWL) were calculated according to the formula in a recent report
[18, 19]. The change in body weight (%Δ body weight)
was calculated as preoperative BW minus postoperative BW divided by preoperative BW times 100.
All p values were two-tailed with 0.05 specified as statistical significance. All statistical analyses were per-formed with statistical software (SPSS version 10.0 for Windows, SPSS, Chicago, IL, USA).
Results
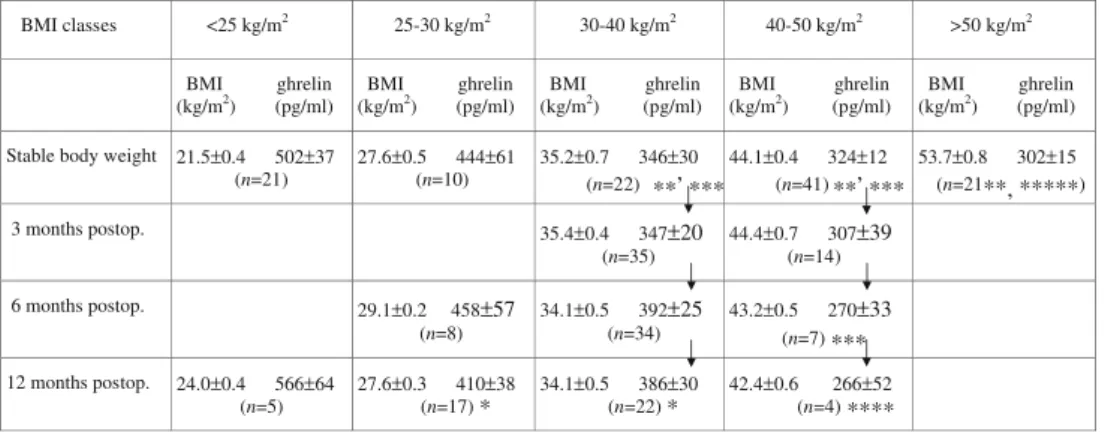
Plasma ghrelin levels (pg/ml) as measured in different BMI
classes (kg/m2) both in stable body weight conditions and
during gastric-bypass-induced body weight loss appear
illustrated in Table1. As shown, the three obese subgroups
showed fasting ghrelin levels significantly lower than those measured in both normal body weight and overweight subjects. No significant differences were observed within the three obese groups.
The 49 surgically treated patients were further divided into subgroups according to the BMI that they had reached at each postoperative time point.
Three months after surgery, 35 patients out of 49 were classified in the obese group and 14 in the morbidly obese group. No statistically significant differences were observed in mean plasma ghrelin between these two groups.
Six months after surgery, eight patients had reached a BMI of overweight; 34 were classified as obese while seven remained in the morbidly obese group. A significant difference was observed in ghrelin values between the overweight and morbidly obese groups (458±57 vs. 270± 33 pg/ml, respectively; p<0.02).
One year after surgery, patients having attained a normal body weight displayed the highest ghrelin levels (566± 64 pg/ml, n=5). This value was significantly different from the ones measured in all the other groups (p<0.05 vs. overweight group; p<0.02 vs. obesity group; and p<0.004 vs. morbidly obese group) but otherwise similar to ghrelin levels in stable body weight normal-weight (N < 25) individuals (502±37 pg/ml).
By using factorial ANOVA, no significant differences were found between ghrelin values measured postopera-tively in the different BMI classes and plasma ghrelin measured in the corresponding BMI classes in conditions of
stable body weight (Table1, follow vertical arrows).
Figure 1a depicts a significant robust negative
relation-ship between BMI and ghrelin levels (r2=0.88; p<0.0002),
the identical significant negative relationship using
postop-erative BMI and ghrelin values (r2=0.87; p=0.0002).
The simultaneous serial changes in BMI, ghrelin, and percentage of excess weight loss (EWL) occurring in the 49
patients submitted to RYGBP are depicted in Table2. As
shown, RYGBP resulted in a 38.5% and 55% excess weight loss at 6 (p<0.001) and 12 months (p<0.0001), respective-ly. Simultaneously, ghrelin levels increased significantly by 19% and 22.8% at 6 (p<0.0001) and 12 months (p< 0.0001), respectively. Finally, BMI decreased by 24.3% and 31.1% at 6 and 12 months, respectively.
Discussion
The most novel finding in our study is the persistent inverse correlation between fasting ghrelin levels and BMI along the 12 months following RYGBP. In our series, fasting total
ghrelin levels increased by 22.8% in the 12 months following RYGBP when compared to baseline values. Besides, no evidence was found that RYGBP surgery had an effect on fasting total ghrelin levels, independent of weight loss.
Our results (Table 1, Fig. 1a,b) disclose a significant
inverse correlation between fasting ghrelin levels and BMI across a wide BMI range (from normal body weight to morbidly obese patients) in agreement with previous reports [20,21] stating that the circulating concentration of ghrelin is determined by body weight in first instance.
All current bariatric surgeries result in weight loss of large magnitude, correction of comorbidities, and excellent
short- and long-term outcomes [3, 22, 23]. Together with
the spectacular weight loss seen in bariatric surgery, endocrine changes take place, particularly after laparoscop-ic RYGBP (LRYGB).
Since ghrelin seems to play a key role in the complicated energy balance loop, it is logical to hypothesize that its
Table 1 Plasma ghrelin levels (pg/ml) as measured in different BMI classes (kg/m2) both in stable body weight conditions and during gastric-bypass-induced body weight loss
BMI classes <25 kg/m2 25-30 kg/m2 30-40 kg/m2 40-50 kg/m2 >50 kg/m2 BMI ghrelin (kg/m2) (pg/ml) BMI ghrelin (kg/m2) (pg/ml) BMI ghrelin (kg/m2) (pg/ml) BMI ghrelin (kg/m2) (pg/ml) BMI ghrelin(kg/m2) (pg/ml)
Stable body weight 21.5±0.4 502±37
(n=21) 27.6±0.5 444±61 (n=10) 35.2±0.7 346±30 (n=22) **, *** **, *** 44.1±0.4 324±12 (n=41) 53.7±0.8 302±15 (n=21**, *****) 3 months postop. 35.4±0.4 347±20 (n=35) 44.4±0.7 307±39 (n=14) 6 months postop. 29.1±0.2 458±57 (n=8) 34.1±0.5 392±25 (n=34) 43.2±0.5 270±33 (n=7) *** **** 12 months postop. 24.0±0.4 566±64 (n=5) 27.6±0.3 410±38 (n=17) * 34.1±0.5 386±30 (n=22) * 42.4±0.6 266±52 (n=4)
*p<0.04 or 0.01 (factorial ANOVA), significantly different from BMI<25 (normal body weight); **p<0.2008 (factorial ANOVA), significantly different from BMI<25 (normal body weight); ***p<0.04 or 0.01 (factorial ANOVA), significantly different from BMI 25–30 (overweight); ****p<0.005 (factorial ANOVA), significantly different from BMI<25 (normal body weight); *****p<0.005 (factorial ANOVA), significantly different from BMI 25–30 (overweight)
Fig. 1 a Scatterplot between BMI and ghrelin levels in stable body weight conditions (base-line). R: Pearson’s coefficient. b Scatterplot between BMI and ghrelin levels postoperatively. R: Pearson’s coefficient
changes after surgery could affect the success of the operation.
As a result of bariatric surgery, energy intake is markedly decreased; patients experience decreased hunger, early fullness, and enhanced satiety. Moreover, the ingested food bypasses important parts of the digestive system because of the decreased food transit time, resulting in partial
malabsorption and a total negative energy balance. [24,25].
Postoperatively, ghrelin levels depend on the functional integrity of the remaining fundus, the size of the gastric pouch [26,27], the length of the Roux limb or biliopancreatic limb
[16, 28], and/or the adaptive responses of body weight
homeostasis [10, 20, 29, 30]. Because ghrelin levels have
been shown to be low after LRYGB in some studies [20,30,
31–36], it has been proposed that lower ghrelin levels may
contribute to the success of some surgical weight loss
procedures, including LRYGB [14, 15, 20] and possibly
laparoscopic adjustable gastric banding [30]. However, data
have been inconsistent [10,12,15,16,25,37]. Cummings et al. [10,20], in a cross-sectional study, was the first to report low total plasma ghrelin concentrations in five obese patients 9–31 months after LRYGB, who were still obese, compared with those in a group of matched obese controls.
Our bariatric population disclosed a marked decrease in BMI in agreement with the majority of LRYGBP
prospec-tive studies [3, 22, 23]. One would expect the massive
decrease in BMI achieved with these surgeries to trigger an elevation in ghrelin levels. Noteworthy, four out of the 13
studies of patients who underwent LRYGB [15,16,37,38]
showed an increase in ghrelin levels after surgery whereas nine have shown a paradoxical reduction in plasma ghrelin levels. It is possible that these different outcomes depend on how and when the postoperative samples were taken (i. e., whether subjects were actively losing weight or had achieved a stable lower BMI), as well as the differences in surgical techniques across centers. Thus, it is difficult to reconcile the existing data and formulate a conclusion as to the effect of LRYGB on ghrelin release.
Our bariatric population disclosed postoperative
ghre-lin values (see Table 2) in agreement with those reported
by Holdstock et al. [16], who, in a prospective study of 66
patients, reported increased ghrelin levels at 6 (+44%) and 12 (+62%) months after LRYGB compared to the preoperative levels. Interestingly, postoperative ghrelin increments in our series were more modest (+19% and 22.8%, respectively). On the contrary, excess weight loss was more prominent at 6 and 12 months postoperatively
(−38.5%, −55.5%, ours, respectively vs. −22%, −30%,
Holdstock, respectively). Circulating ghrelin levels in our bariatric patients continue to be primarily produced by the disconnected stomach and the control of the ghrelin-producing endocrine cells seems to remain unaltered. Thus, it is the lowered caloric intake and the resulting weight loss rather than RYGBP surgery that affects ghrelin levels. These changes are all related to changes in BMI and reflect the new state of energy balance achieved.
Last but not least, fasting ghrelin values in our series are indistinguishable between stable body weight and actively losing weight participants provided they share the same
BMI category (Table 1, vertical arrows), stressing the
underlying specific influence of BMI on fasting ghrelin
values, in agreement with previous reports [20,21].
Should we still pay attention to ghrelin in the context of bariatric surgery? The majority of authors agree upon the fact that ghrelin is an important determinant of energy homeostasis, a peripherally secreted orexigenic hormone acting in key central pathways, with measurable levels demonstrating meal-to-meal variation. Noteworthy, to our knowledge, no study to date has demonstrated that ghrelin levels postoperatively are predictors of success in patients
after LRYGB [36].
Our study limitations include lack of postprandial ghrelin levels and of measurements of the active form— acylated ghrelin levels [31,39]. In future studies, it should also be important to investigate ghrelin levels in parallel satiety scales, as well as simultaneous evaluation of other gut hormones interfering with appetite control such as glucagon-like peptide 1, gastric inhibitory peptide, PYY, and cholecystokinin, among others.
Table 2 Evolution of BMI (kg/m2) and fasting ghrelin (pg/ml), measured before, 3, 6, and 12 months after surgery (RYGBP), in a subgroup of 49 obese subjects submitted to a gastric bypass
BMI (kg/m2) Ghrelin (pg/ml) %EWL
Before surgery 45.7±0.8 329±15 0
3 months postop. 38.0±0.7* 338±19 38.5±1.3
6 months postop. 34.6±0.7* 390±22** 55.5±2.0
12 months postop. 31.5±0.7* 404±23* 71.4±2.9
*p<0.0001, significantly different from preoperative values (ANOVA for repeated measurements); **p<0.001, significantly different from preoperative values (ANOVA for repeated measurements)
Conflicts of interest None to disclose.
References
1. Seidell JC. Obesity, insulin resistance and diabetes—a worldwide epidemic. Br J Nutr 2000;83(Suppl 1):S5–8.
2. DeMaria EJ. Bariatric surgery for morbid obesity. N Engl J Med 2007;356:2176–83.
3. Buchwald H, Avidor Y, Braunwald E, et al. Bariatric surgery: a systematic review and meta-analysis. JAMA 2004;292:1724–37. 4. Gumbs AA, Modlin IM, Ballantyne GH. Changes in insulin
resistance following bariatric surgery: role of caloric restriction and weight loss. Obes Surg 2005;15:462–73.
5. le Roux CW, Aylwin SJ, Batterham RL, et al. Gut hormone profiles following bariatric surgery favor an anorectic state, facilitate weight loss, and improve metabolic parameters. Ann Surg 2006;243:108–14.
6. Horvath TL, Diano S, Sotonyi P, et al. Minireview: ghrelin and the regulation of energy balance—a hypothalamic perspective. Endocrinology 2001;142:4163–9.
7. Bray GA. Afferent signals regulating food intake. Proc Nutr Soc 2000;59:373–84.
8. Jeanrenaud B, Rohner-Jeanrenaud F. CNS–periphery relationships and body weight homeostasis: influence of the glucocorticoid status. Int J Obes Relat Metab Disord 2000;24(Suppl 2):S74–6. 9. Schwartz MW, Woods SC, Porte D Jr, et al. Central nervous
system control of food intake. Nature 2000;404:661–71. 10. Cummings DE, Shannon MH. Roles for ghrelin in the regulation
of appetite and body weight. Arch Surg 2003;138:389–96. 11. Nijhuis J, van Dielen FM, Buurman WA, et al. Ghrelin, leptin and
insulin levels after restrictive surgery: a 2-year follow-up study. Obes Surg 2004;14:783–7.
12. Stoeckli R, Chanda R, Langer I, et al. Changes of body weight and plasma ghrelin levels after gastric banding and gastric bypass. Obes Res 2004;12:346–50.
13. Langer FB, Reza Hoda MA, Bohdjalian A, et al. Sleeve gastrectomy and gastric banding: effects on plasma ghrelin levels. Obes Surg 2005;15:1024–9.
14. Geloneze B, Tambascia MA, Pilla VF, et al. Ghrelin: a gut-brain hormone effect: of gastric bypass surgery. Obes Surg 2003;13:17–22. 15. Faraj M, Havel PJ, Phélis S, et al. Plasma acylation-stimulating protein, adiponectin, leptin, and ghrelin before and after weight loss induced by gastric bypass surgery in morbidly obese subjects. J Clin Endocrinol Metab 2003;88:1594–602.
16. Holdstock C, Engström B, Ohrvall M, et al. Ghrelin and adipose tissue regulatory peptides: effect of gastric bypass surgery in obese humans. J Clin Endocrinol Metab 2003;88:3177–83. 17. Stylopoulos N, Davis P, Pettit JD, et al. Changes in serum ghrelin
predict weight loss after Roux-en-Y gastric bypass in rats. Surg Endosc 2005;19:942–6.
18. Deitel M, Greenstein RJ. Recommendations for reporting weight loss. Obes Surg 2003;13:159–60.
19. Deitel M, Gawdat K, Melissas J. Reporting weight loss. Obes Surg 2007;17:565–8.
20. Cummings DE, Frayo RS, Purnell JQ, et al. Plasma ghrelin levels after diet-induced weight loss or gastric bypass surgery. N Engl J Med 2002;346:1623–30.
21. Tschop M, Weyer C, Tataranni PA, et al. Circulating ghrelin levels are decreased in human obesity. Diabetes 2001;50:707–9. 22. Maggard MA, Shugarman LR, Suttorp M, et al. Meta-analysis:
surgical treatment of obesity. Ann Intern Med 2005;42:97–118. 23. Sugerman HJ, Kral JG. Evidence-based medicine reports on
obesity surgery: a critique. Int J Obes Relat Metab Disord 2005;29:735–74.
24. Trostler N, Mann A, Zilberbush N, et al. Weight loss and food intake 18 months following vertical banded gastroplasty or gastric bypass for severe obesity. Obes Surg 1995;5:39–51.
25. Brolin RE. Bariatric surgery and long-term control of morbid obesity. JAMA 2002;288:2793–6.
26. Fruhbeck G, Diez Caballero A, Gil MJ. Fundus functionality and ghrelin concentrations after bariatric surgery. N Engl J Med 2004;15:308–9.
27. Fruhbeck G, Gil MJ, Cienfuegos JA, et al. The decrease in plasma ghrelin concentrations following bariatric surgery depends on the functional integrity of the fundus. Obes Surg 2004;14:606–12.
28. Choban PS, Flancbaum L. The effect of Roux limb lengths on outcome after Roux-en-Y gastric bypass: a prospective, random-ized clinical trial. Obes Surg 2002;12:540–5.
29. Cummings DE, Shannon MH. Ghrelin and gastric bypass: is there a hormonal contribution to surgical weight loss? J Clin Endocrinol Metab 2003;88:2999–3002.
30. Leonetti F, Iacobellis G, Di Mario U, et al. Different plasma ghrelin levels after laparoscopic gastric bypass and adjustable gastric banding in morbid obese subjects. J Clin Endocrinol Metab 2003;88:4227–31.
31. Korner J, Cirilo LJ, Wardlaw SL, et al. Effects of Roux-en-Y gastric bypass surgery on fasting and postprandial concentrations of plasma ghrelin, peptide YY, and insulin. J Clin Endocrinol Metab 2005;90:359–65.
32. Tritos NA, Mun E, Bertkau A, et al. Serum ghrelin levels in response to glucose load in obese subjects post-gastric bypass surgery. Obes Res 2003;11:919–24.
33. Lin E, Fugate K, Smith CD, et al. The effects of gastric surgery on systemic ghrelin levels in the morbidly obese. Arch Surg 2004;139:780–4.
34. Morínigo R, Moizé V, Vidal J, et al. Short-term effects of gastric bypass surgery on circulating ghrelin levels. Obes Res 2004;12:1108–16.
35. Fruhbeck G, Hernandez-Lizoain JL, Cienfuegos JA, et al. Fasting plasma ghrelin concentrations 6 months after gastric bypass are not determined by weight loss or changes in insulinemia. Obes Surg 2004;14:1208–15.
36. Christou NV, Look D, McLean AP. Pre- and post-prandial plasma ghrelin levels do not correlate with satiety or failure to achieve a successful outcome after Roux-en-Y gastric bypass. Obes Surg 2005;15:1017–23.
37. Pope GD, Birkmeyer JD, Finlayson SR. National trends in utilization and in-hospital outcomes of bariatric surgery. J Gastrointest Surg 2002;6:855–60.
38. Vendrell J, Broch M, Richart C, et al. Resistin, adiponectin, ghrelin, leptin, and proinflammatory cytokines: relationships in obesity. Obes Res 2004;12:962–71.
39. Kojima M, Hosoda H, Date Y, et al. Ghrelin is a growth-hormone-releasing acylated peptide from stomach. Nature 1999;402:656– 60.