Standards for CHERG reviews of intervention effects on child survival
Texte intégral
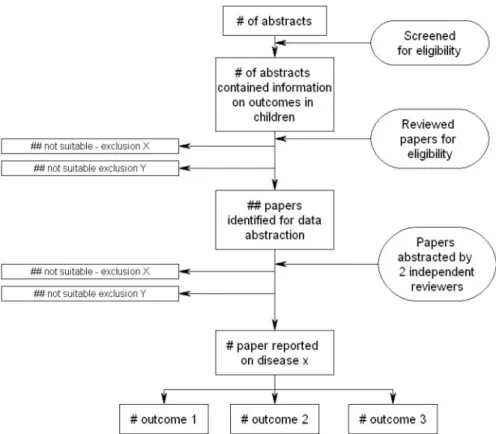
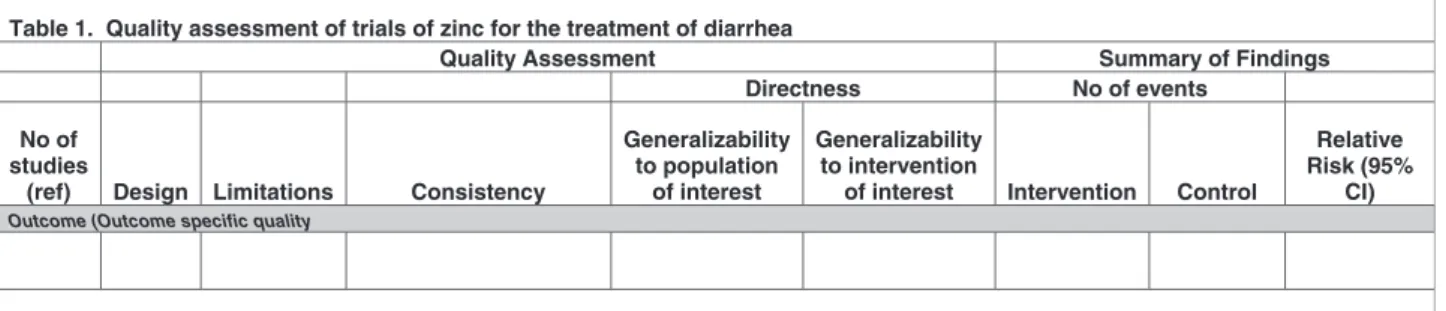
Figure

Documents relatifs
The anthropological theory of the didactic (hereafter ATD) is at the same time a theory in the scientific usual meaning of the term, that is, an organised
Across traditional bullying (both direct and indirect forms) and cyberbullying (through mobile phones and the internet), the most commonly reported victim emotion was anger (Ortega
First, we expand the shape-spaces definition to any spaces repre- sented by the graph G (V, E) where the vertices set V corresponding to the nodes set of a hierarchical
Here we propose, instead of carrying out a full computation for each point of the surface, to use the capability of the LATIN method to re-utilize the solution to a given problem
Combining statistical and expert evidence using belief functions: Application to centennial sea level estimation taking into account climate change... Combining statistical and
An exploratory workshop was held at a French University of Technology to study the development of new engineering training courses on issues of strong sustainability.. During
For a particular soil profile it has been found that values of AF derived from GRNN approach are closer to that of 1D linear viscoelastic seismic analysis particularly if the number
The stereo kernel [6] which compares the minimal stereo subgraphs of two ordered graphs has one drawback : graph information are reduced to a bag of subgraphs without taking
