Characterization of Long-term Continuous Electrodermal
Activity Lateralization in Pediatric Epilepsy Patients
The MIT Faculty has made this article openly available.
Please share
how this access benefits you. Your story matters.
Citation
Poh, M. Z., et al. "Characterization of Long-Term Continuous
Electrodermal Activity Lateralization in Pediatric Epilepsy Patients."
in Abstracts from the 2009 Annual Meeting of the American Epilepsy
Society. Epilepsia, 50(Suppl. 11):11-12, 2009
As Published
http://dx.doi.org/10.1111/j.1528-1167.2009.02377.x
Publisher
Wiley-Blackwell
Version
Original manuscript
Citable link
http://hdl.handle.net/1721.1/57433
Terms of Use
Attribution-Noncommercial-Share Alike 3.0 Unported
Detailed Terms
http://creativecommons.org/licenses/by-nc-sa/3.0/
63rd Annual Meeting of the American Epilepsy Society Boston, MA, USA
December 4-8, 2009
Epilepsia (2009)
Characterization of Long-term Continuous Electrodermal Activity Lateralization in
Pediatric Epilepsy Patients
Ming-Zher Poh1,2, Tobias Loddenkemper, MD3, Nicholas C. Swenson2, Mangwe C. Sabtala2,
Joseph R. Madsen, MD4, Rosalind W. Picard, ScD2.
1Harvard-MIT Division of Health Sciences and Technology, Cambridge, MA, United States, 02139; 2The
Media Laboratory, Massachusetts Institute of Technology, Cambridge, MA, United States, 02139; 3Division
of Epilepsy and Clinical Neurophysiology, Department of Neurology, Children's Hospital Boston, Boston, MA,
United States, 02115 and 4Neurosurgery, Children's Hospital Boston, Boston, MA, United States, 02115.
RATIONALE: Electrodermal activity (EDA) reflects sympathetic activation within the autonomic
nervous system. Activity within prefrontal cortices and limbic structures strongly influence ipsilateral EDA (Critchley HD Neuroscientist 2002;8:132-42). This relationship suggests that unilateral dysfunction of cortical activity may affect the direction of EDA lateralization. We hypothesized that hemispheric location of seizure onset in patients with epilepsy may be related to ipsilaterally increased sympathetic skin response as evidenced by EDA asymmetry.
METHODS: EDA of 22 patients undergoing long-term video/EEG monitoring were recorded
continuously from the ventral side of bilateral distal forearms using custom-built skin conductance sensors for 1-4 days. EDA recordings were lowpass filtered (1024 points, Hamming window, cutoff 0.016 Hz) to obtain skin conductance levels (SCL). Right/left differences were calculated in order to determine fR>L, the frequency of right-sided EDA lateralization (R > L), fL>R, the frequency
of left-sided EDA lateralization (L > R) and fR=L, the frequency of EDA symmetry (R = L).
Differences less than 0.05 µS were considered as R = L. The frequency of right/left EDA lateralization was compared within patients with a right (n = 6) and left-sided (n = 12) irritative zone or seizure onset zone respectively. To examine the role of handedness on EDA lateralization, the frequency of right/left EDA lateralization was also compared within both right (n = 13) and left-handed (n = 3) patients (handedness of 2 patients was unknown). Statistics were computed with MATLAB using the Wilcoxon rank sum test.
RESULTS: 18 patients (11 males, 7 females) between ages 4-20 years with unilateral irritative
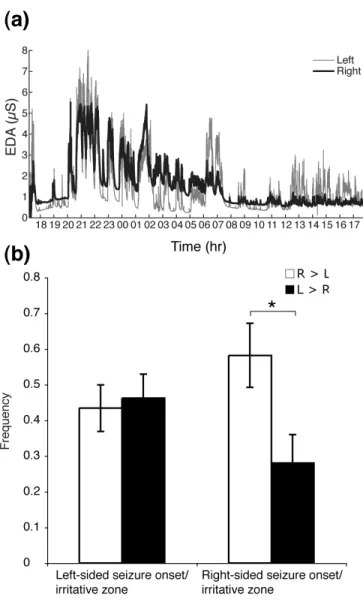
zone or unilateral seizure onset on scalp EEG as determined by long-term video/EEG monitoring were included. 13 patients were right-handed, 3 were left-handed, and in 2 handedness was undetermined. There were 12 and 6 patients with a left and right-sided ictal onset/irritative zone respectively. For patients with a left-sided seizure onset zone or irritative zone, the mean fR>L
(0.43 ± 0.23) was not significantly different from the mean fL>R (0.46 ± 0.23). However, for patients
with a right-sided seizure onset, the mean fR>L (0.58 ± 0.22) was higher than the mean fL>R (0.28 ±
0.20) (p < 0.05). Neither right nor left-handed patients nor patients with right or left MRI lesions displayed significantly different frequency of right/left EDA lateralization.
CONCLUSIONS: We present the first characterization of lateralization in long-term continuous
bilateral EDA in patients with epilepsy. Our pilot series suggests a relationship between hemispheric location of seizure onset/irritative zone and EDA lateralization. Frequency of right/left EDA lateralization may potentially provide additional lateralizing information regarding seizure onset zone or irritative zone on EEG in the presurgical assessment of epilepsy patients. Further studies regarding localizing and lateralizing value are currently underway.
Epilepsia (2009)
2
Table 1. Clinical characteristics and recorded data of patients with epilepsy
Case Age
(yrs)
Sex
Handed-ness
MRI findings Ictal onset zone /
Irritative zone on EEG
%L>R %R>L Duration (days)
1 4 F Rt. Lt. temporal lobe
cortical dysplasia
Lt. frontotemporal 39 50 2
2 14 M Rt. Normal Lt. centrotemporal and
parietal 82 16 1 3 6 F Rt. Normal Lt. temporal predominance 39 59 2 4 9 M Lt. Lt. temporal lobe cortical dysplasia Lt. temporal occipital 48 48 1
5 7 M Lt. Lt. MCA infarct Lt. frontotemporal 40 50 2
6 6 M Lt. Lt. MCA infarct Lt. hemisphere 87 1 1
7 9 M - Lt. cerebellar
hemisphere volume loss
Lt. posterior quadrant 65 26 1 8 14 F Rt. Normal Lt. frontotemporal 39 32 3 9 18 M Rt. Lt. precentral sulcus cortical malformation Lt. hemisphere 22 58 2 10 9 F - Normal Lt. temporal 8 82 1
11 6 M Lt. Normal Lt. posterior quadrant 56 34 1
12 10 F Lt. Lt. temporal lobe cortical dysplasia Lt. temporal 29 66 4 13 10 F Rt. Rt. mesial occipital dysplasia Rt. posterior quadrant 17 56 3 14 20 M Rt. T2 prolongation in occip periventricular white matter Rt. frontocentral 41 42 3 15 9 M Rt. Rt. temporal lobe volume loss Rt. parietal occipital 60 25 2 16 15 M Rt. Normal Rt. frontocentral 17 74 1 17 14 F Rt. Normal Rt. temporal 6 86 1 18 5 M - Cortical tubers, subependymal nodules Rt. occipital 27 67 1
Epilepsia (2009)
3
Figure 1. a) Example of 24 hr bilateral EDA recording (b) Comparison of frequency of
right/left EDA lateralization within patients with unilateral seizure onset. * indicates statistical significance (p<0.05). Error bars represent 1 S.E.M.