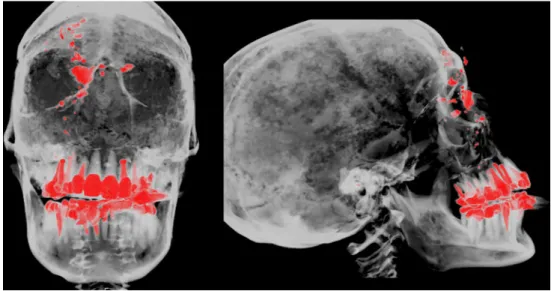
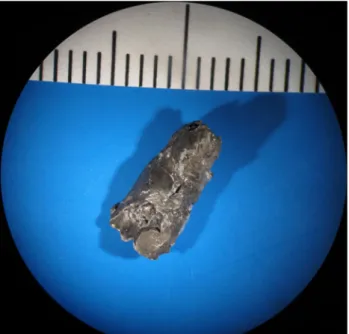
Incidental occult gunshot wound detected by postmortem computed tomography
Texte intégral
Figure
Documents relatifs
Pour certains historiens, cela se traduit par le fait que l’humain n’est pas seulement un objet de l’histoire, mais aussi un sujet, c’est-à-dire qu’il peut prendre une
Zonal annual mean changes in total water path (sum of liquid and ice water path), total cloud cover, total precipitation, shortwave, longwave and net shortwave radiation at
Data management and GIS in the Center for Disaster Management and Risk Reduction Technology (CEDIM): from integrated spatial data to the mapping of risk.. Natural Hazards and
Écris une expression littérale qui permet de calculer le montant total de la collection
The following properties of the tools were extracted and mapped in a structured way: approach (explicit, implicit), development method (consensus technique, expert panel, lit-
[r]
Indeed, the way Sterne experiments when he produces his associations between the past and the present (indeed when he creates a fictional past in order to make a
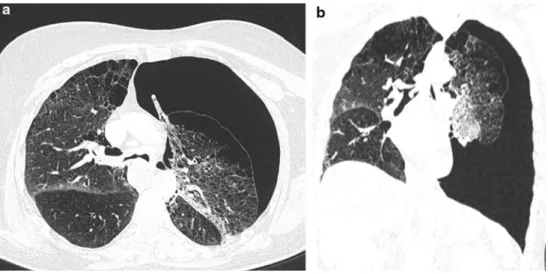
The aim of our study was to analyse the relationships between the mention of pulmonary nodules in the diagnostic report drafted by the radiologist having performed the
