. . . .
. . . .
Biodegradable polymer drug-eluting stents
reduce the risk of stent thrombosis at 4 years
in patients undergoing percutaneous coronary
intervention: a pooled analysis of individual
patient data from the ISAR-TEST 3,
ISAR-TEST 4, and LEADERS randomized trials
Giulio G. Stefanini
1†, Robert A. Byrne
2†, Patrick W. Serruys
3, Antoinette de Waha
2,
Bernhard Meier
1, Steffen Massberg
2, Peter Ju¨ni
4, Albert Scho¨mig
2,
Stephan Windecker
1,3, and Adnan Kastrati
2*
1
Department of Cardiology, Bern University Hospital, Bern, Switzerland;2
Deutsches Herzzentrum, Technische Universita¨t, Lazarettstraße 36, 80636 Munich, Germany;
3
Thoraxcenter, Erasmus University, Rotterdam, Netherlands; and4
Clinical Trials Unit, Bern University Hospital, Bern, Switzerland Received 21 January 2012; revised 5 March 2012; accepted 7 March 2012; online publish-ahead-of-print 24 March 2012
Aims The efficacy of durable polymer drug-eluting stents (DES) is delivered at the expense of delayed healing of the
stented vessel. Biodegradable polymer DES aim to avoid this shortcoming and may potentially improve long-term clinical outcomes, with benefit expected to accrue over time. We sought to compare long-term outcomes in patients treated with biodegradable polymer DES vs. durable polymer sirolimus-eluting stents (SES).
Methods and results
We pooled individual patient data from three large-scale multicentre randomized clinical trials (TEST 3, ISAR-TEST 4, and LEADERS) comparing biodegradable polymer DES with durable polymer SES and assessed clinical out-comes during follow-up through 4 years. The efficacy endpoint of interest was target lesion revascularization and the safety endpoint of interest was definite stent thrombosis. Out of 4062 patients included in the present analysis, 2358 were randomly assigned to treatment with biodegradable polymer DES (sirolimus-eluting, n ¼ 1501; biolimus-eluting, n ¼ 857) and 1704 patients to durable polymer SES. No heterogeneity across the trials was observed in analyses of the primary and secondary endpoints. At 4 years, the risk of target lesion revascularization was significantly lower among patients treated with biodegradable polymer DES vs. durable polymer SES (hazard ratio 0.82, 95% CI 0.68 – 0.98, P ¼ 0.029). In addition, the risk of stent thrombosis was significantly reduced with biodegradable polymer DES vs. durable polymer SES (hazard ratio 0.56, 95% CI 0.35 – 0.90, P ¼ 0.015), driven by a lower risk of very late stent thrombosis (hazard ratio 0.22, 95% CI 0.08 – 0.61, P ¼ 0.004). In keeping with this, in landmark analysis between 1 and 4 years, the incidence of myocardial infarction was lower for patients treated with biodegradable polymer DES vs. durable polymer SES (hazard ratio 0.59, 95% CI 0.73 – 0.95, P ¼ 0.031).
Conclusion Biodegradable polymer DES improve safety and efficacy compared with durable polymer SES during long-term
follow-up to 4 years.
-Keywords Biodegradable polymer † Biolimus A9 † Drug-eluting stent † Meta-analysis † Sirolimus † Stent thrombosis
†G.G.S. and R.A.B. contributed equally.
*Corresponding author. Tel:+49 89 1218 4577, Fax: +49 89 1218 4053, Email:[email protected]
Introduction
Drug-eluting stents (DES) with controlled release of anti-proliferative drugs from durable polymer coatings provide potent suppression of neointimal hyperplasia and markedly reduced the risk of repeat revascularization compared with bare metal
stents.1–3However, the use of early generation durable polymer
DES was associated with an increased risk of very late (.1 year)
stent thrombosis compared with bare metal stents.4–6 Animal
experiments, human autopsy studies, and investigation of throm-bosed DES specimens using intravascular ultrasound demonstrated that very late ST is related to delayed arterial healing and remodelling
of the stented vessel owing to ongoing inflammation.7–11The
per-sistence of durable polymer coatings after completion of the drug release has been implicated as a potential culprit for this
chronic inflammatory response.8,12,13
Biodegradable polymer-based DES, with controlled drug-release followed by subsequent degradation of the polymer coating, may potentially improve long-term clinical outcomes after coronary stenting, by rendering the stent surface similar to that of a bare metal stent and free of a chronic inflammatory stimulus. Biodegrad-able polymer-based DES have been established as a safe and effect-ive alternateffect-ive to durable polymer-based stent platforms as
evidenced in several randomized clinical trials.14–17Moreover, an
optical coherence tomography study suggested improved healing of the stented coronary segment following treatment with bio-degradable polymer DES compared with durable polymer
sirolimus-eluting stents (SES) at 9 months.18However, the
poten-tial clinical advantage of biodegradable polymer DES over durable polymer DES may be expected to emerge first after long-term follow-up, where the incidence of late adverse events related to impaired vessel healing—such as stent thrombosis—is hypothe-sized to be lower. Against this background, we pooled results from the three largest randomized clinical trials comparing
bio-degradable polymer DES with durable polymer SES14–16
incorpor-ating clinical follow-up to 4 years.
Methods
Patient population
We performed a patient-level pooled analysis of the three largest mul-ticentre, randomized clinical trials comparing biodegradable polymer DES with durable polymer SES for coronary revascularization: the ISAR-TEST 3 trial (ClinicalTrials.gov identifier: NCT00350454),14the ISAR-TEST 4 trial (ClinicalTrials.gov identifier: NCT00598676),15and the LEADERS trial (ClinicalTrials.gov identifier: NCT00389220).16A total of 4062 patients were included in the present analysis, 2358 of these were randomly allocated to treatment with biodegradable polymer DES [n ¼ 1501, sirolimus-eluting (Yukon Choice, stent back-bone produced by Translumina, Hechingen, Germany); n ¼ 857, biolimus-eluting (BioMatrix Flex, Biosensors Inc., Newport Beach, CA, USA)] and 1704 patients to durable polymer SES (Cypher Select, Cordis, Miami Lakes, FL, USA). Detailed descriptions relating to the design of the three trials are reported in the primary publications;14–16 a summary of the principal trial characteristics is reported in Table1.
Patients were followed up clinically out to 4 years after enrolment by the investigating sites.
Procedural and discharge medications
In all three trials, an oral dose loading dose of 300 – 600 mg clopidogrel was administered before or at the time of the procedure. During the procedure, all patients received unfractionated heparin or bivalirudin, whereas the use of glycoprotein IIb/IIIa antagonists was left at the dis-cretion of the operators. All patients were discharged on acetylsalicylic acid of at least 75 mg daily indefinitely and clopidogrel 75 mg daily for at least 6 months in the ISAR-TEST 3 and ISAR-TEST 4 trials, and at least 12 months in the LEADERS trial.
Endpoints and definitions
The efficacy endpoint of interest of the present analysis was target lesion revascularization; the safety endpoint of interest was definite stent thrombosis. Additional endpoints analysed were all-cause mortal-ity, cardiac death, myocardial infarction, and definite or probable stent thrombosis. Target lesion revascularization was defined as any clinically indicated repeat revascularization (percutaneous or surgical) of the target lesion. The definition of clinically indicated revascularization was consistent across the included trials. Cardiac death was defined as death due to immediate cardiac causes or complications related to the procedure, as well as any death in which a cardiac cause could not be excluded. Myocardial infarction in the ISAR-TEST 4 trial refers to target-vessel myocardial infarction; in the ISAR-TEST 3 and LEADERS trials, any myocardial infarction was included. Stent thrombosis was defined according to the Academic Research Consor-tium criteria.19
Trial quality assessment
All trials were assessed for bias using components recommended by the Cochrane Collaboration,20including sequence generation of the al-location; allocation concealment; blinding of participants, personnel, and outcome assessors; selective outcome reporting; and other sources of bias. Trials with high or unclear risk for bias for any one of the first three components were considered as trials with high risk of bias. Otherwise, they were considered as trials with low risk of bias.
Statistical analysis
Continuous data are presented as mean (+SD) or median (25th – 75th percentiles). Categorical data are presented as counts and proportions (%). Meta-analysis was performed on individual patient data according to intention to treat. We performed survival analyses using the Mantel – Cox method stratified by the trial. Trials in which the event of interest was not observed in either treatment group were omitted from the analysis of that event. In case only one of the groups of an individual trial had no event of interest, the estimate of treatment effect estimate and its standard error were calculated after adding 0.5 to each cell of the 2× 2 table for that trial.21We used the Cochran test to assess heterogeneity across trials. Also, we calculated the I2statistic to measure the consistency between trials with values of 25, 50, and 75% showing respectively, low, moderate, and high inconsistency.22 Hazard ratios from individual trials were pooled using the DerSimonian and Laird method for random effects.23Results were considered statistically significant at two-sided P , 0.05. Statistical analysis was performed using the Stata software, version 9.2 (Stata Corp, College Station, TX, USA). Survival curves
. . . .
. . . . Table 1 Summary of included trials
Study No. of patients
Stent type
Patients pooled in the current analysis according to the stent type
Primary endpoint Inclusion criteria
Exclusion criteria Baseline characteristics Clinical Lesion Mean age,
years (SD) Male, % ACS, % Diabetes, % Clinical follow-up Angiographic follow-up ISAR-TEST 3 605 DP SES BP SES PF SES DP SES (n ¼ 202) BP SES (n ¼ 202)
In-stent late luminal loss Symptoms or evidence of ischaemia Acute MI, cardiogenic shock In-stent restenosis, left main lesion, bypass graft lesion 66.1 (10.7) 79.3 30.9 27.4 4 years 6 – 8 months ISAR-TEST 4 2603 BP SES DP SES DP EES BP SES (n ¼ 1299) DP SES (n ¼ 652) Composite of cardiac death, target vessel MI, clinically indicated TLR at 12 months Symptoms or evidence of ischaemia Cardiogenic shock In-stent restenosis, left main lesion, bypass graft lesion 66.7 (10.9) 76.1 40.7 28.9 4 years 6 – 8 months LEADERS 1707 BP BES DP SES BP BES (n ¼ 857) DP SES (n ¼ 850) Composite of cardiac death, MI, clinically indicated TVR at 9 months
No restriction None None 64.5 (10.7) 74.8 55.2 24.2 4 years 9 months
ACS, acute coronary syndrome; BES, biolimus-eluting stent; BP, biodegradable polymer; DP, durable polymer; EES, everolimus eluting stent; MI, myocardial infarction; PF, polymer-free; SES, sirolimus-eluting stent; TLR, target lesion revascularization; TVR, target vessel revascularization.
G.G.
Stefanini
et
al
are presented as simple, non-stratified Kaplan – Meier curves across all trials and constructed with the use of S-Plus software version 4.5 (In-sightful Corporation, Seattle, WA, USA).
Role of funding source
The sources of funding for this study had no role in the design, data collection, analysis, interpretation of data, writing of the report, or the decision to submit the paper for publication.
Results
A total of 4062 patients were included in the present analysis, of which 2358 patients had been randomly assigned to treatment with biodegradable polymer DES—1501 patients with sirolimus-eluting and 857 patients with biolimus-sirolimus-eluting stents—and 1704 patients to treatment with durable polymer SES.
No heterogeneity across the trials was observed in the analyses of the primary and secondary endpoints. All three included trials were assessed as low risk for bias. Clinical outcomes up to 4
years are summarized in Table2with landmark analyses between
1 and 4 years in Table3.
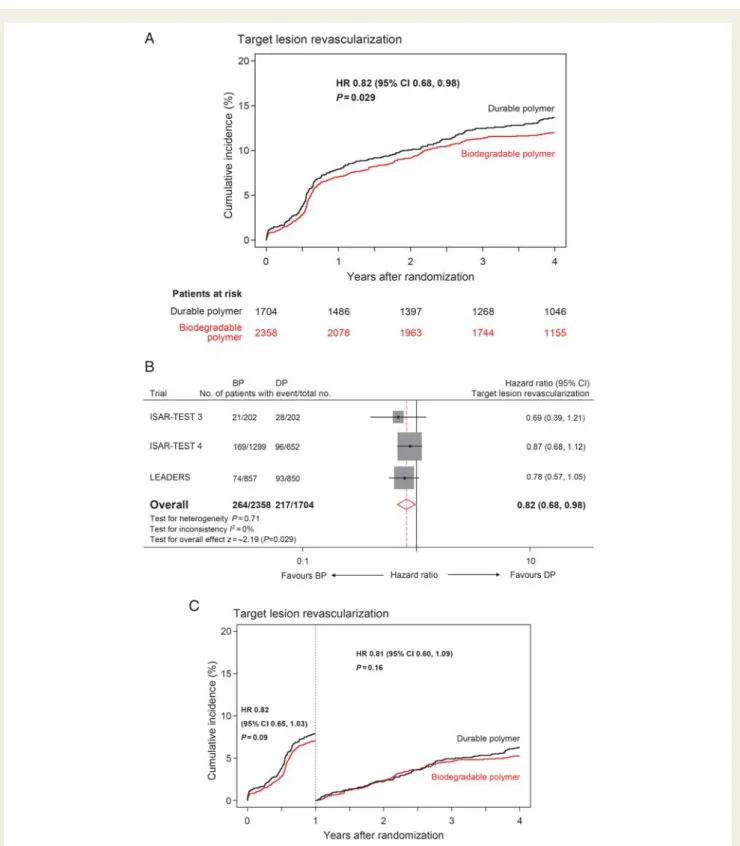
In terms of the efficacy endpoint, the risk of target lesion revas-cularization was significantly lower among patients treated with biodegradable polymer DES vs. durable polymer SES (hazard
ratio 0.82, 95% CI 0.68 – 0.98, P ¼ 0.029) (Figure1).
Regarding safety endpoints, the risk of definite stent thrombosis was significantly reduced with biodegradable polymer DES when compared with durable polymer SES (hazard ratio 0.56, 95% CI
0.35 – 0.90, P ¼ 0.015) (Figure 2). This difference was primarily
driven by a significant risk reduction in terms of very late definite stent thrombosis with biodegradable polymer DES vs. durable polymer SES (hazard ratio 0.22, 95% CI 0.08 – 0.61, P ¼ 0.004)
(Figure2). The risk of definite or probable stent thrombosis was
also lower among patients treated with biodegradable polymer DES (hazard ratio 0.68, 95% CI 0.46 – 1.01, P ¼ 0.054). In landmark analysis between 1 and 4 years, patients treated with biodegradable polymer DES when compared with durable polymer SES had sig-nificantly lower risk of myocardial infarction (hazard ratio 0.59, 95% CI 0.37 – 0.95, P ¼ 0.031).
Discussion
Our findings show that the use of biodegradable polymer DES improves safety and efficacy compared with durable polymer SES during long-term follow-up.
Early generation durable polymer DES have been associated with increased rates of very late (.1 year) stent thrombosis
com-pared with bare metal stents,2,4–6a difference that emerged
par-ticularly among patients with ‘off-label’ indications.24–26 The
pathophysiological mechanisms underlying this adverse event are delayed arterial healing, a process in which the durable polymer coatings used for controlling drug release may have an important
aetiological role.8–12In addition, an excess of late in-stent
resten-osis with durable polymer DES compared with bare metal stents can be detected at angiographic surveillance, and while the clinical impact is likely low, this is interpreted as another expression of
. . . .
. . . . Table 2 Clinical outcomes through 4 years
Biodegradable polymer DES (n 5 2358)
Durable polymer SES (n 5 1704)
Hazard ratio (95% CI) P-value
1 year
Death 93 (4.0) 64 (3.8) 0.97 (0.70 – 1.34) 0.85
Cardiac death 55 (2.4) 47 (2.8) 0.80 (0.54 – 1.19) 0.26 Myocardial infarction 106 (4.5) 67 (4.4) 1.18 (0.86 – 1.61) 0.31 Definite stent thrombosis 26 (1.1) 26 (1.5) 0.80 (0.47 – 1.38) 0.43 Clinically indicated TLR 174 (7.6) 145 (8.8) 0.82 (0.65 – 1.03) 0.09 Cardiac death or myocardial infarction 145 (6.2) 103 (6.1) 1.02 (0.78 – 1.31) 0.91 Cardiac death, myocardial infarction, or
clinically indicated TLR 287 (12.3) 223 (13.3) 0.89 (0.75 – 1.06) 0.20 4 years Death 207 (9.3) 163 (10.0) 0.90 (0.73 – 1.11) 0.32 Cardiac death 113 (5.2) 95 (5.9) 0.87 (0.66 – 1.15) 0.34 Myocardial infarction 135 (6.0) 109 (6.8) 0.96 (0.74 – 1.24) 0.74 Definite stent thrombosis 30 (1.3) 44 (2.8) 0.56 (0.35 – 0.90) 0.015 Clinically indicated TLR 264 (12.0) 217 (13.7) 0.82 (0.68 – 0.98) 0.029 Cardiac death or myocardial infarction 221 (9.9) 187 (11.6) 0.89 (0.73 – 1.09) 0.25 Cardiac death, myocardial infarction, or
clinically indicated TLR
429 (19.0) 350 (21.6) 0.85 (0.74 – 0.98) 0.027
Events are reported as number (percentage from the Kaplan – Meier estimate); hazard ratios and P-values were calculated using random effects meta-analysis. CI, confidence interval; DES, drug-eluting stents; SES, sirolimus-eluting stents; TLR, target lesion revascularization.
impaired vascular healing, with a chronic inflammatory response
provoking a delayed low-grade cellular proliferation.27–29
Biodegradable polymer DES have been developed with the aim of reducing the adverse long-term sequelae related to the persistence of durable polymers in the arterial wall beyond the period necessary to control drug release. Several clinical trials have confirmed the safety and efficacy of biodegradable
polymer DES when compared with durable polymer DES,14–17
although the potential clinical benefit of biodegradable polymer DES is hypothesized to emerge only during the late post-intervention phase, once the polymer coating is completely resorbed.
The findings of the current study may be regarded as novel and important for at least 3 reasons. First, with respect to safety, our findings show for the first time a statistically significant and likely clinically important risk reduction for definite stent thrombosis in favour of biodegradable polymer DES compared with durable polymer-based SES at 4 years (HR 0.56, 95% CI 0.35 – 0.90, P ¼ 0.015). Importantly, this difference was not apparent when the trials included in this study were analysed separately, a
finding mainly attributable to a lack of statistical power.30,31
Indeed, the powering of individual trials to detect differences in rarely occurring adverse safety events such as stent thrombosis has not been adequate in any study to date and was one of the key reasons we undertook the present analysis. Secondly, in a land-mark analysis between 1 and 4 years, we could demonstrate that the incidence of myocardial infarction was significantly lower with biodegradable polymer vs. durable polymer DES (hazard ratio 0.59, 95% CI 0.73 – 0.95, P ¼ 0.031). This risk reduction in late adverse clinical events associated with the use of biodegrad-able polymer DES represents a major benefit, by overcoming the principal limitation of early generation durable polymer DES. Taken together, both of these new findings may be regarded as an important step in the proof-of-concept chain of investigation for biodegradable polymer DES. Thirdly, the enhanced safety profile does not occur at the expense of antirestenotic efficacy.
In actual fact, target lesion revascularization was significantly lower at 4 years in patients treated with biodegradable polymer DES (hazard ratio 0.82, 95% CI 0.68 – 0.98, P ¼ 0.029), a finding not observed in the individual trials and potentially related to the absence of a late catch up phenomenon with biodegradable polymer stents. It may therefore be hypothesized that biodegrad-able polymer-based DES result in improved arterial healing which in turn not only minimizes the risk of stent thrombosis but also improves the long-term durability of the antirestenotic efficacy.
The present study has several limitations. First, this is not a ran-domized clinical trial, but a pooled analysis of individual patient data from three different randomized clinical trials. However, the trials primarily intended to investigate biodegradable polymer DES vs. durable polymer DES consistent with the aim of the present analysis. In addition, we used a statistically conservative meta-analytical model rather than the less robust method of simple data pooling with standard statistical testing. Moreover, our analyses showed no evidence of heterogeneity across the trials and pooled individual patient data revealed no significant dif-ference between the two compared groups at baseline. Secondly, inclusion criteria were not equivalent across the included trials. Nevertheless, the high overall prevalence of acute myocardial in-farction at baseline as well as the relatively complex angiographic characteristics reflects the broadly inclusive nature of the included patient population. Thirdly, only sirolimus-eluting durable polymer DES were included in the present comparison, and therefore the results cannot be extended to other available durable polymer DES. However, durable polymer SES represents the gold standard among early generation DES, and performance differences with newer generation durable polymer DES—such as everolimus-eluting and zotarolimus-everolimus-eluting stents—vs. SES is still a matter of
some debate.32 Finally, two different biodegradable polymer
stents were included in the analysis, and although the coatings of both stents contain polylactic acid monomers and limus-agent drugs, differences in polymer degradation and drug release kinetics between the two stents may be expected.
. . . . Table 3 Clinical outcomes in landmark analysis (1 – 4 years)
Biodegradable polymer DES (n 5 2358) Durable polymer SES (n 5 1704) HR (95% CI) P-value 1 – 4 years Death 114 (5.6) 99 (6.5) 0.85 (0.65 – 1.12) 0.26 Cardiac death 58 (2.9) 48 (3.2) 0.95 (0.64 – 1.40) 0.79 Myocardial infarction 29 (1.5) 42 (3.0) 0.59 (0.37 – 0.95) 0.031 Definite stent thrombosis 4 (0.2) 18 (1.3) 0.22 (0.08 – 0.61) 0.004 Clinically indicated TLR 102 (5.2) 86 (6.3) 0.81 (0.60 – 1.09) 0.16 Cardiac death or myocardial infarction 76 (3.9) 84 (5.9) 0.73 (0.53 – 1.00) 0.050 Cardiac death, myocardial infarction, or clinically indicated
TLR
154 (8.2) 140 (10.4) 0.79 (0.63 – 1.00) 0.048
Events are reported as number (percentage from Kaplan – Meier estimate); hazard ratios and P-values were calculated using random effects meta-analysis. CI, confidence interval; DES, drug-eluting stents; SES, sirolimus-eluting stents; TLR, target lesion revascularization.
Figure 1 Efficacy endpoint: target lesion revascularization. (A) Kaplan – Meier curves for the pooled population in each of the stent groups. (B) Forest plot with hazard ratios with biodegradable polymer stents vs. permanent polymer stents for individual trials and the pooled popu-lation. Hazard ratios are shown on a logarithmic scale. The size of the square is proportional to the weight of the individual studies, measured as the inverse of the estimated variance of the log hazard ratio. BP, biodegradable polymer drug-eluting stent; DP, durable polymer sirolimus-eluting stent. (C ) Kaplan – Meier curves for the pooled population in each of the stent groups with the landmark analysis at 1 year.
Figure 2 Safety endpoint: definite stent thrombosis. (A) Kaplan – Meier curves for the pooled population in each of the stent groups. (B) Forest plot with hazard ratios for biodegradable polymer stents vs. permanent polymer stents for individual trials and the pooled population. Hazard ratios are shown on a logarithmic scale. The size of the square is proportional to the weight of the individual studies, measured as the inverse of the estimated variance of the log hazard ratio. BP, biodegradable polymer drug-eluting stent; DP, durable polymer sirolimus-eluting stent. (C ) Kaplan – Meier curves for the pooled population in each of the stent groups with the landmark analysis at 1 year.
Conclusions
Biodegradable polymer DES improve safety and efficacy compared with durable polymer SES during long-term follow-up to 4 years.
Acknowledgements
S.W. and A.K. had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Funding
The ISAR-TEST 3 and ISAR-TEST 4 trials were industry independent; funding was provided in part by the Bavarian Research Foundation (BFS-ISAR Aktenzeichen AZ: 504/02 and BFS-DES Aktenzeichen AZ: 668/05). The LEADERS trial was funded by Biosensors Europe SA, Switzerland. Funding for the current analysis was provided in part by the Swiss National Science Foundation (Grant 33CM30-124112). G.G.S. is recipient of a research grant from the European Association of Percutaneous Cardiovascular Interventions of the European Society of Cardiology. No other sources of funding were used for the current analysis.
Conflict of interest: B.M. has received educational and research support to the institution from Abbott, Cordis, Boston Scientific, and Medtronic; A.S. and A.K. hold a patent related to the stent coating used on the biodegradable polymer DES studied in the ISAR-TEST 3 and ISAR-TEST 4 trials, A.K. reports having received lecture fees from Abbott, Biotronik, Cordis and Medtronic; S.W. has received research contracts to the institution from Abbott, Boston Scientific, Biosensors, Cordis, and Medtronic. The other authors report no conflicts.
References
1. Stettler C, Wandel S, Allemann S, Kastrati A, Morice MC, Schomig A, Pfisterer ME, Stone GW, Leon MB, de Lezo JS, Goy JJ, Park SJ, Sabate M, Suttorp MJ, Kelbaek H, Spaulding C, Menichelli M, Vermeersch P, Dirksen MT, Cervinka P, Petronio AS, Nordmann AJ, Diem P, Meier B, Zwahlen M, Reichenbach S, Trelle S, Windecker S, Juni P. Outcomes associated with drug-eluting and bare-metal stents: a collaborative network meta-analysis. Lancet 2007;370:937 – 948. 2. Kastrati A, Mehilli J, Pache J, Kaiser C, Valgimigli M, Kelbaek H, Menichelli M,
Sabate M, Suttorp MJ, Baumgart D, Seyfarth M, Pfisterer ME, Schomig A. Analysis of 14 trials comparing sirolimus-eluting stents with bare-metal stents. N Engl J Med 2007;356:1030 – 1039.
3. Byrne RA, Sarafoff N, Kastrati A, Schomig A. Drug-eluting stents in percutaneous coronary intervention: a benefit-risk assessment. Drug Saf 2009; 32:749 – 770.
4. Wenaweser P, Daemen J, Zwahlen M, van Domburg R, Juni P, Vaina S, Hellige G, Tsuchida K, Morger C, Boersma E, Kukreja N, Meier B, Serruys PW, Windecker S. Incidence and correlates of drug-eluting stent thrombosis in routine clinical prac-tice. 4-year results from a large 2-institutional cohort study. J Am Coll Cardiol 2008; 52:1134 – 1140.
5. Spaulding C, Daemen J, Boersma E, Cutlip DE, Serruys PW. A pooled analysis of data comparing sirolimus-eluting stents with bare-metal stents. N Engl J Med 2007; 356:989 – 997.
6. Stone GW, Moses JW, Ellis SG, Schofer J, Dawkins KD, Morice MC, Colombo A, Schampaert E, Grube E, Kirtane AJ, Cutlip DE, Fahy M, Pocock SJ, Mehran R, Leon MB. Safety and efficacy of sirolimus- and paclitaxel-eluting coronary stents. N Engl J Med 2007;356:998 – 1008.
7. Nakazawa G, Finn AV, Joner M, Ladich E, Kutys R, Mont EK, Gold HK, Burke AP, Kolodgie FD, Virmani R. Delayed arterial healing and increased late stent throm-bosis at culprit sites after drug-eluting stent placement for acute myocardial in-farction patients: an autopsy study. Circulation 2008;118:1138 – 1145.
8. Finn AV, Nakazawa G, Joner M, Kolodgie FD, Mont EK, Gold HK, Virmani R. Vas-cular responses to drug eluting stents: importance of delayed healing. Arterioscler Thromb Vasc Biol 2007;27:1500 – 1510.
9. Cook S, Ladich E, Nakazawa G, Eshtehardi P, Neidhart M, Vogel R, Togni M, Wenaweser P, Billinger M, Seiler C, Gay S, Meier B, Pichler WJ, Juni P, Virmani R, Windecker S, Cook S, Ladich E, Nakazawa G, Eshtehardi P,
Neidhart M, Vogel R, Togni M, Wenaweser P, Billinger M, Seiler C, Gay S, Meier B, Pichler WJ, Juni P, Virmani R, Windecker S. Correlation of intravascular ultrasound findings with histopathological analysis of thrombus aspirates in patients with very late drug-eluting stent thrombosis. Circulation 2009;120: 391 – 399.
10. Joner M, Finn AV, Farb A, Mont EK, Kolodgie FD, Ladich E, Kutys R, Skorija K, Gold HK, Virmani R. Pathology of drug-eluting stents in humans: delayed healing and late thrombotic risk. J Am Coll Cardiol 2006;48:193 – 202.
11. Wilson GJ, Nakazawa G, Schwartz RS, Huibregtse B, Poff B, Herbst TJ, Baim DS, Virmani R. Comparison of inflammatory response after implantation of sirolimus-and paclitaxel-eluting stents in porcine coronary arteries. Circulation 2009;120: 141 – 149, 1 – 2.
12. Byrne RA, Joner M, Kastrati A. Polymer coatings and delayed arterial healing fol-lowing drug-eluting stent implantation. Minerva Cardioangiol 2009;57:567 – 584. 13. Virmani R, Guagliumi G, Farb A, Musumeci G, Grieco N, Motta T, Mihalcsik L,
Tespili M, Valsecchi O, Kolodgie FD. Localized hypersensitivity and late coronary thrombosis secondary to a sirolimus-eluting stent: should we be cautious? Circu-lation 2004;109:701 – 705.
14. Mehilli J, Byrne RA, Wieczorek A, Iijima R, Schulz S, Bruskina O, Pache J, Wessely R, Schomig A, Kastrati A. Randomized trial of three rapamycin-eluting stents with different coating strategies for the reduction of coronary restenosis. Eur Heart J 2008;29:1975 – 1982.
15. Byrne RA, Kastrati A, Kufner S, Massberg S, Birkmeier KA, Laugwitz KL, Schulz S, Pache J, Fusaro M, Seyfarth M, Schomig A, Mehilli J. Randomized, non-inferiority trial of three limus agent-eluting stents with different polymer coatings: the Intra-coronary Stenting and Angiographic Results: Test Efficacy of 3 Limus-Eluting Stents (ISAR-TEST-4) Trial. Eur Heart J 2009;30:2441 – 2449.
16. Windecker S, Serruys PW, Wandel S, Buszman P, Trznadel S, Linke A, Lenk K, Ischinger T, Klauss V, Eberli F, Corti R, Wijns W, Morice MC, di Mario C, Davies S, van Geuns RJ, Eerdmans P, van Es GA, Meier B, Juni P. Biolimus-eluting stent with biodegradable polymer versus sirolimus-eluting stent with durable polymer for coronary revascularisation (LEADERS): a randomised non-inferiority trial. Lancet 2008;372:1163 – 1173.
17. Chevalier B, Silber S, Park SJ, Garcia E, Schuler G, Suryapranata H, Koolen J, Hauptmann KE, Wijns W, Morice MC, Carrie D, van Es GA, Nagai H, Detiege D, Paunovic D, Serruys PW. Randomized comparison of the Nobori Bio-limus A9-eluting coronary stent with the Taxus Liberte paclitaxel-eluting coron-ary stent in patients with stenosis in native coroncoron-ary arteries: the NOBORI 1 trial—Phase 2. Circ Cardiovasc Interv 2009;2:188 – 195.
18. Barlis P, Regar E, Serruys PW, Dimopoulos K, van der Giessen WJ, van Geuns RJ, Ferrante G, Wandel S, Windecker S, van Es GA, Eerdmans P, Juni P, di Mario C. An optical coherence tomography study of a biodegradable vs. durable polymer-coated limus-eluting stent: a LEADERS trial sub-study. Eur Heart J 2010;31: 165 – 176.
19. Cutlip DE, Windecker S, Mehran R, Boam A, Cohen DJ, van Es GA, Steg PG, Morel MA, Mauri L, Vranckx P, McFadden E, Lansky A, Hamon M, Krucoff MW, Serruys PW. Clinical end points in coronary stent trials: a case for standardized definitions. Circulation 2007;115:2344 – 2351.
20. Higgins J, Green S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.0.0 edn. The Cochrane Collaboration; 2008.
21. Sterne JAC, Bradburn MJ, Egger M. Meta-analysis in StataTM. In: Systematic Reviews
in Health Care. London: Blackwell BMJ Books; 2001.
22. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ 2003;327:557 – 560.
23. DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials 1986;7: 177 – 188.
24. Win HK, Caldera AE, Maresh K, Lopez J, Rihal CS, Parikh MA, Granada JF, Marulkar S, Nassif D, Cohen DJ, Kleiman NS. Clinical outcomes and stent thrombosis following off-label use of drug-eluting stents. JAMA 2007;297: 2001 – 2009.
25. Beohar N, Davidson CJ, Kip KE, Goodreau L, Vlachos HA, Meyers SN, Benzuly KH, Flaherty JD, Ricciardi MJ, Bennett CL, Williams DO. Outcomes and complications associated with off-label and untested use of drug-eluting stents. JAMA 2007;297:1992 – 2000.
26. Marroquin OC, Selzer F, Mulukutla SR, Williams DO, Vlachos HA, Wilensky RL, Tanguay JF, Holper EM, Abbott JD, Lee JS, Smith C, Anderson WD, Kelsey SF, Kip KE. A comparison of bare-metal and drug-eluting stents for off-label indica-tions. N Engl J Med 2008;358:342 – 352.
27. Byrne RA, Iijima R, Mehilli J, Pinieck S, Bruskina O, Schomig A, Kastrati A. Durabil-ity of antirestenotic efficacy in drug-eluting stents with and without permanent polymer. JACC Cardiovasc Interv 2009;2:291 – 299.
28. Finn AV, Nakazawa G, Kolodgie FD, Virmani R. Temporal course of neointimal formation after drug-eluting stent placement: is our understanding of restenosis changing? JACC Cardiovasc Interv 2009;2:300 – 302.
29. Raber L, Wohlwend L, Wigger M, Togni M, Wandel S, Wenaweser P, Cook S, Moschovitis A, Vogel R, Kalesan B, Seiler C, Eberli F, Luscher TF, Meier B, Juni P, Windecker S. Five-year clinical and angiographic outcomes of a randomized comparison of sirolimus-eluting and paclitaxel-eluting stents: results of the Sirolimus-Eluting Versus Paclitaxel-Eluting Stents for Coronary Revascularization LATE Trial. Circulation 2011;123:2819 – 2828.
30. Byrne RA, Kastrati A, Massberg S, Wieczorek A, Laugwitz KL, Hadamitzky M, Schulz S, Pache J, Fusaro M, Hausleiter J, Schomig A, Mehilli J. Biodegradable polymer versus permanent polymer drug-eluting stents and everolimus- versus sirolimus-eluting stents in patients with coronary artery disease: 3-year outcomes from a randomized clinical trial. J Am Coll Cardiol 2011;58:1325 – 1331.
31. Stefanini GG, Kalesan B, Serruys PW, Heg D, Buszman P, Linke A, Ischinger T, Klauss V, Eberli F, Wijns W, Morice MC, Di Mario C, Corti R, Antoni D, Sohn HY, Eerdmans P, van Es GA, Meier B, Windecker S, Juni P. Long-term clinical outcomes of biodegradable polymer biolimus-eluting stents versus durable polymer sirolimus-eluting stents in patients with coronary artery disease (LEADERS): 4 year follow-up of a randomised non-inferiority trial. Lancet 2011; 37:1940 – 1948.
32. de Waha A, Dibra A, Byrne RA, Ndrepepa G, Mehilli J, Fusaro M, Laugwitz KL, Massberg S, Schomig A, Kastrati A. Everolimus-eluting versus sirolimus-eluting stents: a meta-analysis of randomized trials. Circ Cardiovasc Interv 2011;4: 371 – 377.
INTERACTIVE CARDIOVASCULAR FLASHLIGHT
. . . .
doi:10.1093/eurheartj/ehr496
Online publish-ahead-of-print 12 January 2012
A patient with angina at night: core curriculum chapters 3 (non-invasive
imaging) and 9 (chronic ischaemic heart disease)
Frank A. Flachskampf1* and Roger Hall2
1
Institutionen fo¨r medicinska vetenskaper, Uppsala Universitet, Uppsala, Sweden and2
University of East Anglia, Norfolk, UK
*Corresponding author. Tel:+46 18 611 4404, Fax: +46 18 50 92 97, Email:[email protected]
This diabetic 66-year-old male patient had episodes of nightly angina, but then was symptom free and could be exercised without symptoms. His ECG at rest (Figure) showed T-wave inversion in II, III, avF, and V5 and V6. How should this patient be worked up? Should he have non-invasive testing, and if so, which kind? If coronary artery disease amen-able to revascularization was found, is there an indication to perform it? Follow us step-by-step through this typical scenario. Explore the full
case on the ESC’s case-based learning website at www.escardio.org/
education/eLearning/clinical-cases.