Sperm counts in enzymatically liquefied cervical mucus: quantitative validation using donor cervical mucus
7
0
0
Texte intégral
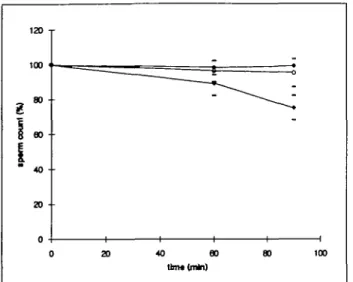
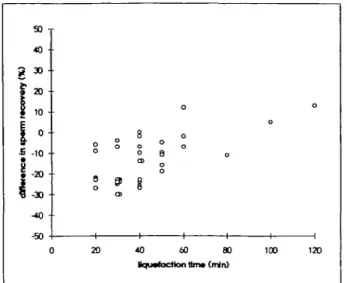
Figure


Documents relatifs
