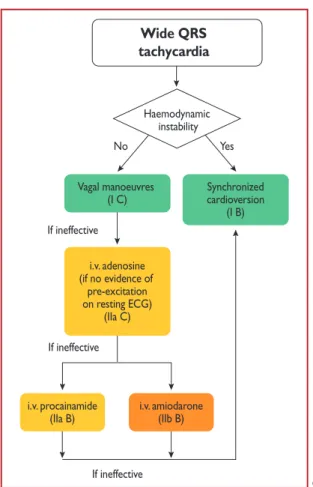
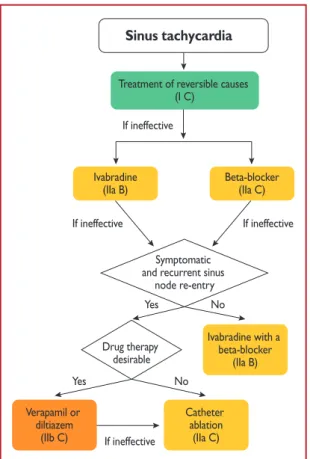
2019 ESC Guidelines for themanagement of patients with supraventricular tachycardia
Texte intégral
Figure




Documents relatifs
And finally, the easy identification allows more flexibility in the mode of TALEN introduction into Drosophila embryos, and we showed that TALEN plasmid microinjection is a
J’espère de tout mon cœur que l’un n’ira pas sans l’autre, autant pour le bien de l’humanité que pour celui de notre bien malade planète et de tous ces mondes que nous
Il di ri ge et il sur vei lle la cons truc tion.. Le char pen tier fa bri q ue la char
The main goal of this paper is to propose a non-Newtonian exten- sion to the standard LB model that incorporates correct blood rheology in case of small shear stress.. In Section 3,
Tracer La courbe des fréquences cumulées croissantes (courbe de répartition) et déterminer graphiquement une valeur approchée de la médiane de la série... 4. On souhaite
Dans une approche privi- légiant la composition en diptyque, le rapport se stabilise, pour ne pas dire s’inverse, car, en l’occurrence, c’est tout le roman Madame Bâ qui prend en
Une mise en œuvre rapide des traitements étant primordiale lors de neutropénie fébrile, de syn- drome de lyse tumorale et pour certains patients at- teints de diarrhée et
