J:
-What is new in MGUS and smoldering
multiple myeloma
M. Vercruyssen'. L Vrancken2,
J
.
Caers2SUMMARY
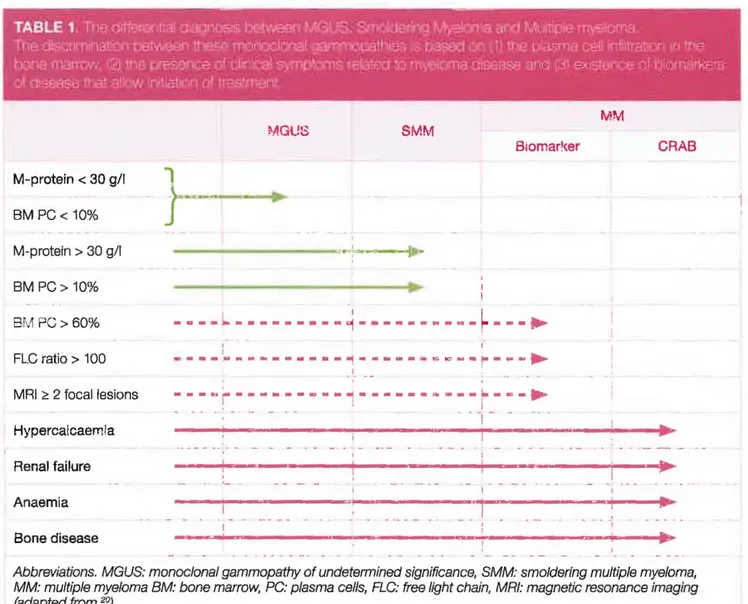
Multiple Myeloma (MM) and other plasma cell malignancies initially present as an asymptomatic precursor state, known as monoclonal gammopathy of undetermlned signiflcance (MG US). When confronted to a mono-clonal proteln in blood or urine tests, physicians should first exclude the presence of a treatment-requiring MM. They should be aware that there are two benign precursor states, that do not require anti-myeloma trealmen!. Both MGUS and Smoldering Multiple Myeloma (SMM) need an initial visit by a haematologist, with further follow-up tailored to the individual patient and disease characteristics. In the current article we describe both entitles, discuss their monitoring and resume the latest publications in their field.
INTRODUCTION
In 2014, the International Myeloma Working Group (lMWG) updated the diagnostic criteria for Monoclonal Gammopathy
ofUndetermined Significance (MGUS), Smoldering Multiple
Myeloma (SMM) and multiple myeloma (MM)' The
dis-tinction between the different disease stages is based on
biological parameters and tbe presence of clinical symptoms or early signs of emerging myeloma disease
(Table
1). MGUS is defined by a serum M-protein 1evel of <3 gldL, a bone marrow plasma ceil (EMPC) infiltration of <10%, and the absence of clinical complications. SMM is defined by serumM-protein (lgG or IgA) levcls of ,,3 gldL and/or clonai BMPCs
of 10%-60% in the absence of a myeloma defining event (MDE) or amyloidosis.' The updated IMWG diagnostic
cri-teria for MM include the presence of M-protein in blood or
urine, a BMPC infiltration of
>
10%, or biopsy-proven bony or extrameduUary plasmacytoma as weU as a MDE. A MDE is defined by CRAB criteria fhypercalcemia, radiological bone lesions. anaemia, and renal faiture) or one or more ofthe foUowing biomarkers of malignancy: a clonai BMPC percentage of >60%, involved/uninvolved serum free light chain (sFLC) ratio of >100 or >1, and focallesions (FLs) detected by magnetic resonance imaging (MRD.
MONOCLONAL GAMMOPATHY OF
UNDETERMINED SIGNIFICANCE
The incidence of MGUS is estimated at 3.4% in the general population over 50 years of age. This incidence increases with age from only 1. 7% in patients aged 50-59 years to 6.6% beyond 80 years.' Several hereditary, genetic as weU as environmental factors play a role in the development of MGUS, including age, race, gender, familial history and
obe-siey. A recent French study demonstrated that the M-protein isolated from MGUS and MM patients, reacted in 57 (23.4%) of 244 patients studied with Iysates or proteins from infectious pathogens. Of these, EBV nuelear antigen-I (EBNA-l) was the most frequent target.' These results indicate that
antigen-driven stimulation of plasma cells could be an early patho-genic mechanism that initiates monoclonal gammopathies.
RISK OF PROGRESSION OF MGUS
The average risk of evolution from MGUS to MM, amyloidosis
or other lymphoproliferative disease is 1% per year, depen-ding on the nature of the protein implicated (lgG or non-IgG), the monoclonal protein leve! (> 15g!l) and theFLC ratio (abnormal Ot nor).
5.'
Using these three items, the Maya Clinic developed a simple score that aUows to stratify patients'Se",ce d'Hématologie. Inst~ut Jules Bordet: 'Service d'hématologie. CHU de Liège.
Aease send ail correspondence 10: Dr. Jo Gaers. MD, AlD; Departmef1t of ClinK:aJ HiematoklQv, Centre Hospital ... Universliare de Uège. Dom Un" Sart lilman -B 35, B-4OOO Liège, Tel: +32 (0)43667704, Secr: +32 (0)4 3667201, Eman: [email protected]
CDnfllet Dt Intarest: The authors have noth~ to cfooose and Indicate no potential confllct of i-..st.
TABLE 1 ~ ii1t~.<lIff8mr,I:af
cfillQl1C$S
b:!lWeenMGU$.
SmoIdeMg
~'6 a<l(lMuilicie
my:;1om8.1he discnmnaoon
0Bl1NE! .... U~ mcr'lOCh~ ~,pélhoes .0QaSe(I
an \ 1I11Je
IJlasma œn
InllllfBOCr! ", !nebone
m·lITO ...12)1r19
rr..sonce
cldir11ca1
S}'!11P'.ctnS letEr~X1 :0 m,~diooase and
(3)exiSf(lr<;e cf t!i'.1<rIarkes
al
(l1:l8ilSB Ina:ai'ON
ln'tialUl ,~ lroot.menlMM
MGt!B SMM 8jomar~er CRAS M-protein < 30 g/I}--~.
BM PC< 10% M-protein > 30 g/I ---~-~-_...
BMPC> 10% BM PC> 60% _·_-~_·_---1-_____
M_~_~__
.~,
,
FLC ratio> 100-
---~---
,
-
---~---
-
~
~
~-r---·
.-1, __ MRI ~ 2 focallesions___
~~_________
,
______
~___
~_R_~ ~ . 1 - _. - .- - . - . -1 - - _. Hypercalcaemia Renal failure Anaemia-..
-',
Bone disease 1Abbreviations. MGUS: monoclonal gammopathy of undetennined significance, SMM: smolderlng multiple myeloma,
MM: multiple myeloma BM: bone marrow. PC: plasma cel/s, FLC: free light chain, MRI: magnetic resonance imaging (adapted from 20)
according to their r"k status: eg 5% of the patients that do not show any risk factors progress at 20 years. This percen-[age increases to 58%
if
three factors are present.6 Of note,if
the FLC ratio is very abnormal«
0.125 or> 8),
the risk of progression is even higher, reaching 60.5% at 20 years.'Another significam risk factor of progression is a decreased serum level of both uninvoh-ed immunoglobulins (Hazard Ratio of 2) while a decrease in just one of them does not impact this risk.' Recently, two different teams showed that also the presence of translocation (4;14) and deletion 17p
in the bane marrow clonaI plasma ceUs is associated with
a higher risk of progression.6,9 As such, when feasible, cyto-genetics may allow the identification of a high-risk patier" group for whom a c10ser follow up might be beneficial.
MONITORING OF MGUS PATIENTS
While MGUS is relatively frequent, in the absence of symp-toms the work-up rarely leads to a the diagnosis of an O\'ert disease. Moreover, ir is nO[ certain chat close follow-up, and an early diagnosis of MM, leads to a better prognosis, since
VOLU
IV!
E9cECEMBER2018more than one third of the MGUS cases evolve to SMM and do not require any treatmemYi Furthennore, the \'ast majority of the MGUS patients will die from other diseases, As such, after the identification of the risk group and ex-clusion of any evolution after three months, one could refer
the patient ta his genera! practitioner for a follow-up every
2
0:-3
ye~!::cr
z.:l
rtu
&
ll
:\-
i:: G.sec
f
Q!1e. Qi:"m
ore risk
fa~tor5. Moreoyer, if life expectancy is less than5
years and/or thepatient is older than 85 years, the follow-up can be omitted." If a progression is suspected, of course, the patient should be referred ta the haematologist for [urther investigations.
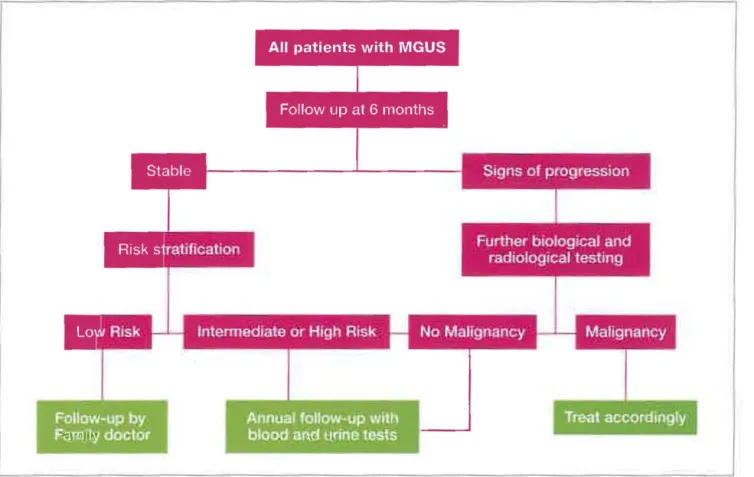
Ta identify progression to myeloma or Iymphoma, biological and radiological tests are generally required to identify a
disease progression. However a careful clinicat examinarion is needed to exc\ude complication of the monoclonal protein itself. Once the work-up has established the absence of these pathologies and the early follow-up did not show a
rapid evolution of the paraprotein, the patient can be refer-red ta his general practitioner ta assure the right follow-up (Figure 1).
•
•
~
TIP
-Follow-up
by
F'!HolTIi/ doctor
Annual follow-up w.th
blood an.d u.rine lests
Treal
accordingly
FIGURE 1. Aigorithm for fo"ow·up of patients wlth monoclonal gammopathy of undeterrnined significance (MGUS).
MONOCLONAL GAMMOPATHY OF CLiNICAL SIGNIFICANCE: A NOVEL CONCEPT
Signs or symprams of a peripheral neuropathy must be inves-tigated ra exclude paraneoplastie syndrome, in particular if IgM is the paraprotein implicated since the prevalence of symptoms can reach 31% versus only 6% in case of IgG sub-type." Fifty percent of them are due ta ami-MAG (myelin-associated glycoprotein) activity of the M componem and anotber 35% is related to anti-ganglioside aetivity. Amyloi-dosis or POEMS syndrome (Polyneuropathy, Organomegaly, Endocrinopathy, Monoclonal protein and Skin change) must also be evoeated, especiaIly in case of lambda secretionlZ
In case of a creatinine increase, myeloma or progression to
myeloma must he excluded, but other, sometimes discrete but always severe troubles can emerge. This includes nephro-tic syndrome in amyloidosis or in other light or heavy chain depasits (RandaIl type). Fanconi disease, caused by light chain deposits in the renal tubules, must a150 be recognised in case of Ionie and metabolic abnormalictes. Other para
-neo-plastic immune glomerulonephritis can aIso be obser-ved. AIl these emities are known as MGRS (Monoclonal Gammopathy of Renal Sigrtificanee) as the abnormalities can he proved ta be related to the monoclonal pattern. A treatment could he envisaged. 50, in from of an unexplained
renal impairment, lurther investigations must be perfromed and a kidney biopsy deserves serious discussionIJ
Sorne dermatologie entities are also described. The Schnit-zler syndrome which manifests with fever, unicarial rash and arthropathy (sometimes wlth organomegaly) is eaused by a monoclonal IgM paraprotein, especially kappa. Other
skin diseases can be encoumered, such as necrobiotic xan-thogranuloma or other skin changes, in particular in the POEMS syndrome.
FinaIly, sorne haemorrhagic status can be observed in case of paraneoplastic deficiency of von Willebrand factor or fac-tor X in amyloidosis.
SMOLDERING MULTIPLE MYELOMA
In contrast ra MGUS, SMM has a higher risk of progression ra symptomatic MM. However, bath diseases are considered as precursor disease stages and, by definition, both disor-ders are asympramatic. The 2014 IMWG criteria, changed the group of ultra-high risk SMM (which was associated with an 80% risk of progression to MM) into the group treatment-requiring MM' This change aIlows physicians ta initiate an early therapeutic stTategy, that could avoid serious complications .nd where the potenti.1 benefit justifies the risks of taxicity.TABLE 2, Pl1lgrxoSlc f~s
cl f.gH:s!<
SMM (Ptl'11a! flS1)1
Serum M-protein ;,30g/Ll
,
~9A~MM_
1,
-
--1
-Progressive increase in M-protein levai (evoMng type 1
of SMM; increase in serum M-protein by ;,25% on 2 successive evaluations within a 6-month period)
- Immunoparesis with reduetion of 2 uninvolved immuno-globulin isotypes
Ab~orma! PC immunopher.otype r.::2:95~é cf 8MPCs are clona!)
t(4:14) O( del(17PJ or 1q gain
Inereased cireulating PCs
M RI with diffuse abnormalities or 1 focal lesion DEi \'vit.~ nypermetabo!ic focal (esicns, but vv'ltnoul
underlying cone Iylie iasions
RISK OF PROGRESSION OF SMM
The risk of progression of SMM was originally established by
Kyle et al.
based on a cohoIt of 236 patients with smolderingmycloma disease, defined by the old IMWG criteria." The
esrimaœd risk of progression ta MM or amyloidosis was
10% per year for the fiISt 5 yeaIS, then the progression rates
decreased progressively, but after 20 years 72% of the patients
progressed. The recent IMWG criteria consider ultra-high
risk SMM as treatment-requiring MM. As such, this group of patients is no longer considered as SMM patients, which probably affects the initial progression risks that were des-cribed by
Kyle et al.
Prospective studies are needed tO reassessthis risk when the 2014 IMWG criteria are applied.
ln the past decades, other prognostic factors that identified
patients with a high risk of progression have been described. These risk factors are summarized in
Table
2. PatientS th8.tdo not present any of these risk factors can be considered as
low-risk patien:s, -.vith ar: estimated risk of progression of 5 to 10% per year. Sorne of these factors are based on routine
tests, while others require complememary examinations.
Routinely performed radiologieal and laboratory testS
(im-munoglobulin isotype, serum M-protein levels, sFLC levels,
immunoglobulin quantification) can help to estimate this
progression tisk in daUy practice. The use of cytogenetic
evaluation is justified for young patients, but there is insuffi-cient data to justify the systematic reahzation of a PET-CT
for ev",y patient with SMM.
VOLUIVl
E9DBCE
,BER2018Researchers at the Mayo Clinic :-e-examined their cohort of patients with SMM who met the 2014- jMWG criteria to
define their natural history and idemified sC\'eral risk factors for progression." They finally proposed a simple scoring
syscem, that can be retained as the "3 X 20" score. A bone
marrow plasmaeytosis superior to 20%, M-protein levels
above 20 glL, and a sFLC ratio abm'e 20 at diagnosis can be
usee! ta risk st!"atify patie:i.ts with SMM u5ing t::'e cur:eŒ: IMWG criteria. The estimated median time to progression
~n the low-risk, intermediace-risk, and high-risk groups were
109.8 months, 67.8 months and 29.2 months, respecti\'eiy.
MONITORING OF SMM PATIENTS
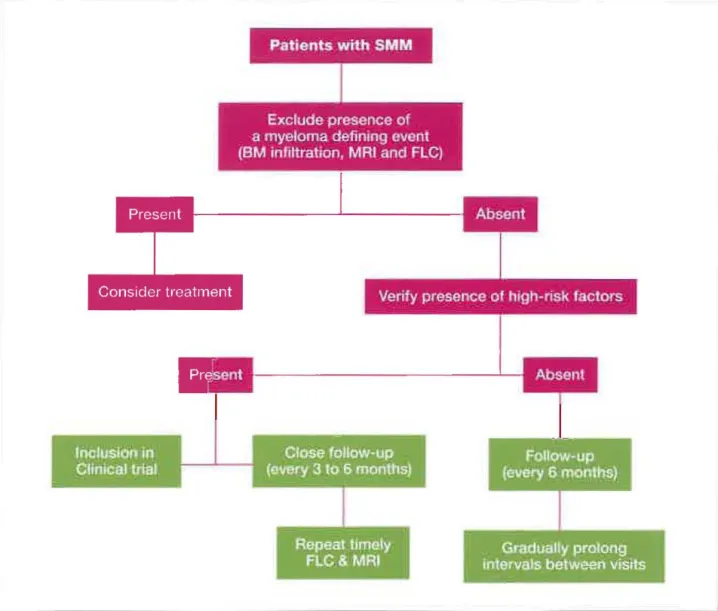
Similar ta MGUS patients, the monitoring of SMM is based
on clinical (paying attention to signs of a possible MM) and
biological (blood coums, calcemia, serum creatinine, prorein
electrophoresis, proteinuriaJ follow-up (Figure 2)." High-risk patients need to be [ollowed-up closely (every 3 months) to
allow the early derection of an evolution towards symptomatic
MM and [Q avoid devastating complications such as acute
renai failure, vertebral fractures, spinal cord compression,
etc. For these patients, sFLC assays and MRIs can be
repea-ced during the follow-up, although there is no standardised
recommendation on the frequency and intervals of these tests.
For low-risk SMM patients, the monitoring can be delayed
(every 6 months) and complementary studies such as sFLC
and MRI should be repeated in case of signs of progression.
We believe that prospective studies are needed to define the
best monitoring strategies for both S[~I~1 patient gTOL:pS.
EARLY TREATMENT OF HIGH-RISK SMM?
After the land mark publication of Mateos
et
al.
, other clinical
trials evaluating early treatment strategies for high-tisk SMM
have been presentedY These trials eirher aim ar curing patients with aggressive ueatments or to control and delay
progression with a prolonged treatment. Preliminary results from 2 studies were presented at ASH 2017.
Mateos
etal.
presented the preliminary results of the GEM-CESARstudy,
a phase Il single-arm trial including 90 patients with a
high-tisk SMM (defined according to the prognostic scores
of the Mayo Clinic and/or of the Spanish Myeloma Group)."
The treatment in this trial eonsisted of earfilzomib,
lenalido-mide and dexamethasone (KRd) as induction, followed By
HDT-ASCT and consolidation with Krd and Rd maintenance.
lt has to be acknowledged tbat 30 patients (33%) presemed
at least one of the new MM diagnostic criteria of 2014. The
primary endpoint was the aehievement of minimal residual
disease (MRD) negativity (evaluated by f10w cytometry). At
the time of the analysis, most patients (N=71) completed the
Patients
with
SMMExclude presence of
a myeloma defining avent
(BM infiltration
,
MAI
and
FLC)
Inclusion in
Clinlcal trial
Verity
presence of high
-
rlsk factors
FIGURE 2. Aigarijhms for patients with smoldering muHiple myelama (SMM).
received consolidation, and 29 were in the maintenance
phase. After a median fallow-up of 10 month, 69 patients
(98%) responded ta treatment after the completion of
induc-tion therapy, about half of wham had a complete response
(CR) or stringent CR (sCR). Two patients obtained a CR but
relapsed before the end of induction. MRD negativity and depth of response ta treatment increased as patients
pro-gressed through therapy. After the consolidation phase,
60% of the patients achieved MRD negativity, indicating
that deep re.sponses can be obtained wÎth an intensive
treat-ment of SMM.'6 Of course, longer follow-up data are needed
ta assess if this strategy will ultimately cure patients.
HoJmeister
et al. presented the preliminary results of theCENTAURUS trial, a randomized phase II study evaluaring
3 dararumumab dose schedules in 123 SMM patients." There
were 3 treatment strategies, all including cycles of 8 weeks
of treatment: (1) a short regimen consisting of 1 cycle of
daratumumab weekly; (2) an intermediate schedule staring
with weekly daratumumab in cycle 1 and every 8 weeks up
ta cycle 20 and (3) a long regimen (weekly daratumumab in
cycle l, every other week in cycles 2 and 3, every 4 weeks in
cycles 4 through 7, and every 8 weeks up ta cycle 20). The
two main endpoints were CR rate and progression-free s
ur-vival (PFS). The 12-month PFS rates were 95% with the long
schedule, 88% with the intermediate dosing schedule, and
81% with the short, intense schedule. More than haU (54%)
of the patients in the long arm and 49% in the intermediate
arrn had a partial response (PR) or better. ln the short arm,
38% of patients achieved a PR or better. The CR rate was Iess
than 15% in each arm. These results show that daratumumab
in monotherapy may induce a haematalogical response and
delays the progression of high-risk SMM. However, it also
suggests that the treatment should be extended as shawn
by the poor results in the short ann. lt is unlikely that
tumurnab single-agent will cure high-risk SMM, but il.: may 6, Rajkumar, S. '/. et al. Serum lree ),ç,ht Ch<;;n ratio is an naepend!m; 1s{fecto
-fo-delay the progression of the disease. The long dosing sche- ,:>r::g'6ssion in monockmal gammopathy of undetermined signlficence B!oQC
dule is currentlyunder investigation in the ongoingphase III 2OG5.1CS,9-:2-ê17
AQUlLA study. "7 K;.'Ie, A. A. el al.LDng-Term Folb.· .. -Up of ~-tonoclonal Gamrnopatt:~' 0: ,j:-c s:er-Bath these approaches (intensive vs. extended treatffienù are fTllnec S ;'l'~œ.,œ ,\, ~gl J Med 2018:378, 241-24d.
inreresting, but they also have their limitations. Additionally, 8. LekshTlan, A. et al. Prognostlc slgI1iflcance of interphase E5H~., ~o,.,odcnal sorne questions remain unanswered: what
will
be the relapse gammopath~1 of undetermined significance. Leukemia 2018;3:2:1811-1815. rate after the intensive treatment?; Howwill
relapsing patients 9. ~1erz, H et =:1 CynçenetiC ab~or'11a~es ii morcdot.e; G8mrm:mtny o~respond ta their subsequent treatment? Similar questions undetermned siglificar:C9. Leukemla 2018; Epub ahead of print
can he proposed regaroing the daratumumab-treated patients. le, Go. R. 5 .. GLn.;:!n.,r-,. J. D & i\9ll:"'.eI'. J M Determining the clin!cal signifk:anœ
Taking iota accaum these question, it is impanant to res- cf moncclol"a1 gai1mopa~tr;J 0' urce:ermined significance: a SEEA-~.1e:jicar9
train [hese approaches to patients with a high-ri..s~{ of pro- pc::;...Iation anal';sis. Clin IymP. rfr/91 8. feu-< 2Gi5;1E"F?-l95.
gression that justifies a [herapeutic imen"emion. 11, Go, R. S. & Rajkumar, 5, V. How 1 manage monoclonal gam/'Tlcpaihy of undetermined signiflcance, Blood 2018:131 :163-173,
CONCLUSIONS
12. Chaudhry. H. H .. "auermann. H L. & RaJkumar. S. V. f.~orockJnaJGamma-MGUS is a frequent abnormali[y especially i::-L the aIder pattl/-ASSoci8ted Peripheral Neuropattl}: Ds.;:;noss and ~~anagemer,t ivlayc population. In most cases, its diagnosis 1S accidentai and [he Cllolo proc 2017;92:838·850.
work-up
will
rarely lead to the diagnosis of an oven malig- 13. Leung, N. et al. Monoclonal gammopalh'l' of (ena! significance: ... e'l MGt.iS nancy. The general risk of progression is1%
per year, but 15 no longer undeterrnined Of Inslgnificanl Sicod 2012;120:4:292-4295should be adapred to every individual situation, depending 14. ~/Ie, R', A. et al, Clinical course and prognosis of srnoldering (asymptomatic)
on the different known factors but also with the help of the multiple m~'8loma. N Engl J Med :2807:33e:2582-259C
cytogenetic raols if possible. More caution is needed in the 15. Lakshman, A et al. Risk strattficatl':Y1 cf smc'::;eri:1ç muitip 9 myelcma,
:nc:x-tOllow-up of SM>1 patients who have a higher risk of pro- poratlrç 'EMsed IMWG diagnos1lc cril..-•. 31oc" 20'3,8:69.
gression ta MM. The recent IMWG criteria redirected ultra- i5. Csars. J. et al. The Olanging Landscape 01 Srooidering Multiple Myelome: high risk SMM patients [Q treatment-rt:quiring MM patieus. .:.. aJropeaI1 Perspecti'.-a. Oncologlst 2016;21:233-342.
17. Meteos, ~t V. et al. ll3naIldcmJde pk.Js dexamethasone fC"" t Çh'';51( smoId!'lfk"lg
REFERENCES
rru~Jp~ myekxna. N Engl J Mad 2013;369438-447Î. Ra.)(c..rnar, S. V. et al. lntemational Myeloma WOrklng Group updated cn;:ër'::: 18, rv.el.~s, rV1.-'), et al. O_rati'iEl 5trateg',' for High-Risk 5molderlng ,\/l~ s'oma.
~or ~r;5 jieQ'1osls af llt.!tiple 1T;''$lar.''iê.. !...a."~( C'I1col 2'J1"'-, ·15,6538-543 (GEr..l-G=s.':";:1)' Ce. -:Uzo'Tl!b. LS1Slidorrids a -,~ DexarreTIBSc1e (\<pc) ":'.S lnou
e-2. Cëe.rs. ,J et al Tr-a Changi'l;) Lardsca']9 0' $rncce,1ng H:.Jbple ~"'I're:or.le. t.CI" FolIC'M'ed By HDT-.... SC-. Gcr,smoE::icr 'Ai:~~"C alc "·)antef'al'lC9 ·/I,;·th Rc A European Perspective. Oncobgist 2016;21:333-342. Slooc 2(;-17;i30 402-402
3. CaefS, J. et al. Dlagnosis and follow-up of monoclonal gammopathies ct :S. l-of,""l8l:ltSi", C C. e-:: al. Daratumumab MonotheraP"/ '0( ::Iatie1ts lNitt'I urdetermined s~ni1îcance: Information for refemng physlcians, Annals of msdl- Intermediate Of High-Risk Smoldering Multiple t.1~eIoma (S~~~ 1): Centaurus,
cine 2013;45:413-422, a Randomized, Open-Label, Mullicenter Phase 2 Study. Blood 2017:130'
4, Bosseboeuf, A et al. MonoclonallgG in HGUS and multiple rTl'/eloma targets é-Q-SIC
infeclious pathogens . .x::llnsight 2017;2, '2C Caa's. J. et al. An European M;eloma Nelwork recommendation on \ools 5. 1'(19, R. A. el al. A Iong·term sludy of prognosis ln monoclonal gano-::-·OQ6.Tj '0' ~lagr.cs.3 and mo"i[:Jn~,~ ~f ilJb:Jle m;'-elo1i:! wt~ t~ ~S~ and >Nhen.
of undet&minec signifca .... ,:::e. N Engl J Med 2002:346:564-ë5S. r-.aematologica 2018; in press