HAL Id: hal-01936639
https://hal-mines-albi.archives-ouvertes.fr/hal-01936639
Submitted on 27 Nov 2018
HAL is a multi-disciplinary open access
archive for the deposit and dissemination of
sci-entific research documents, whether they are
pub-lished or not. The documents may come from
teaching and research institutions in France or
abroad, or from public or private research centers.
L’archive ouverte pluridisciplinaire HAL, est
destinée au dépôt et à la diffusion de documents
scientifiques de niveau recherche, publiés ou non,
émanant des établissements d’enseignement et de
recherche français ou étrangers, des laboratoires
publics ou privés.
Plas’O’Soins: An Interactive ICT Platform to Support
Care Planning and Coordination within Home-Based
Care
Elyes Lamine, Rémi Bastide, Marinette Bouet, Paul Gaborit, Didier Gourc,
François Marmier, Hervé Pingaud, Michel Schneider, Farouk Toumani
To cite this version:
Elyes Lamine, Rémi Bastide, Marinette Bouet, Paul Gaborit, Didier Gourc, et al.. Plas’O’Soins:
An Interactive ICT Platform to Support Care Planning and Coordination within Home-Based
Care. Innovation and Research in BioMedical engineering, Elsevier Masson, 2019, 40 (1), pp.25-37.
�10.1016/j.irbm.2018.10.015�. �hal-01936639�
Plas’O’Soins:
An
Interactive
ICT
Platform
to
Support
Care
Planning
and
Coordination
within
Home-Based
Care
E. Lamine
a,b,∗
,
R. Bastide
a,d,
M. Bouet
c,
P. Gaborit
b,
D. Gourc
b,
F. Marmier
b,f,
H. Pingaud
a,e,
M. Schneider
c,
F. Toumani
caToulouseUniversity,ISIS,InstitutNationalUniversitaireChampollion,RueFirmin-Oulès,81104Castres,France bToulouseUniversity,IMTMinesAlbi,DepartmentofIndustrialEngineering,RoutedeTeillet,81013AlbiCedex9,France cClermontAuvergneUniversity,CNRS,LIMOS,63170Aubiere,France
dToulouseUniversity,CNRS,IRIT,F-31432ToulouseCedex04,France eToulouseUniversity,CNRS,LGC,F-31432ToulouseCedex04,France
fStrasbourgUniversity,CNRS,BETA,av.delaForêtNoire,67085StrasbourgCedex,France
h
i
g
h
l
i
g
h
t
s
g
r
a
p
h
i
c
a
l
a
b
s
t
r
a
c
t
•DesigninganICTplatformfor supporting coordinationhomecareprocesses.
•Defining aDSL specifyingcare plans al-lowing transition towards the planning task.
•Providingacareplanverificationapproach basedontimedautomata.
•Providing analgorithm for planningthe daily activities with multiple time-windows.
•Testingandvalidatingallproposalsinreal conditionswiththeuserpartners.
a
b
s
t
r
a
c
t
Keywords:Homecare Coordination Personalizedcareplan Dynamiccareplanning Domainspecificlanguage
Background: DuetotherisingdemandinhomehealthcareservicesinFranceaswellasinotherEuropean countries,homecareorganizationsarefacingchallengesintermsofcoordinationandcontinuityofcare.In bothcases,theproblemislinkedtotheefficiencyinwhichcareinterventionsaredistributedandmanaged amongthedifferentparticipantsinvolvedinhomecareprocesses.ProjectPlas’O’Soinswhichwasdeveloped withintheframeworkoftheFrenchresearchprogramTecSan,aimstoaddressthesecontemporaryproblems byprovidinganinteractiveICTplatformtoimprovecoordinationand continuityofcarewithinhomecare organizations.
Mainachievements: Plas’O’Soins, the software platform wedesigned, supports care specificationas well as planning and monitoring of the care plans. It allows the modeling of careplans usinga dedicated Domain Specific Language, the schedulingof careoperations taking intoaccount the human resources, themedicalconstraintsandthegeographicaldistributionofpatients,andthemonitoringoftheexecution of the operationsby the careactors. Thissoftware platform enables the coordination of activities and thecommunicationbetweenactorsandreactstounforeseeneventsandproducesdashboardsinorderto quantifytheeffectivenessoftheprocesses.
*
Correspondingauthor.E-mailaddresses:[email protected](E. Lamine),[email protected](R. Bastide),[email protected](M. Bouet),[email protected](P. Gaborit), [email protected](D. Gourc),[email protected](F. Marmier),[email protected](H. Pingaud),[email protected](M. Schneider), [email protected](F. Toumani).
Conclusion:The softwareplatform hasbeen deployedand used inan experimentalsettingby homecare partnerorganizations,providingvaluableinsightsontheorganizationalchangesrequiredbytheintroduction ofsuchanICTsolutionintheactualpracticeofhomecare.
1. Introduction
Over these last decades, there has been a significant demo-graphic shift,including the aging of the population. This demo-graphicchangeisaccompaniedbyanincreasedproportionof frag-ile andelderlypersons,witha correlatedrise inchronicdiseases (e.g.diabetes,heartfailure, etc.)thatrequirecontinuous monitor-ing and care management on a long-term basis. Faced with this evolution,hospitalsbecomeunable tomeet caredemands andin order to relieve their congestion, home care organizations have become increasinglycommonin healthcaredelivery.Indeed,they ensurethetransferofanimportantpartofpatientcarefrom hos-pitals to patients’ homes by coordinating theactivities ofall the personnelinvolvedinthepatient’scareprocess.
Withinthe home careenvironment, care coordination is con-sidered as both crucial and timely for the efficient delivery of provided care services. Home care activities forma collaborative process, which is a set of potentially linked set of interventions regardingsocial care, healthcare,or both [1]. Inthiscontext, an intervention describes a visit at the patient’s home, undertaken by a medical or paramedical staff on a specified time slot. In other words, an intervention is composed of several medical or technical actsperformedby the staff on a single visit. Currently, home care organizations are facing many management hurdles mainly in terms of coordination, which manifest at two levels [2]:(1) Theinterventionslevel:wheredifferentsocialand health-care providershaveto organize thedelivery ofhome care activi-tiesandinformationexchangesregardingcarriedoutinterventions. (2) Thetransitionsovertimelevel:where thestakeholders must ensure continuity andconsistency of provided care between dif-ferentepisodes ofcaretransitionandacross thefull spectrum of patient’scare,particularlywhenmovingfromonecareinstitution toanother.
Thecoordinationofhome-basedinterventionsatthefirstlevel isgenerallyfocused onthe follow-upofproperrealizationof pa-tientcareplans.Thesecondlevelofcoordinationismainlyrelated to the continuity of care over time through the integration, col-laborationandsharingofinformationbetweendifferentproviders. The coordination at this level simply consists of organizational shiftingofcareresponsibilitiesandthetransferofcurrentpatient stateconditionandeventuallytheenactmentofcarehistory.
Referring to the above-mentioned levels the focus of Plas’O’-Soinsprojectisonthefirstlevelofcoordinationsinceweconsider it to be a fundamental step forhome-care management. Indeed, this level of care coordination focuses on organizing staff and other resources to carry out the required cares while managing theexchangeofnecessaryinformationamongthedifferentactors involved in home-care processes. WithinPlas’O’Soins project, we attempttodevelopanICTplatformforbettermanagingthe coor-dinationofcareandservicestopatientsathome,abetterflowof information relatedto patientsand a better monitoringof home care in a context of improved quality of services andcontrol of public health expenditure. We recommend an explicit specifica-tionofpersonalized careplansinorderto deducethescheduling of all the visits. The main processes are thus: Editing personal-izedcareplan,Home-careschedulingandrouting,andMonitoring home-careinterventions.
Thepaperisstructuredinthreemainparts.Inthefirstone,we presentastateoftheartoftheuseofICTmethodsandtechniques forhomecareandwepointoutthechallengesforthis.Thesecond partisfocusedonthepresentationoftheresultsobtainedwithin thePlas’O’Soinsproject,inparticularthedesignofthethreemain processesandtheimplementationoftheICTplatform.Inthethird part, we discusstheobtained resultsandwe put theminto per-spective withongoing work.Finally,we providea conclusionand futureoutlook.
2. Stateoftheart
Theinterestofusinginformationandcommunication technolo-gies(ICT)tosupporthomecarehaslongbeeninvestigatedthrough numerousstudies, bothinacademic andprofessional circles.This work resulted in recommendations, prototypes and commercial-izedsoftwareplatforms. Wefirstpresenta globalvision,thenwe focusonpointsofinterestrelatedtothePlas’O’Soinsproject. 2.1. GlobaloverviewofICTinhomehealthcare
First attempts to use ICT for home care are related to tele-medicine. Telemedicine started early 1990s with the advent of audio and video technologies. Telemedicine can provide valuable help for home care [3]. Its simplest form is telenursing, which allowsremoteconsultationorremotemonitoring.Remote monitor-inginvolvesvariousdevicesusedbythepatientathometocollect andtransmit medicaldata.Thesetechnologies areused to allevi-ateorevenavoidsomeofthehomevisits.Telemedicine forhome care hasbeentestedwithsome successDarkins etal.[4], Kamei [5].Costreductioniseffective,butsocialimpactremainstobe as-sessed precisely. Telemedicine benefits now fromthe accelerated developmentofmobiledevicesandconnectedobjects.
NumerousstudieshavebeendevotedtothedevelopmentofICT platforms integratingsome orall ofthe functions forhome care. The principles used are varied: ECA rules approach [6], Ethno-graphic approach [7], Ontological approach [8,9], Multiagent ap-proach [10,11], Process approach[12,13]. Initiatives are academic and professional. Numerous commercialized software have been proposed intheAnglo-Americancontext(ConsumerAffairs1)orin
the Francophone context (we can cite Arcan2 or Medlink3). The
functionalitiesofferedbythissoftwarecanrelatetofinancial man-agement, patient management,remote accessvia mobile devices, sometimes scheduling androuting home visits. Such software is generallyexpensive.Apreciseassessmentoftheuseofthese pro-totypesandsystemsinrealconditionsremainstobeestablished. 2.2. Careplanmodelingandverification
Oneofthemaindocumentsinhomecareisthecareplanwhich istheplannedlistofcareactstobeperformedforapatient[14]. The care concern acts andtreatments to which are associated a
1 Compare Reviews for Best Home Health Care Software http://www. consumeraffairs.com/online/home-health-care-software/.
2 AtHomesoftwarehttp://www.arcan.fr/logiciel-suivi-soins-a-domicile.html. 3 MedLinkproducthttp://www.med-link.org/.
frequency and schedules [15]. This is a reference document for allactors.Tomodelandexploittheinformationcontainedincare plansisthusextremelyimportantifwewishtofavorinformation exchangesbetween thedifferentactorsimpliedinhome careand toimprovethecontinuityofthecare.Therearemedicalontologies (CIM10,CCAM, ...)orstandardssuch asHL7onwhichthe defini-tionofacareplancanbebased.Butitisalsonecessarytodefine theoperationalpart(resources,duration,frequency)oftheactsto becarriedout.In[16,17],theinteresttodesignstandardizedcare plansandtodefineagenericframeworktoimprovethepracticeof homecareisunderlined.Hägglundetal.[18] goesfartherby high-lightingthenecessarymatchingbetweenthestandardsofmedical representationof knowledge and the systems ofexchange of in-formation.Anotherproblemisthenecessityto verifythevalidity ofthecareplanbeforemakingtheplanningoftours.Wealso no-tice alack of IT supportin the checkingofthe care plan during itsediting.Finally,italsoseemsimportanttocontextualizeor per-sonalizethecareplan,whichwematerializedbyadomain-specific language(DSL)inPlas’O’Soinsproject.
2.3.Homecarescheduling
Main researches in the field of home health care, concerning routing and scheduling problems which are an instance of VRP problems, started around 2000 with, for example, the works of Hindleetal.[19,20] concerningresourceallocationandtravelcost approximations.
Ernstetal.[21] proposesanimportantannotatedbibliography synthesis on computational methods for rostering andpersonnel scheduling.Theauthorsclassifyarticles,morethan700references, according to the type of problem addressed, the domain of ap-plication and the methods used. In addition, Rinder et al. [22] present a systematic literature review of the application of in-dustrialengineeringmethodsinhealthcarescheduling. Techniques andmethodsthat havebeenusedinpastworksare multipleand cover a huge part of industrial engineering methods and Opera-tionResearchmethods.Theycanbedecomposedinexactmethods (Linear Programming, Tree Search Space, Branch-and-Bound and Constraint Programming), heuristics methods and metaheuristics methods (like Variable Neighborhood Search, Simulated Anneal-ing,Evolutionary Algorithm).Moyauxetal.[23], Burkeetal.[24] andMeiselsandSchaerf[25] developanapproachbasedona con-straintsatisfactiontechnique;BeddoeandPetrovic[26] useacase based reasoning approach; Chen andYeung [27] and Yeung [28] proposeanexpertsystem;Bachouch[29] usesheuristicsand meta-heuristicstechniques;tabusearch;Akjiratikarletal.[30] propose an original approach using an algorithm of Particle Swarm Opti-mization(PSO)tobuildthescheduleofthehomecareactors.This algorithmcombinesaglobal explorationofthespaceofthe solu-tionsandaprocedureoflocalsearch torefinethesolutionby an analysisoftheneighborhood.
InthePlas’O’Soinsproject,wetackleaspecificproblemof rout-ingandschedulingwhich iscalledVehicleRoutingProblem with MultipleTimeWindows(VRPMTW).Thisproblemisderived from the VRPTW problemwhich is an extension of the VRP, where a specificconstraintisadded,requiringthestartofserviceforeach customer within atime window. Vidal etal.[31] propose an ex-tensive state-of-the-art of methods used to solve severalrouting andschedulingproblemsderivedfromVRPTW.Toourknowledge, theVRPMTWhasreceived relativelylittle attentioninthe opera-tionsresearchliterature,ithasonlybeeninvestigatedbyFavaretto etal.[32] in2007.InthecontextofHomeHealthCare(HHC),there wasnoworkdealingwithVRPMTWforHHC,noresultshadbeen producedbeforetheprojectstarted.
Basedonseveralstudies [33–37], FikarandHirsch[38] extend theliteraturereviewofHHCrouting andschedulingpapers.Their
review is structured in two classes of works: first those related to single-period home healthcare problemsandthen those con-cerning multi-period home health care problems. Based on this categorization, FikarandHirsch[38] propose asystematicreview ofobjectivesandconstraintsmodeledinHHCroutingand schedul-ing problems. Objectives identified in this literature review en-hancethesetofobjectivesclassicallylistedinVRPproblems.The objectives mentioned in HHC worksconcern several dimensions: traveltime,travelcost,traveldistance,waittime,overtime, prefer-ence, numberofnurses,softconstraintviolations,fairness (work-load balance), number of tasks, patient preferences, staff prefer-ences.Additionally,asetofconstraintswasidentifiedbyauthorsin HHCworks, thislistiscomposedof:time windows,skill require-ments,workingtimeregulations,breaks,precedence, synchroniza-tion,workload balance,uncertainty. Noneofthe worksidentified implementssimultaneouslyalltheitemslisted.
To manage the optimizationprocess, most ofthe authors de-velopamonoobjectiveapproachwhichcanbetheconsolidationof severalelementaryobjectivesinaconsolidatedobjectivefunction. Someotherworksproposeabi-objectiveapproach,asforinstance Braekersetal.[37].InthePlas’O’Soinsproject,wehavechosento implement a two stage approach combining multi objectivein a firststepandthenanaggregatedobjectivetoselectthebest solu-tions.
2.4. Monitoringhomecareinterventions
Monitoringhomecareinterventionsconsistsofkeepingtrackon the implementationof the plannedinterventions inorder to en-suretheproperexecutionoftheprescribedpatientcareplansand to alertthe coordinatorin theeventofunforeseen problems.For thisreason, it is essentialto haverelevant situationalknowledge aboutthefieldbyobtaining timelyfeedbackwhichallowsthe co-ordinatortomaketherightdecisionsattherighttime.
Mobiledevices, suchassmartphones,tabletsandsmartwatchs, arerecognizedasbeingessentialforreceivingimmediatefeedback, inthehomecaredomainparticularlythroughcontinuousdaily pa-tient monitoringand checkingcompliance withself-management programs. Nowadays,manypromisingprojectsexistbasedonthe useofmobiledevicesandallowing theremotemonitoringof pa-tients’ basicvitalsigns andtogeneratealerts incaseofanomaly [39,40]. However,despite all thebenefits that can arisefrom the use of mobile device in healthcare domain, there are still many challenges that must be overcome, and among which stand out userattitudes,technologyacceptanceandthreatstoconfidentiality andprivacy[3].Tothisend,aparticularattentionwaspaid,within the Plas’O’Soins project,to the acceptability of the proposed so-lutions andtothe securityandconfidentiality ofthestorage and exchangeofdata.
ThestateoftheartatthebeginningofthePlas’O’Soinsproject can be summarized asfollows: We observe a good understand-ing of the differentfeatures ofcoordination and communication, butitremainstheneedtoevaluatetheproposalsinrealcontexts withasufficientvarietyofsituations.Schedulingandrouting solu-tionsaretoooftendisconnectedfromotherfunctionsanditexists astrongrequirementtoadaptthemtotheconditionsactually en-countered by the home care structures, taking into account the planningdynamicsandtheuncertaintiesofoperations.Wenotea lackofaprecisedescriptionofthecaretobecarriedoutwith con-sequentinabilitytocheckforinconsistenciesandmakethelinkage withschedulingandrouting;Itremains thenecessityto fully in-tegrate the different processes, going from patient admission to patient exitandtakingintoaccountcarespecification, scheduling androuting,coordinationofactors.
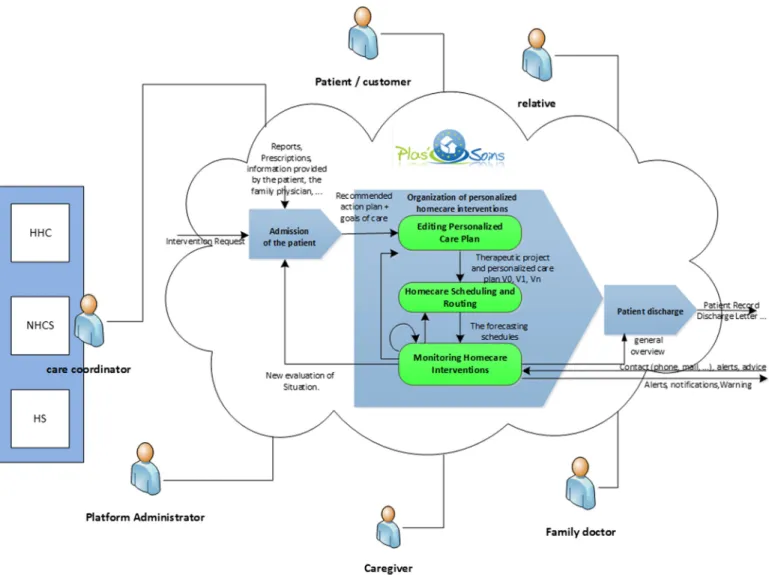
Fig. 1. Overview on the functional architecture of the Plas’O’Soins Platform. 3. Mainachievements
3.1. Overviewonthefunctionalarchitectureoftheplatform
The diagram inFig. 1 provides a broadoverviewof the func-tionalarchitectureoftheplatform.Itisprocessoriented.Thethree main processesconstitute thebackbone aroundwhich other pro-cessessuchastheadmissionprocessorthedischargeprocessare organized:(1) EditingPersonalizedCarePlan:Itisbasedona Do-mainSpecificLanguage(DSL)approachformodelingacustomized careplanaccordingtothepatient’sprofile;(2) Homecare Schedul-ing and Routing: It is about the finding of a weekly assignment ofcaregiverstohomecareinterventionsaccordingtopatients’care plansandgeneratingtourstakingintoaccountmanyspecific con-straints; (3) MonitoringHomecare Interventions: It isfocused on thefollow-upofproperrealizationofpatientcareplans.
These components are described more specifically in the fol-lowingparagraphs.
Thisdiagramalsoshowsthedifferenttypesofactorsandtheir interactionswiththeprocesses.
3.2. Careplanmodeling
All the medical andsocial activities delivered fora given pa-tient according to certain frequencies are scheduled in a home care plan. Hence, the notion of a care plan is a key concept in home care area. In thePlas’O’Soins project, we are interested by
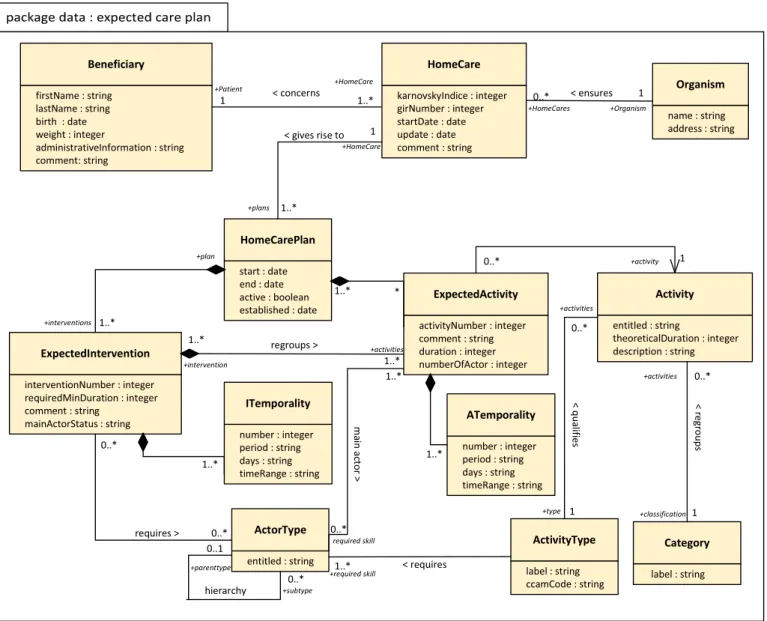
theproblemsunderlyingthedesignandmanagementofthehome careplanstobringsomecomforttothemedicalcoordinator,avoid the collision when planningactivities or toensure the feasibility of the home care plan. After a domain analysis performed with end-users, we proposed to describe home care domain concepts throughUMLclassdiagramsaccordingthethreevisions(expected, plannedandperformed)ofthecareplan(Fig.2).Havingan appro-priate externalrepresentationofthecareplanisappearedcrucial to assist asmuch aspossible the medicalcoordinator inthe de-signofindividual careplans.That’swhyweproposea DSLbased approach, tailored to expresshome care plans using abstractions highlightedintheUMLanalysis[41].
The DSL consistsof all the objects that can appear ina care planandoperations thatcanbemadeontheseobjects.The activ-ity (act)isthe centralconcept.It mustbe performedby an actor of a certain type (physician, nurse, nurseauxiliary, liberalhelper ...)withsomequalifications.Theactivitymayalsoinvolvematerial resources andconsumablesthatthesystemmustbe ableto man-age.Thesetofactivitiesisknownandstoredinaknowledgebase. Each activity is associated with theactortype (nurse, nurse aux-iliary ...)and anyconsumables.An indicative duration ofthe acts (e.g.average ofthedurationsalreadyobserved) isalsosuggested. Allthedataarestoredintheknowledgebase.
An intervention isa groupingof actswhich cantake place in thesametimeslotandwhichcanbecarriedoutbythesame ac-tor. Thankstothisconcept,we switchfromthemedicalvisionof thecareplan(patientoriented)totheoperationalplanofthecare
Fig. 2. One of our class diagrams: prescribed view of the care plan.
plan(actororiented).Therearealwaysseveralpossibilitiesfor dis-tributing the acts into interventions andthe search for the best solution is not trivial. Our system suggests interventions, which thecoordinatormayrearrangeashepleasesandfinalizethem be-foremovingontotheplanningstage.Therulesusedtoinferthese interventionsare asfollows:theactsinvolvedinthecomposition havecompatibletimeslotsandcanbeperformedbythesametype ofactor.
Finally, an intervention is defined by the acts that compose it(with possiblesuccessional constraints),a time slot,a duration (sumofthedurationsoftheactsformingpartofitscomposition), a type of actor(possibly an actor). The planningmodule will be responsible,foreachoccurrenceofanintervention,tosetthestart timeandendtimeandassignittoatourandanactor.
Toassist the coordinator, the care plan may be displayed ac-cordingtoadevelopedform(agendaform)(Fig.3)and/or accord-ingtoacondensedform(Fig.4)knowingthatthedevelopedform isdeducedautomaticallyfromthecondensedform.Thecondensed formisclosertocommonmedicaluse(semi-naturallanguage)and easiertocommunicate.
Thecondensed formisused by thecoordinator tospecifythe careplan.Foreachact, itindicates itstime slotandfrequencyof repetition(everymorning–everyMonday,WednesdayandFriday
at 18h), certain constraints for actors (type, status – liberal, not liberal–,preassignedforthepatient).
OurDSLhasbeendesignedtoofferavarietyofpossibilitiesto specifytherangeandfrequencyofanact.Italsomakesitpossible to indicate the particular casesand exceptions. Temporal modal-ities are formalized as a quadruplet (Days, Time ranges, Period, Duration)where(1) Period:specifiesthetimeperiodduringwhich theactivityisdefined,(2) Days:indicatesthedayswithinaperiod inwhichanactivitymusttakeplace,(3) Time:rangesindicatesthe timeslotsinwhichtheactivitycanoccurand(4) Duration:gives theoretical duration which corresponds to the averageof already observeddurations.
Days andTime ranges attributes can take several patterns to correspondtothedifferentpossibilitiesencounteredinthemedical world(e.g.onmorning,onMondays. . . )andexceptionsclausesare introduced via the keyword “except” (e.g. every day except pub-licholidays).Forcontrollingthespecification,we haveproposeda languageexpressedinBNFformwhichenablesregularorirregular repetitionsofanactwithinsomeperiod[42].
The DSLconcepts allowusto describe thehome caredomain concepts throughtheUMLclassdiagramsandcanhandle tempo-ralirregularities.Through thecondensed ordevelopedforms,itis not obviousatfirstglance whethertheplan carecontains
incon-Fig. 3. Specification of a care plan: agenda form.
Fig. 4. Specification of a care plan: condensed form.
sistenciesortimeimpossibilities.IntheFig.5,aproblemariseson Sunday,January11th,2015fortheactParenteralnutrition.Sothe careplanisnotrealizable.Thisiswhy,weproposeatool(cf.next section)toverifycareplanbeforestartingtheplanningstep. 3.3. Careplanverification
It is important to provide toolsto assist as much aspossible themedical coordinatornot onlyin thedesignof individualcare
plans,butalsointheautomatedsupportforverificationoftheplan andmonitoringof itsexecution. Althoughthecondensed formof careplansallowsmoresophisticatedreasoningthanthedeveloped form, a more formal representationisneeded tomeet theneeds forcontrolofthecareplan.Astemporalconstraintsplayacrucial roleinhomecares,theproposedformalizationisbasedonexisting theoryandtoolsinthefieldoftimedautomata[43,44].Obviously, this projection inthe timedautomaton field iscompletely trans-parent to the coordinator. He continues to design the care plan
Fig. 5. Example of a non-realizable care plan.
asexplained inthe previous section. From there, the system au-tomaticallytransformsthe careplaninto atimedautomaton and indicateswhetherthecareplanisfeasibleornot.Moregenerally, this transformation is indispensable to perform any kindof ver-ification and monitoring of the home care plan. In the field of automata, the notion of a medicalor paramedical act is assimi-latedtoanactivity.Therefore,weonlyusethisdesignationinthe restofthissection.
Ourapproachisbasedontwosteps:
1. Definitionoftheactivityautomaton:Theobjectiveofthisstep istomap eachactivityinto anactivityautomaton.The prob-lemissimplewhenthetemporalityofanactivityisexpressed throughasinglepattern.Eachpatterndefines, throughits du-ration and period, a pattern automaton which becomes the activityautomaton.ThiscaseisillustratedinFig.6forthetwo activities. Theproblemis morecomplex when the temporal-ityofthe activity usesseveral patterns.The resultedpattern automata mustbe assembled together to generatethe activ-ityautomatonaccordingtotheclassicalintersectionoperation [43].Ifanirregularityisindicatedatthelevelofatemporality, thecorrespondingexceptionistranslatedintonewtransitions andguardsonthepatternautomaton.Explanationsand exam-plesillustratingthesecasescanbefoundin[45].Theresulting timedautomaton recognizes all possible timedwords corre-spondingtoallthepossiblecorrectschedulesoftheactivity. 2. Definitionofthecareplanautomaton: The construction of
thecare plan automaton fromthe activityautomata is auto-matic.Itusesaspecificpersonalizedcompositionoperatorbased on an asynchronous product on some states, on a synchro-nization productonwaitingstatesandonblockingoperations in the execution states.It must also guarantee that a single activityis executed at a precise time t. Mostof the existing works considered timed automata without duration. In our approach, we handle the problem of duration by extending the basic model of timed automata with the notion of exe-cutionstate andby redefiningthecomposition operator.This extension does not increase the expressive power ofthe ba-sicautomata,andhence,does notimpacttheircomputational properties.So,acare planautomatondescribesall the possi-blelegalschedulesofa homecareplan foraspecific patient (Fig.6).
Oncethecareplanautomatonisgenerated,weusetheUPPAAL ModelCheckertotestthemodelobtained.Inourcontext, satisfy-ingpropertiesallow usnotonlyto checkthe feasibilityofacare plan (the classical emptiness problem[46]), butalso to compute automatically interventions (grouping of activities of home care
plantominimizethetotalnumberofinterventionsandtoreduce thecostofhome care).Furtherdetailsmaybefound in[45].The proposed system (DSL
+
timed automata+
model checking) is usedto movefromapatientorientedprocess (amedicalviewofa patient-specificplanofcare)toaoperationalprocess(estimated in-terventions)ofthecareplan.3.4. Homecareschedulingandrouting
In home health care (HHC), planners have to schedule inter-ventionsidentifiedincareplans, whichareassociatedtopatients. Eachpatienthavehis/herowncareplanwhichismodeledas pre-sented above in section 3.2. So, a home care structure have to organizeoperationsforseveralpatients/clients.Plannersassign ac-tors(nurse,nurseauxiliary,...)topatients,scheduleworkingtimes andidentifyarrivaltimesofnursestoeachpatient.Forthis,travel routeshavetobeidentifiedandevaluated.
Severalrequirements,expressedbystakeholders,havetobe in-tegrated in the scheduling procedure, such as matching nurses’ skill and patients’ wishes or medical requirements [38]. In this study, we have classified requirements and hard constraints ac-cording to threepoints ofview: nurseoriented, patient oriented or,structure andtouroriented. Some examples ofconstraintswe have modeled for each point of view are presented below. Con-cerningnurses’wishes,theassignmenthavetorespectcontractual andlegalworking time ofeach nurse,andtolimit waiting times i.e.nointerruptionsduringthetour.Individualpreferencesofeach worker can be used to organize the planning. For patient, con-straints modeled are: respect of visitingtime windows given by thepatient(itcanbeconsideredoneorseveralpossibletime win-dow fora givenvisit),respect ofthetime between twoor more visits on the same day for a specific patient. Home health care structure constraints are rules which hold forthe entire organi-zation, they are often based on legal regulations constraints as: respectingworkers’legalworktimebyday,byweek,bymonth(e.g. minimum/maximum hours ofwork by day,by week, by month), respectingskillsandqualificationrequiredtorealizethe interven-tion, all the interventionsidentified in the care plan have to be plannedfortheexpecteddaywhichareexpressedinthetemporal modalitiesofthepatient’careplan(see3.2),minimizingthetravel trip(durationanddistance).
IntheprojectPlas’O’Soins,wefocusonadailyhomecare rout-ing andschedulingproblem.One oftheoriginalitiesofthiswork concernsmultitimewindowrequirements’expression.Inthisway, theoptimizationprocessallowstotakeintoaccountpatients’ pref-erencesexpressedwithmultipletimewindows.Patientscanallow severaltime-windowsonadayfornurses’visit.Forexamplea pa-tientcanbevisitedbyanactorifherespectsthe nextconstraints:
Fig. 6. Process of definition of the care plan automaton.
Fig. 7. Examples of five tours’ planning.
(between8 h 30and9 h30) or(between 11 hand12 h).These time-slotsaremodeledinthecareplanduringthefirstvisitofthe HHCcoordinatoratpatienthome.
Based on these constraints and requirements, the optimizer modulehavetogeneratesolutionsandgivethebestones.Forthis, we have developed a specific set of objectives according to the strategy of the HHC’ partners of the project. In this project,the objectiveshavebeencategorizedintwoclassesofcriteriato
eval-uateeach solutiongenerated.Thefirstclassiscomposed ofthree criteriathatarethemostimportantweightintheevaluation pro-cess:maximizingthepatients’preferenceswhichisexpressedwith time windows respect (c1). Time windows for each intervention
are definedinthepatients’careplan;minimizingtheplannedtour overtime (c2) forrespecting nurses’work time. Thisobjective
fo-cusedonbothminimizingthetotalworktimefornursesandaims tolimittheovertime;maximizing therespectoftime interval
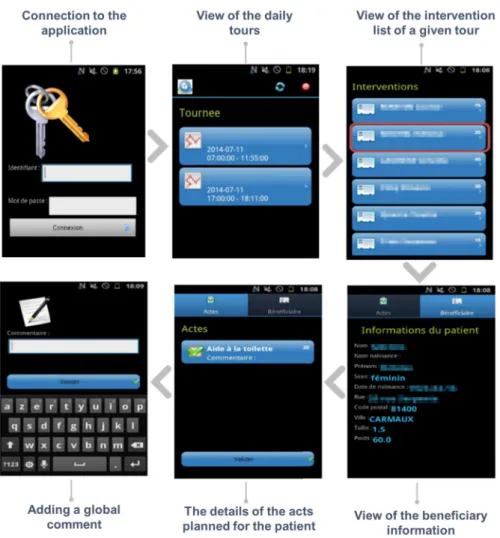
be-Fig. 8. An overview of the mobile user interface.
tweentwovisits(c3).Thesecriteriaaimtovalidatetherealismof
thesolution,theycorrespondto constraintstocomplywith. Thesecondclassofcriteriaconcernsattributesthathavetobe optimized:traveltime(c4);maximizingovertimeequilibrium(c5).
Thesecriteria aimto minimizethedifferencebetween thelongest serviceandthe shortestservicetimes amongthe workers; hard-nessequilibrium(c6).Theselastthreecriteriaareaggregatedwith
alinearfunction.
Thesolutionadoptedtogeneratethetours takingintoaccount those specific requirements and constraints consist in a meta-heuristicapproachbasedontabusearchtechniqueassociatedwith neighborhoods generation technique to explore solutions [47]. In the proposed approach, three types of neighborhoods generation havebeenintroduced:shiftintervention,swapintervention,OrOpt insertion.
3.5.MonitoringHomecareInterventions
As shownin Fig.8, a specific applicationhas beendeveloped onAndroid Smartphonestofollow-uptheproperimplementation ofplanned visits. It allowsto visualize the dailyScheduled tours andthe list of patientsin the order ofvisit with, foreach one, the surname, the first name and the estimated duration of the intervention. When opening the application, an identifier and a password are required to access the information related to the worker. Thisapplicationalsoallows tosee thedetails oftheacts planned for each patient and to validate their good realization. Aglobal commentforthe intervention could be entered aswell. The information accessible fromthe application is storedon the
smartphoneinadatabaseencryptedwiththeuser’spassword. To send and/or retrieve the information from the server, it is then necessaryto performasynchronization byclicking onthe button dedicated to this function. To do this, it is necessary to have a connection to the Internet network. This synchronization of the exchanged data withthe serveris madevia PHP and storedSQL procedures.
3.6. SoftwarearchitectureandHCI
TheproposedsolutionwithinPlas’O’Soinsprojectisasoftware platformdesignedfollowingtheprinciplesadvocatedbySOA (Ser-vice Oriented Architecture), and including mobile and location-aware devices adapted to the practice of different stakeholders. This platform is based on a model-based architecture (Model DrivenEngineering,MDE),andincludesinparticularthedefinition ofadomain-specificlanguage(DSL)designedafteradetailed anal-ysisoftheactivityofahome caremanager,andthedevelopment ofspecificallydesignedschedulingalgorithms.
Withregard tothe implementation ofthis platform,the soft-ware architecture is made ofseveral components, asdepicted in Fig.9.The serveris installedon anUbuntuoperatingsystem. All datais storedina MySQLdatabase. Aparticipatorydesigned ap-proachwasusedtoguidethedesignofalltheseHuman-computer Interaction (HCI)andthe choiceofinteraction devices. By associ-ating users with the development of systems, it was possible to study the mostappropriate formsof interaction.The coordinator interfaceisaweb-basedinterfacedevelopedinJavausingJava Per-sistenceAPIandTomcat.
Fig. 9. Software architecture.
ThisHCIhasbeendesignedtoallowthecoordinatortointeract withthesolutionsgeneratedaccordingtohisneeds.Itisthus pos-siblefor himto make the necessarycorrections. He willbe able tomove theinterventionsfromonetourto another,orto modify theirschedulingwithinatourandtoassignaspecificcaregiverto atour.
Toimplementthiscoordinatorinterface,weusedVaadin frame-workthatallowstoquicklygenerateaestheticandergonomicweb applicationsusingonlyJavacodethatistransformedandthen gen-eratestheHTMLpages.
The datatransportation between theserver andthe coordina-tion browser or smartphone application is based on the HTTPs protocolandgoesthroughafrontalApacheserver.
3.7. Experimentation
Theaimoftheexperimentwastovalidate thetechnical archi-tectureoftheplatform,theoperationaluseofitssoftwaremodules andthestaffacceptability. Theexperiments havebeenconducted withtheCARMI(aregionalsocial securityinsuranceinthe south westofFrance).Severalcoordinatorsandactorsofthecare activ-ities were mobilizedandspecifically 5Caregivers and1.5nurses. The study covered the cares of 55 patients. Depending of their health, patientsreceived from1 to 2 visits per day, 2 to 7 days perweek.Theseinterventionsweredone,inthemorning(5tours from7:00amto12:00am),intheafternoon(1tourfrom2:00 pm to5:00pm)andintheevening(4toursfrom5:00pmto7:20 pm). Theprotocolto testtheplatform wasestablished overathree weeksperiod.Thefirstweekwasfocusedonthepreparation. Dur-ing this week the Plas’O’Soins consortium ensured the input of the initial information necessary for the experimentation in the databases. Necessary precautions have been taken to ensure the conformityof thesoftwareanddeviceswiththe regulations,and particularlyconcerningthestorageofpersonaldataandthe
host-ingofhealthdata.Thenatrainingwasprovidedtothestaffforthe useofhardwareandsoftwaremodules.
The second week was focused on the experiment itself. The platformbeingaresearch prototype,itwas necessarytouseboth systemsinparallel:usual operationandoperation onthebasis of Plas’O’Soins.Thisreplicationoftheworkwasachievedbythestaff oftheCARMI.
Finally, the third week was focused on the debriefing and on the analysisoftheexperiments. Asurvey was giventoeach par-ticipant tocollecttheirqualitativeperceptionsandassessmentsof theplatformanditsmodules.
Regarding the Interface for entering care plans, the function-alities offered corresponded to the needs expressed initially. The specificationofthetemporalconstraintsoftheactsinacondensed formwasconsideredtoberatherappropriate.Theorganizationof thedialogtocapturethesetemporalconstraintsappearedasbeing adaptedandvaluable.
RegardingthePlanningSoftwareModule.Thismodule,devoted to the staff in charge of coordinating the patient care, defined the patient care plans but also established a schedule of medi-cal andparamedicaltours. Figs. 7a and 7b illustratea fivetours’ planning respectively done by human expertise and by the ap-proachdevelopedinthisproject.Basedonthisexample,whichis anextractfromtheexperimentsthathavebeencarriedonduring the project,the gainobtainedarepresented inTable1.These re-sultsarepromisinganddemonstratethevalueofthisapproachthe value incomparisonwithapurelyhumanapproach.Dueto com-plexityandhardnessoftheconstraintsexpressed,thisapproachis totally adapted because it is able to explore numerous solutions whichcan bebasedonapossiblesolutionwhichrespecta setof identified constraintstoobtain newinterestingones. However, in some casesmanual adaptations are requiredbecauseit is impos-sibletotake allthehumanrulesusedforgeneratingtheplanning intoaccount.
Table 1
ComparisonofthemanualplanningandthePlas’O’Soinssolution(valuesin min-utes). Criteria Manual (see Fig.7a) Plas’O’Soins (seeFig.7b) Gain (%) c1 145 1 99% c2 306 172 43% c3 68 fullyrespect 100% c4 476 362 24%
Theexperimentationhasshowedthedifficultyoffully automa-tizedplanninggeneration.Attheend,adjustmentswerenecessary through the proposed interface. The debriefing phase with care coordinators allowed to identify several rootcauses of modifica-tions:unexpectedinterventionrequiringtwocareworkers, acare worker has an exceptional family constraint, unavailability of an equipment or supplies, etc. So, this module should therefore be consideredasaplanningaid.
Regarding the software module for the consultation of inter-ventions and the capture of achievements on smartphones, this onewasintendedforthemedicalandparamedicalstaffofCARMI, responsible forproviding patient care. This module was used on mobile devices allowing each participantto consult the detailed agendaofthetours.Its handlingdidnotposeanydifficulties.The increase ofavailableinformationcompared tothecurrentway of working was considered as being very useful. In the same way, usersaskedifinformationaboutpatientscouldalsobeadded.
4. Discussion
Inthissection,foreachofthecontributingpointsoftheproject, werecallitscontext,wediscusshowitevolvedwithresearchwork thattookplacelater(after theendoftheproject) andwe reposi-tiontheperspectivesthatremainopen.
4.1. ModelingandverifyingtheHomeCarePlan
Themodelwe haveproposedis oneoftheoriginalitiesofthe project.Itallowsto expressthetemporal andorganizational con-straintsofthecare.It allowstheuseoftimedautomatato check theconsistencyofacareplan.Toourknowledge,itdoesnotexist alternative offeringthesamepossibilities. Thismodelwas reused in [48] to explore another verification approach based on TRE-CANets.TRECANetsarederivedfromPetrinetsandallowrecursion. Theymakeiteasy toexpressaminimumandmaximumduration forcareandtomodelsuccessionsandrepetitions.
4.2.Schedulingandrouting
The approach we have proposed allows to generate a daily scheduling forexecuting the interventionsof the whole patients managedbyahomecarestructure.Thisprocessallowstoexpress patients’ preferences with multiple time-windows and give good resultsontherespectofpatients’preference.Sincetheprojecthas finished, further works have been developed with multiple time windows[49,50] andconfirmtheinterestfortheseproblems.
Theexperimentationphasewasabletoidentifysomelimitsof this work concerning the configuration of the optimization pro-cess, the stability of the plans and the interdependent services scheduling.Inthisstudy,wehaveassumedthatthedecisionmaker (the planner) is able to provide realistic weights for each crite-rionof the objective function. This task can be difficult and the valuesselectedhaveanimportantinfluenceontheresultsof opti-mizationprocess.Aninterestingcomplementaryworkwouldbeto proposeamethodologicalapproachforhelpingdecisionmakersin thistask.
Another setback identified concerns the difficulty of ensuring a stability of the hours of intervention for a patient over time. This functionality which was not satisfied in this first develop-mentcould be usedto implementre-schedulingapproach during the tour.Indeed,when aproblemoccursduring the executionof the plan(new patient,a supplementary intervention, unavailabil-ity ofa worker, etc.), it isvery important that the adaptation of the planin realtime does not modifytoo much theplanned in-terventions.Current works, developedin theprojectANR SMART PLANNING,aimtotakeintoaccounttheseeventsinthescheduling process inananticipativeway inordertogeneraterobust sched-ule. Besides this, recentworks have explored this way to model continuityofcarewiththedefinitionofacriterionmeasuring the totalnumberofdifferentnursesthatvisitthesameclientduringa planninghorizon[51,52].
Sometimes,fortheexecutionofspecificinterventions(i.e. com-plex patients’ manipulation, lifting over-weighted patients), it is necessary to have two or more workers in the same time at the patient’ house. Taking this constraint into account requires synchronizing the schedule of two workers. Further works, like those ofEn-nahlietal.[53] andMankowskaetal.[35],integrate interventions synchronization mechanisms. Forinstance, En-nahli et al. [53] propose an approach based an Iterated Local Search (ILS) metaheuristic coupled with a variant of the Random Vari-ableNeighborhoodDescentmethod(RVND)whichusesarandom ordering ofneighborhoods inlocal search phase (RVND-ILS algo-rithm) to solve thisvehicle routing problemwith time windows andsynchronizationconstraints(VRPTWSyn).
Inrealworld,thepreviousplanningperiodinfluencesthe eval-uation of some constraints (e.g. equilibrium workload, minimum andmaximum numberofconsecutiveworking days) [54]. Inour study, we focused ondaily tour generating.So, itwas not possi-bleto taketheseobjectivesinto accountinoptimization process-ing.
4.3. Architectureoftheplatform
Wechoseaprocessorienteddevelopmentapproachwhich cor-responded to the process modeling we used to model activities. Thedevelopmentitselfwasorganizedaroundarelationaldatabase andinvolvedtheMYSQL,JPA,VAADINtechnologies.Subsequently, we tested,still usingaprocess orientedapproach,adevelopment organized around a NoSQL database with the MongoDB system [55]. MongoDB is a document orientedsystem. We have associ-ateditwithWebServicestotakeprocessesintoaccount.ANoSQL documentorientedsystemhasadvantagesanddisadvantagesthat arerelatedtothetypesofapplications.Designingthelogicaldata modelandimplementing thephysical modelisgenerally simpler andmoredirectthanwitharelationalsystem. Theformatof doc-umentscaneasilybechanged.Butreferencesbetweendocuments mustbemanagedbythedeveloperandaNoSQLsystemmustonly be used forapplications withfairly simple reference schemes.In addition,transactionaloperations are not supported byMongoDB and,ifnecessary,atransactionmanagementmustbeimplemented. Fortunately,ourapplicationonlyinvolvessimplecasesforboth ref-erences andtransactionsandit hasappeared that a systemsuch as MongoDB could bring greater ease of development and offer greateragilitythanarelationalsystem.Forsomeprocesses,andin particular scheduling, it appearedthat users wish to define their own rules.In thisperspective, a development paradigm associat-ingprocessesandrulescouldbeadirectiontoexplore.
4.4. Usages
The experiments showed that the interfaces were appropri-ate forboth types ofactors andthat theplatform could provide
effective assistance at several levels: specification of care plans, scheduling,tours piloting,monitoringcareinterventions.However theplatforminvolvesasignificantchangeinhabitsandamore rig-orousorganization.It isatthislevelthatacceptability arises.The resolutionofthelastminutehazardsismoreconstrainingthanin a manual management.Greater flexibility should thereforebe al-lowedtotriggerdefinitiveacceptancebyusers.
5. Conclusion
The objectiveofthe projectwas to develop an interactive ICT platform tosupport home careservices. Itwas a matter to favor communicationamong actors, coordination ofactivities and con-tinuity ofcare. Theplatform is designedaround threemain pro-cesses:modelingcareplans, planningvisitsandtours,monitoring homecareinterventions.Thesethreeprocessesofferthree comple-mentaryvisionsofthecareplan:prescribedvision,plannedvision, performedvision.The projectintroduced newscientific contribu-tions. A DSL and a temporal model were proposed to formalize a care plan. This model is then used to automatically verify a care plan using a timed automaton approach. Various investiga-tions were carried out on the planning of visits. Some of these contributionshavebeentakenupbydifferentresearchteamstobe improvedortoserveasabasisforfurtherinvestigations.The pro-posalswere testedinrealconditionsandwelcomedbytheusers. Theycanbe usedassupportfortherealizationofsoftware com-ponentsthatcanbeintegratedintocommercializedsystems.
Humanandanimalrights
The authorsdeclare that thework described hasbeen carried out in accordance withthe Declaration ofHelsinki ofthe World MedicalAssociationrevisedin2013forexperimentsinvolving hu-mansaswell asinaccordancewiththe EUDirective 2010/63/EU foranimalexperiments.
Informedconsentandpatientdetails
Theauthors declarethatthisreport doesnot containany per-sonal informationthat could lead tothe identificationofthe pa-tient(s).
Theauthorsdeclarethat theyobtainedawritteninformedcon sent from the patients and/or volunteers included in the article. Theauthors alsoconfirmthatthe personaldetails ofthepatients and/orvolunteershavebeenremoved.
Disclosureofinterest
Theauthorsdeclarethattheyhavenoknowncompeting finan-cialorpersonal relationships thatcould be viewedasinfluencing theworkreportedinthispaper.
Funding
Thisworkhasbeensupported by:TheFrenchNationalAgency for Research(ANR), within the TecSanframework andsupported bytheCancerBioSantécluster.
Authorcontributions
AllauthorsattestthattheymeetthecurrentInternational Com-mitteeofMedicalJournalEditors(ICMJE)criteriaforAuthorship.
Acknowledgements
Theworkpresentedherehasbeendevelopedintheframework ofprojectPlas’O’Soins,anationwideprojectfundedbytheFrench NationalAgencyforResearch(ANR),withintheTecSanframework (ANR-2010-TECS-016-08) andsupported by the Cancer BioSanté cluster. Theauthors wouldliketothankthe end-userpartners of Plas’O’Soinsconsortium:AlbiHospital,UMT,andCARMISud-Ouest for providing insight and expertise that greatly assisted the re-search andforallowingthemtoexperimentthePlas’O’Soins plat-form in real situation. The authors would also like to thank the industrial partners:Almerys andCGx Systems fortheir contribu-tioninspecifyinganddevelopingphasesofPlas’O’Soinsplatform.
References
[1]Lamine E,Tawil ARH,Bastide R,Pingaud H.Anontology-drivenapproachfor themanagementofhomehealthcareprocess.In:EnterpriseinteroperabilityVI. Cham:Springer;2014.p. 151–61.
[2]Lamine E,Tawil ARH,Bastide R,Pingaud H.Ontology-basedworkflowdesign forthecoordinationofhomecareinterventions.In:Workingconferenceon vir-tualenterprises.Springer;2014.p. 683–90.
[3]Mohammadzadeh N,Safdari R.Patientmonitoringinmobilehealth: opportu-nitiesandchallenges.MedArch2014;68:57.
[4]Darkins A,Ryan P,Kobb R,Foster L,Edmonson E,Wakefield B,etal.Care coor-dination/hometelehealth:thesystematicimplementationofhealth informat-ics,hometelehealth,anddiseasemanagementtosupportthecareofveteran patientswithchronicconditions.TelemedE-Health2008;14:1118–26. [5]Kamei T.Informationandcommunicationtechnologyforhomecareinthe
fu-ture.JpnJNursSci2013;10:154–61.
[6]Wang F,Turner KJ.Towardspersonalisedhomecaresystems.In:Proceedingsof the1stinternationalconferenceonPErvasivetechnologiesrelatedtoassistive environments.ACM;2008.p. 44.
[7]Bossen C, Christensen LR, Grönvall E, Vestergaard LS. Carecoor: augment-ing the coordination of cooperative home care work. Int J Med Inform 2013;82:e189–99.
[8]Paganelli F,Giuli D.Anontology-basedsystemforcontext-awareand config-urableservicestosupporthome-basedcontinuouscare.IEEETransInfTechnol Biomed2011;15:324–33.
[9]Lasierra N,Alesanco A,Guillén S,García J.Athreestageontology-driven solu-tiontoprovidepersonalizedcaretochronicpatientsathome.JBiomedInform 2013;46:516–29.
[10]Koutkias VG,Chouvarda I,Maglaveras N.Amultiagentsystemenhancing home-carehealthservicesforchronicdiseasemanagement.IEEETransInfTechnol Biomed2005;9:528–37.
[11]Isern D,Moreno A,Sánchez D,Hajnal Á,Pedone G,Varga LZ.Agent-based exe-cutionofpersonalisedhomecaretreatments.ApplIntell2011;34:155–80. [12]Bricon-Souf N,Anceaux F,Bennani N,Dufresne E,Watbled L.Adistributed
co-ordinationplatformforhomecare:analysis,frameworkandprototype.IntJ MedInform2005;74:809–25.
[13]Lamine E,Zefouni S,Bastide R,Pingaud H.Asystemarchitecturesupporting theagilecoordinationofhomecareservices.In:Collaborativenetworksfora sustainableworld;2010.p. 227–34.
[14] Next Step inCare –A Programm ofUnited Hospital Fund.A family care-giver’s planner for care at home. http://www.nextstepincare.org/Caregiver_ Home/Care_Planner/,2008.
[15]Fédérationnationaledesétablissementd’hospitalisationàdomicile.Livreblanc dessystèmesd’informationenhospitalisationàdomicile.1stedition.FNEHAD; 2009.
[16]Monsen K,Foster D,Gomez T,Poulsen J,Mast J,Westra B,etal. Evidence-basedstandardizedcareplansfor useinternationallytoimprove homecare practiceandpopulationhealth.In:Appliedclinicalinformatics–Schattauer; 2011.p. 373–80.
[17]Riaño D,Real F,Campana F,Ercolani S,Annicchiarico R.Anontologyforthe careoftheelderathome.In:Proceedingsofthe12thconferenceonartificial intelligenceinmedicine:artificialintelligenceinmedicine.Berlin,Heidelberg: Springer-Verlag;2009.p. 235–9.
[18] Hägglund M,Chen R,Koch S.ModelingsharedcareplansusingCONTsysand openHRtosupportsharedhomecareoftheelderly.JAmMedInformAssoc 2011;18:66–9.https://doi.org/10.1136/jamia.2009.000216.
[19] Hindle T, Hindle A, Spollen M. Resource allocation modelling for home-based health and social care services in areas having differential popula-tiondensitylevels:acasestudyinNorthernIreland.HealthServManagRes 2000;13:164–9.https://doi.org/10.1177/095148480001300304.
[20] Hindle T,Hindle G,Spollen M.Travel-relatedcostsofpopulationdispersionin theprovisionofdomiciliarycare totheelderly:acasestudyinEnglish lo-calauthorities.HealthServManagRes2009;22:27–32.https://doi.org/10.1258/ hsmr.2008.008012.
[21] Ernst AT,Jiang H,Krishnamoorthy M,Owens B,Sier D.Anannotated bibliog-raphyofpersonnelschedulingandrostering.AnnOperRes2004;127:21–144. https://doi.org/10.1023/B:ANOR.0000019087.46656.e2.
[22] Rinder M,Weckman G,Schwerha D,Snow A,Dreher P,Park N,etal.Healthcare schedulingbydatamining:literaturereviewandfuturedirections.JHealthc Eng2012;3:477–502.https://doi.org/10.1260/2040-2295.3.3.477.
[23]Moyaux T,Chaib-draa B,D’Amours S.Satisfactiondistribuéedeconstrainteset sonapplicationalagénérationd’unemploidutempsd’employés.In:Actesdu 5econgrèsinternationaldegénieindustriel;2003.
[24]Burke E,Cowling P,DeCausmaecker P,Berghe GV.Amemeticapproachtothe nurserosteringproblem.ApplIntell2001;15:199–214.
[25] Meisels A, Schaerf A. Modelling and solving employee timetabling prob-lems. Ann Math Artif Intell 2003;39:41–59. https://doi.org/10.1023/A: 1024460714760.
[26] Beddoe,G.Petrovic,S.Determiningfeatureweightsusingageneticalgorithm inacase-basedreasoningapproachtopersonnelrostering,2004.
[27]Chen JG,Yeung TW.Hybridexpert-systemapproachtonursescheduling. Com-putNurs1993;11:183–90.
[28]Yeung TW-K.Hybridexpertsystemapproachtonursescheduling.Universityof Houston;1991.
[29]Bachouch RB.Pilotageopérationneldesstructuresd’hospitalisationàdomicile. Ph.D.thesis,INSAdeLyon;2010.
[30] Akjiratikarl C,Yenradee P,Drake PR.PSO-basedalgorithmforhomecareworker scheduling inthe UK. Comput Ind Eng 2007;53:559–83. https://doi.org/10. 1016/j.cie.2007.06.002.
[31] Vidal T,Crainic TG,Gendreau M,Prins C.Ahybridgeneticalgorithmwith adap-tivediversitymanagementforalargeclassofvehicleroutingproblemswith time-windows. Comput Oper Res 2013;40:475–89. https://doi.org/10.1016/j. cor.2012.07.018.
[32] Favaretto D,Moretti E,Pellegrini P.AntcolonysystemforaVRPwithmultiple timewindowsandmultiplevisits.JInterdiscipMath2007;10:263–84.https:// doi.org/10.1080/09720502.2007.10700491.
[33] Bachouch RB,Guinet A,Hajri-Gabouj S.Adecision-makingtoolforhomehealth carenurses’planning.SupplyChainForumIntJ2011;12:14–20.https://doi.org/ 10.1080/16258312.2011.11517250.
[34] Gayraud F,Deroussi L,Grangeon N,Norre S.Anewmathematicalformulation forthehomehealthcareproblem.ProcTechnol2013;9:1041–7.https://doi.org/ 10.1016/j.protcy.2013.12.116.
[35] Mankowska DS, Meisel F, Bierwirth C. The home health care routing and scheduling problem with interdependent services. Health Care Manage Sci 2014;17:15–30.https://doi.org/10.1007/s10729-013-9243-1.
[36] MayaDuque PA,Castro M,Sörensen K,Goos P.Homecareserviceplanning. ThecaseofLandelijkeThuiszorg. EurJOperRes2015;243:292–301.https:// doi.org/10.1016/j.ejor.2014.11.008.
[37] Braekers K,Hartl RF,Parragh SN,Tricoire F.Abi-objectivehomecare schedul-ingproblem:analyzingthetrade-offbetweencostsandclientinconvenience. EurJOperRes2016;248:428–43.https://doi.org/10.1016/j.ejor.2015.07.028. [38] Fikar C,Hirsch P.Homehealthcareroutingandscheduling:areview.Comput
OperRes2017;77:86–95.https://doi.org/10.1016/j.cor.2016.07.019.
[39]Bajorek M,Nowak J.Theroleofamobiledeviceinahomemonitoring health-caresystem.In:2011federatedconferenceoncomputerscienceand informa-tionsystems(FedCSIS).IEEE;2011.p. 371–4.
[40]Ventola CL. Mobiledevicesandappsforhealthcareprofessionals:usesand benefits.PharmTher2014;39:356.
[41]Gani K, Bouet M,Schneider M,Toumani F.Formalmodelingandanalysisof homecareplans.In:12thInternationalconferenceonserviceoriented com-puting(ICSOC2014);2014.
[42]Bouet M,Gani K,Schneider M,Toumani F.Ageneralmodelforspecifyingnear periodicrecurrentactivities-applicationtohomecareactivities.In:2013IEEE 15thinternationalconferenceonE-healthnetworking,applications&services (Healthcom).IEEE;2013.p. 207–11.
[43]Alur R,Dill DL.Atheoryoftimedautomata.TheorComputSci1994:183–235. [44]Cassez F,Roux O-H.StructuraltranslationfromtimePetri netstotimed
au-tomata.ElectronNotesTheorComputScience2005;128(6):145–60.
[45]Gani K.Usingtimedautomataformalismformodelingandanalyzing home careplans.Ph.D.thesis,UniversiteBlaisePascalClermont-FerrandII;2015. [46]Yannakakis M,Lee D.Anefficientalgorithmforminimizingreal-timetransition
systems.In:Proceedingsofthe5thinternationalconferenceoncomputeraided verification.London,UK:Springer-Verlag;1993.p. 210–24.
[47]Gourc D,Marmier F,Gaborit P.Anapproachbasedontabusearchtechniquefor solvingamultitimewindowhomehealthcareschedulingproblem.In:MOSIM 2014,10èmeconférencefrancophonedemodélisation,optimisationet simula-tion;2014.
[48]Barkaoui K,Hicheur A,Kheldoun A,Liu D.Modellingandanalyzinghomecare plansusinghigh-levelPetri nets.In:201613thinternationalworkshopon Dis-creteeventsystems(WODES).IEEE;2016.p. 284–90.
[49] Belhaiza S,Hansen P,Laporte G.Ahybridvariableneighborhoodtabusearch heuristicforthevehicleroutingproblemwithmultipletimewindows.Comput OperRes2014;52:269–81.https://doi.org/10.1016/j.cor.2013.08.010.
[50] Beheshti AK,Hejazi SR,Alinaghian M.Thevehicleroutingproblemwith multi-pleprioritizedtimewindows:acasestudy.ComputIndEng2015;90:402–13. https://doi.org/10.1016/j.cie.2015.10.005.
[51] Bowers J, Cheyne H, Mould G, Page M. Continuity of care in community midwifery.HealthCareManageSci2015;18:195–204.https://doi.org/10.1007/ s10729-014-9285-z.
[52] Milburn AB,Spicer J.Multi-objectivehomehealthnurseroutingwithremote monitoring devices.Int JPlanSched2013;1:242–63. https://doi.org/10.1504/ IJPS.2013.059677.
[53] En-nahli L, Afifi S, Allaoui H,Nouaouri I.Localsearch analysisfor a vehi-cle routing problemwith synchronizationandtime windowsconstraintsin homehealthcareservices.IFAC-PapersOnLine2016;49:1210–5.https://doi.org/ 10.1016/j.ifacol.2016.07.674.
[54]Burke E, De Causmaecker P, Petrovic S, Berghe GV. Variable neighborhood search for nurserosteringproblems.In: Metaheuristics:computer decision-making,appliedoptimization.Boston,MA:Springer;2003.p. 153–72. [55]Bouet M,Schneider M.ANoSQL-basedframeworkformanaginghomeservices.