Science Arts & Métiers (SAM)
is an open access repository that collects the work of Arts et Métiers Institute of
Technology researchers and makes it freely available over the web where possible.
This is an author-deposited version published in:
https://sam.ensam.eu
Handle ID: .
http://hdl.handle.net/10985/20231
To cite this version :
Yann-Philippe CHARLES, Sylvain PERSOHN, Philippe ROUCH, Jean-Paul STEIB, E.A.
SAULEAU, Wafa SKALLI - The effect of posterior non-fusion instrumentation on segmental shear
loading of the lumbar spine - Orthopaedics and Traumatology - Surgery and Research - Vol. 100,
n°5, p.461-467 - 2014
Any correspondence concerning this service should be sent to the repository
Available
online
at
ScienceDirect
www.sciencedirect.com
Original
article
The
effect
of
posterior
non-fusion
instrumentation
on
segmental
shear
loading
of
the
lumbar
spine
Y.P.
Charles
a,b,∗,
S.
Persohn
a,
P.
Rouch
a,
J.-P.
Steib
b,
E.A.
Sauleau
c,
W.
Skalli
aaLaboratoiredeBiomécanique,ArtsetMétiersParisTech,151,boulevarddel’Hôpital,75013Paris,France
bServicedeChirurgieduRachis,HôpitauxUniversitairesdeStrasbourg,FédérationdeMédecineTranslationnelle(FMTS),1,placedel’Hôpital,BP426,
67091StrasbourgCedex,France
cDépartementdeSantéPublique,HôpitauxUniversitairesdeStrasbourg,FédérationdeMédecineTranslationnelle(FMTS),1,placedel’Hôpital,BP426,
67091StrasbourgCedex,France
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Accepted27May2014 Keywords: Degenerativespondylolisthesis Facetectomy Undercuttinglaminectomy Non-fusioninstrumentation Anteriorsheara
b
s
t
r
a
c
t
Background:Lumbarstenosisandfacetosteoarthritisrepresentindicationsfordecompressionand instru-mentation.ItisunclearifdegenerativespondylolisthesisgradeIwitharemainingdischeightcouldbean indicationfornon-fusioninstrumentation.Thepurposeofthisstudywastodeterminetheinfluenceofa mobilepediclescrewbaseddeviceonlumbarsegmentalshearloading,thussimulatingtheconditionof spondylolisthesis.
Materialsandmethods:Sixhumancadaverspecimensweretestedin3configurations:intactL4–L5 seg-ment,thenfacetectomyplusundercuttinglaminectomy,theninstrumentationwithlesion.Astaticaxial compressionof400NwasappliedtothelumbarsegmentandanteriordisplacementsofL4onL5were measuredforposterior-anteriorshearforcesfrom0to200N.Theslopeoftheloadingcurvewasassessed todetermineshearstiffness.
Results:Homogenousload-displacementcurveswereobtainedforallspecimens.Theaverageintact ante-riordisplacementwas1.2mm.Afterlesion,thedisplacementincreasedby0.6mmcomparedtointact (P=0.032).Theinstrumentationdecreasedthedisplacementby0.5mmcomparedtolesion(P=0.046). Thestiffness’swere:162N/mmforintact,106N/mmforlesion,148N/mmforinstrumentation.The differencewasnotsignificantbetweeninstrumentedandintactsegments(P=0.591).
Conclusions: Facetectomy plusundercutting laminectomy decreases segmental shear stiffnessand increasesanteriortranslationalL4–L5displacement.Shearstiffnessoftheinstrumentedsegmentishigher withthedeviceandanteriordisplacementsundershearloadingaresimilartotheintactspine.This con-ditioncouldtheoreticallybeinterestingforthesimulationofnon-fusioninstrumentationindegenerative spondylolisthesis.
©2014ElsevierMassonSAS.Allrightsreserved.
1. Introduction
Lumbar non-fusion instrumentation systems are aimed to reduce theriskof adjacentsegment degenerationsecondary to fusion [1]. Total disc replacement can be efficiently indicated in low-backpain caused bydiscopathy. Nevertheless, the load-sharingcomplexbetweenthediscand facetjointsmaylead to recidivatingpainifadditionalmoderatefacetdegenerationisnot diagnosed preoperatively [2]. This has spawned an interest in
∗ Correspondingauthorat:LaboratoiredeBiomécanique,ArtsetMétiers Paris-Tech,151,boulevarddel’Hôpital,75013Paris,France.Tel.:+33388116826; fax:+33388115233.
E-mailaddress:yann.philippe.charles@chru-strasbourg.fr(Y.P.Charles).
the development of posterior facet preserving non-fusion sys-tems,whichmaydecreasesegmentalmotionwithoutsuppressing it [3–5]. Facet resurfacing and replacement devices have been designed toaddress severe facetosteoarthritis and subsequent stenosis[6].
Instrumentationisrequiredafterfacetectomyorarthrectomy becauseofsegmentalincreaseofmotioninaxialrotationandunder shearloading[7,8].Invitrostudiesandfiniteelementmodels indi-cate that posterior non-fusiondevices could stabilizea lumbar segmentandmaintainmobilityafterpartialortotalfacetresection andlaminectomy[9–12].Firstclinicaltrialsshowedthat decom-pressionandnon-fusioninstrumentationmightimproveback-and leg-pain, and thequalityoflife indegenerative spondylolisthe-sis [13–15]. However,these devices are restricted to segments witha sufficient discheight,and it isnot cleartowhat extent http://dx.doi.org/10.1016/j.otsr.2014.05.005
462 Y.P.Charlesetal./Orthopaedics&Traumatology:Surgery&Research100(2014)461–467
Fig.1.Non-fusioninstrumentationwithpolyaxialconnectorlinkingtherodsto caudalscrews,thusallowingathree-dimensionalmovementandstabilizationafter medialfacetresection.
decompressionshouldbeperformed,sinceshearforcesare trans-mitted through the implant, which may lead to device-related complications[16].
The NeoFacetTM (Clariance, Dainville, France) represents an
implant,whichisdesignedforposteriorelementsupplementation ifafacetresectionisrequiredinadditiontoundercutting laminec-tomy.Itmightbeindicatedforlow-backpain,mainlyduetofacet osteoarthritis,andsciaticaduetolateralrecessand/orforaminal stenosis.Thissystemutilizesfourpediclescrewswithtwo angu-latedrodsfixedcranially.Thisimplantismadeofimplantablegrade metalcomponents,whichaddresstheanatomicalrequirementsof thesegmentsL3–L4andL4–L5.Traditionalpediclescrewfixation isused.Tworods(30◦ or45◦)areinsertedandfixedatthe
cra-nialvertebrausingpolyaxialpediclescrews.Theserodsarelinked tocaudalpediclescrewsusingapolyaxialconnectoroneachside, whichallowsmovementsinflexion-extension,lateralbendingand axialrotation.Across-linkconnectsbothrodstoeachother,thus avoidingexcessiveaxialrotation(Fig.1).Pediclescrewsare man-ufacturedof titaniumalloy.A titaniumplasma spraycoating is
appliedtotheboneinterfacesurfacesofthescrews.Theother com-ponentsoftheimplantaremanufacturedfroma wear-resistant cobalt-chromium-molybdenumalloy.
Apreviousinvitrostudydemonstratedthatthisdevicecould preserveflexibilitybetweenlumbar vertebraewhile restraining motioninaxialrotationafterfacetectomy[17].Itisalsoimportant toinvestigatetheshearbehaviorofthisimplant,whichmaybe indicatedindegenerativespondylolisthesisgradeIwitha remain-ingdischeight.Thepurposeofthisstudywastodeterminethe influence of non-fusion instrumentation on a lumbar segment undershearloading,thussimulatingtheconditionsof degener-ativespondylolisthesistreatedbyfacetectomyplusundercutting laminectomy.
2. Materialsandmethods
Sixfresh-frozenhumancadavericL4–L5spinesegmentswere tested.Theaverageageofthedonorswas73.8yearsandranged from63to84years.Therewere5malesand1female.The speci-menswerefreshlydissected,sealedindoubleplasticbags,frozen, andstoredat−20◦Cuntiltesting.Thespecimenswerethawedto
6◦C12to14hoursbeforestartingthepreparationprocess.Soft
tis-sueswereremoved,leavingallligaments,jointcapsules,discsand bonystructuresintact.Spinaldeformities,damageorsevere degen-erationofthediscsandfacetjointswereexcludedmacroscopically andradiographically.Mediandischeightswere≥7mmonlateral radiographs.Theexperimentwasperformedatroomtemperature, whileusingasalinesolution(NaCl0.9%)tomoisturethedisc.
ThecranialhalfoftheL4vertebralbodyandthecaudalhalfof theL5vertebralbodywereembeddedin2metalcontainersusing polymethylmetacrylatecement(Technovit3040;Haerus,Hanau, Germany).ThemedianplaneoftheL4–L5discwasalignedwith ananteriorinclinationof10◦withregardtothehorizontalplane,
thusreproducingitssagittalalignmentinvivo.Biplaneradiographs wereusedtochecktheorientationofthespecimen.Shear load-ingtestswereconductedinaspecificspine-testingdevicethatwas designedforthispurpose.Thecaudalcontainer,fixedonL5,was rigidlyscrewedtoatable,whilethecranialcontainer,fixedonL4, wasmountedtoarail,allowingtranslationinthesagittalplane. Acompressivepreloadof400Nwasappliedtothemotion seg-ment[10,11,18,19].LoadswereappliedtoL4usingdeadweights placedattheendofloadingbars,cablesandpulleys,thus induc-ingananteriortranslationofL4onL5(Figs.2and3).Thissystem
Fig.2.ExperimentalsetupforinvitrosheartestingoftheL4–L5segment,withamobilerailfixedtoL4,alineartransducerformeasurementsoftranslationofL4onL5 obtainedbyanteriortractionviaacableandpulleysystemattachedtotherail.
Fig.3. InstrumentedL4–L5specimeninthespine-testingdevice.
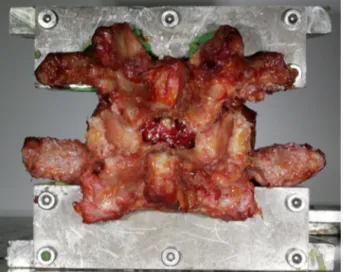
Fig.4.LesionappliedtoL4–L5bymedialfacetectomyplusundercutting laminec-tomy.
allowedapplyingquasi-staticforcesinstepsof10N,withan inter-valof15secondsbetweeneachstep,untilamaximumof200N wasreached.Themaximalanteriordisplacementandbackto neu-tralpositionwerecompletedduringthesameloading-unloading cycle.Threepreconditioningcycleswereappliedtothespecimen usingthesameloadingprotocol,beforethemeasurementcycle wasstarted.Displacementsweremeasuredattheleveloftherail usingalineartransducer(VishaySfernice50L4D202W00235D 2k;VishayElectronicGmbH,Selb,Germany).Themeasurement accuracyofthis systemwasestimatedat0.1mmfor linear dis-placements.Load-displacementcurveswereobtainedforloading andunloadingcycles.Thestiffnesswascalculatedconsideringthe slopeofthelinearpartoftheloadingcurve.
Thespecimens weretestedin 3configurations:intact speci-men,specimenwithlesion,instrumentedspecimenwithlesion. ThelesionconsistedofanL4–L5medialfacetectomybyremoving theinferiorL4articularprocesses.Aninterlaminarfenestrationand yellowligamentresectionattherecessuswereperformedusinga Kerissonrongeur,thussimulatinganundercuttinglaminectomy (Fig.4).Theimplantwaspositionedsymmetricallybetweenright andleftsides.Pediclescrews,witha6.5mmdiameteranda45mm length,wereplacedparalleltothesuperiorendplateandalonga convergent trajectoryinthehorizontalvertebralplane.Therod systemandthepolyaxialconnectorsweremountedtoL4andL5 screws,respectively.Bothrodswereconnectedbyarigid cross-link.Thepositionoftheimplantwasdocumentedusingbiplane radiographs(Fig.5).
Fig.5.Antero-posteriorandlateralradiographsofinstrumentedL4–L5segment withlesionandvertebralbodiesembeddedinPolyMethylMethAcrylate(PMMA).
Statistical evaluation was performed with R Software Ver-sion 2011 (R Foundation for Statistical Computing, Vienna, Austria).Afterchecking homogeneityof variancesusing a non-parametricFligner-Killeentest,theWilcoxonranktestwasusedfor pairedsamplestocomparemaximaldisplacementsandstiffness’s betweendifferentconfigurations.Unilateraltestsfor superiority wereused.Thesignificancelevelwassetat0.05foralltests.
3. Results 3.1. Displacement
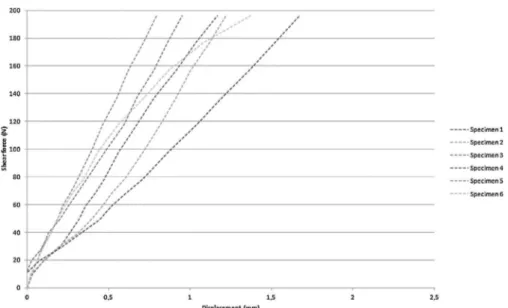
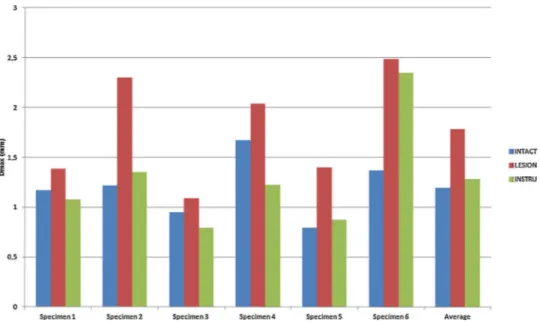
Load-displacement curves were obtained for anterior trans-lation and back to neutral position. A hysteresis phenomenon was observedfor each configurationsince the unloadingcurve wasnotsuperimposedontheloadingcurve.Loadingcurveswere comparable for the six intactspecimens (Fig.6).The variances werehomogenousformaximaldisplacements(P=0.194).Table1 demonstrates average,median andextremevalues obtainedfor each configuration.Fig. 7representsaverageload-displacement curvesandFig.8showsindividualvaluesobtainedforeach spec-imen.Thelesionledtoanaverageincreaseof0.6mmcompared totheintactL4–L5segment(P=0.032).Theinstrumentedsegment withlesionincreasedtheaveragedisplacementby0.1mm com-paredtotheintactspine(P=0.468).Theinstrumentationdecreased theaveragedisplacementby0.5mmcomparedtothelesionalone (P=0.046).
464 Y.P.Charlesetal./Orthopaedics&Traumatology:Surgery&Research100(2014)461–467
Fig.6.Load-displacementcurvesduringloadingfrom0Nto200Nforeachspecimen.
Table1
Maximalanteriordisplacement(mm)at200N.
Configuration Average Median Minimum Maximum Differencewithintact P-valuea
Intact 1.2 1.2 0.8 1.7 – –
Lesion 1.8 1.7 1.1 2.5 +0.6[+49%] 0.032
Instrumented 1.3 1.2 0.8 2.4 +0.1[+6%] 0.468
aWilcoxontestsignificantifP<0.05.
3.2. Stiffness
Thevarianceswerehomogenousforstiffness’s(P=0.717). Val-uesforeachconfigurationaredemonstratedinTable2.Thelesion decreased the stiffness by 56N/mm on average compared to theintactL4–L5segment(P=0.032).Thedifferencebetweenthe instrumented and theintact segment was14N/mm(P=0.591). The average stiffness of the instrumented segment increased by 42N/mm compared to the lesion without instrumentation (P=0.046).
4. Discussion
Theindicationforposteriornon-fusiondeviceshasbeen empha-sizedin lateralrecessand/orforaminalstenosisassociatedwith osteoarthritis of thefacet joints. Thesurgical treatmentof this lumbardegenerativepathologyusuallyrequiresadecompression of thecanal,and anadditional partialorcomplete resectionof thefacetjointsifthesearemainlyresponsibleforbackpain.This impliesastabilizationusingaposteriorinstrumentationandfusion to avoid segmental hypermobility of the treated segment. The
Fig.8. Maximaldisplacements(Dmax)at200Nforeachspecimenandtheiraverageforthedifferentconfigurations.
rationale behindpediclescrewbased mobilesystemswould be thestabilizationof thelumbar segmentwhilepreservinga cer-tainamountofsegmentalmobility,andthuspreventingadjacent segmentdegeneration[18].Nevertheless,theprotectiveeffectof thesenon-fusiondevicesonadjacentlevelshasnotbeenclearly demonstratedtodate.Theinfluenceofthesedevicesonsegmental kinematicsofthelumbarspinemainlydependsontheimplant’s design:flexion-extensionandlateralbendingareusuallyslightly decreased,whereasaxialrotationisonlylimitedbysystemswith across-linkcomponent[9–12,20].However,thispropertyseems essentialforthestabilizationofthelumbarsegmentwhen perform-ingafacetectomy[7].Ontheotherhand,shearloadingincreases mobilityofthelumbarsegmentafterfacetresection[8,19],and posterior-anterior displacementsmay havean influence onthe implant’s function.Thiswouldbeclinically relevantif degener-ative spondylolisthesis grade Iwithan associated stenosis was consideredasanindicationforposteriornon-fusion instrumenta-tion.
Hasegawaetal.[20]investigatedlumbarsegmental hypermo-bilityinvivobyusingintra-operativebiomechanicaldatacompared topreoperativeradiologicalparameters.Openingofdegenerated facetjointsonaxialcomputedtomographyimagesand degenera-tivespondylolisthesiswerefoundtobethestrongestpredictors for an unstable segment. Furthermore, thePfirrmann grade of degenerated discs onmagnetic resonance imaging was investi-gated.Segmentswithgrades3and4,whichcorrespondtomild andmoderatediscdegeneration,weremorepronetobeing hyper-mobilethanthosewithagrade5.Theconceptofposteriormobile instrumentation couldbeinteresting for patientswithstenosis and moderatediscopathy, presenting theserisk factorsfor seg-mentalhypermobility.Wethereforefocusedonaninvitromodel
analyzinganteriorshearstress,whichmightreproducethe clini-calindicationofdegenerativespondylolisthesiswithmoderatedisc degeneration,treatedbyposteriordecompressionandnon-fusion instrumentation.
Bothinvitroand finiteelementstudieshave shownthatthe shear stiffness of a lumbar segment is reduced after posterior decompressiontechniques[8,19,21,22].vanSolingeetal.[21]used aporcinemodelofthelumbarspinetodemonstratethat laminec-tomy and partial facetectomy resulted in a decrease of shear stiffnessof9%atapreloadof1600N.Bisshopetal.[22]useda simi-lartestingprotocolforhumancadavericL2–L3andL4–L5segments, andshowedthatshearstiffnesswasdecreasedafterlaminectomy comparedtotheintactspineinmilddiscdegenerationbasedonthe Pfirrmanngrade.Incontrasttothat,severedegenerationappeared toenhanceshearstiffnessratherthanreducingit.Moreover,the amountofpreloadneedstobeconsideredsinceaxial compres-sioninfluencesthestiffness,thehysteresisareaandthelinearityof theload-displacementrelationshipofthelumbarmotionsegments [23].Luetal.[19]analyzedtheinfluenceofposteriorversus ante-riorelementresectiononshearstiffnessofhumanlumbarmotion segments.Thecompleteremovaloffacetjointsandposterior lig-aments ledtoanaveragedecrease ofstiffnessinanteriorshear of 77.7%comparedtoanintactspine.Aftercompletesectionof thediscincludinganteriorandposteriorlongitudinalligaments, anteriorshearstiffness decreasedby22.8%onaverage. Further-more,theresectionofposteriorelementsapproximatelydoubled anteriordisplacements(+117%)whenthespecimenswereloaded to250N.Theseresultsstresstheimportanceofthefacetjoints, thesupraspinous,interspinousandyellowligamentsforshear sta-bility. Nevertheless,anterior and posterior elementsdo not act independentlyofoneanotherinresistinganteriorshear,butthe
Table2
Stiffnessduringposterior-anteriorloading(N/mm).
Configuration Average Median Minimum Maximum Differencewithintact P-valuea
Intact 162 164 112 242 – –
Lesion 106 113 81 172 −56[−34%] 0.032
Instrumented 148 165 81 240 −14[−8%] 0.591
466 Y.P.Charlesetal./Orthopaedics&Traumatology:Surgery&Research100(2014)461–467 intervertebralsegment is rather a composite structure withits
differentcomponentsfunctioningincooperation, whichare fur-therguidedbysurroundingmusclesinvivo.Thefindingsin our studyareinlinewiththepreviouslymentionedresults,showing reducedshearstrengthandstiffnessofthespineafterrealizinga medialfacetectomyincombinationwithanundercutting laminec-tomy.Theconfigurationofamoderatediscopathyleadingtolower shearstiffnessinvitrohasconsequencesfortheinstrumentation ofahypermobilesegmentinvivo.Thiswouldreflecttheclinical indicationofadegenerativespondylolisthesiswithadisc degen-erationgradePfirrmann3or4,facetosteoarthritis,lateralrecess and/orforaminalstenosis,whichwouldbecarriedoutforposterior non-fusioninstrumentation.
Theinfluenceofnon-fusioninstrumentationsonshearstress isnotwellunderstoodtodateandithasneverbeenanalyzedfor posteriormobiledevicestoourknowledge,althoughload trans-missioninposterior-anteriordirectionandaxialrotationappears crucialfor theirfunction.Schillinget al.[24]haveanalyzedthe effectofdesignparametersofposteriordynamicstabilization sys-temsanddemonstratedacorrelationbetweenaxialstiffnessand inter-segmentalmotionrestrictioninthesagittalplane,butnotin thetransversal plane.Thismaybeduetothefactthatdynamic stabilizationsystemsarenotprovided witha cross-linkin con-trasttothemobilesysteminourstudy.Furthermore,theseauthors showedthatthespecificdesigndictatedtheimplantsshear prop-erties.Implantsusingaspacerlockedintoplacebyacordbetween thescrewshadalowershearresistancethanthoseusingaspring mechanismrestricting translationalmovements.The implantin thepresent studyrestrictedanteriorsheardisplacementsofthe lumbarsegmenttreatedbymedialfacetectomyandundercutting laminectomy.Thisindicated thatthepolyaxial connectormight allowmovementsinflexion-extension,lateralbendingandaxial rotation,butthatitalsolimitstheeffectofanteriorshearstress. Furthermore,thepropertiesoftheroditselfareimportantforthe loadtransfercharacteristicsbetweentheimplantandthelumbar spine.Melnyketal.[25]investigatedtheinfluenceofrod mate-rialandgeometryonshearstiffnessupto250N(under300Naxial compression)inhumanlumbarsegmentsthathadbeentreated invitrobypartialfacetresection,undercuttinglaminectomyand nucleotomy.Theimplantssupportedgreatershearforcesasthe specimenwasdestabilized.Lowershearloadsweretransferredto thespinewith5.5mmtitaniumrods(stiffestconfiguration) com-paredto6.35×7.2mmoblongPEEKrods(intermediatestiffness) and5.5mmroundPEEKrods(lowstiffness).Themeasuredanterior displacementswereinferiorto2mmandcomparabletotheresults oftheinstrumentspineinourstudyatsimilarloadingconditions. Therodsofthepresentnon-fusiondevicehavea5mmdiameter andaremadeofacobalt-chromium-molybdenumalloy,whichhas ahigherstiffnessthantitanium.
Althoughthetechnicalcharacteristicsoftheimplantare impor-tantforshearresistance,thesurgicalprocedureitselfalsoneedsto beadapted,thusprovidingacompleteneurologicaldecompression butthelowestpossibledestabilizationofthelumbarsegment.The undercuttingorcompletelaminectomyitselfdoesnotcreateand unstablesituationifthereisnoolisthesisofthetreatedsegment. Onlythecombinationwithafacetresection,requiredforfarlateral andforaminaldecompression,maynecessitatestabilizationbyan implant.
5. Conclusion
Thecombination of partialfacetresectionplusundercutting laminectomydecreasessegmentalshearstiffnessandincreasesthe anteriortranslationaldisplacementofL4onL5undershear load-ing.Theshearstiffnessoftheinstrumentedlumbarsegmenttends
toincreasewiththeposteriornon-fusiondeviceandanterior dis-placementtendstodecreaseundershearloading.Thiscondition couldtheoretically beinterestingforthesimulationofposterior non-fusioninstrumentationindegenerativespondylolisthesis. Disclosureofinterest
TheLBMArtsetMétiersParisTechreceivedinstitutionalsupport fromClariance.
Y.P.CharlesisconsultantforClariance. J.-P.SteibisaboardmemberofClariance. Acknowledgements
Clariancefortechnicalsupport. References
[1]ShonoY,KanedaK,AbumiK,McAfeePC,CunninghamBW.Stabilityof poste-riorspinalinstrumentationanditseffectsonadjacentmotionsegmentsinthe lumbosacralspine.Spine1998;23:1550–8.
[2]SiepeCJ,MayerHM,Heinz-LeisenheimerM,KorgeA.Totallumbardisc replace-ment:differentresultsfordifferentlevels.Spine2007;32:782–90.
[3]SchnakeKJ,SchaerenS,JeanneretB. Dynamicstabilization inadditionto decompressionforlumbarspinalstenosiswithdegenerativespondylolisthesis. Spine2006;31:442–9.
[4]PanjabiMM,HendersonG,JamesY,TimmJP.StabilimaxNZ®
versussimulated fusion:evaluationofadjacentleveleffects.EurSpineJ2007;16:2159–65. [5]Schmoelz W, Erhart S,Unger S,Disch AC. Biomechanical evaluation of
aposterior non-fusioninstrumentation ofthelumbar spine.EurSpine J 2012;21:939–45.
[6]Büttner-Janz K. Status quo of facet joint replacement. Orthopade 2010;39:609–22.
[7]AbumiK,PanjabiMM,KramerMM,DuranceauJ,OxlandT,CriscoJJ. Biome-chanicalevaluationoflumbarspinalstabilityaftergradedfacetectomy.Spine 1990;15:1142–7.
[8]TeoEC,LeeKK,QiuTX,NgHW,YangK.Thebiomechanicsoflumbargraded facetectomyunderanteriorshearload.IEEETransBiomechEng2004;51: 443–9.
[9]Wilke HJ, Schmidt H, Werner K, Schmölz W, Drumm J. Biomechanical evaluation of a new total posterior element replacementsystem. Spine 2006;31:2790–6.
[10]ZhuQ,LarsonCR,SjovoldSG,RoslerDM,KeynanO,WilsonDR,etal. Biome-chanicalevaluationoftheTotalFacetArthroplastySystem:3-dimensional kinematics.Spine2007;32:55–62.
[11]PhillipsFM,TzermiadianosMN,VoronovLI,HaveyRM,CarandangG, Ren-nerSM,etal.EffectsoftheTotalFacetArthroplastySystemaftercomplete laminectomy-facetectomyonthebiomechanicsofimplantedandadjacent seg-ments.SpineJ2009;9:96–102.
[12]GoelVK,MehtaA,JangraJ,FaizanA,KiapourA,HoyRW,etal.Anatomic FacetReplacementSystem(AFRS)restorationoflumbarsegment mechan-icstointact:afiniteelementstudyandinvitrocadaverinvestigation.SASJ 2007;1:46–54.
[13]McAfeePC,KhooLT,PimentaL,CapuccinoA,SengozA,CoricD,etal.Treatment oflumbarspinalstenosiswithatotalposteriorarthroplastyprosthesis:implant description,surgicaltechnique,andaprospectivereporton29patients. Neu-rosurgFocus2007;22:E13.
[14]Castellvi A. The treatment of symptomatic lumbar spinal stenosis with ACADIATM.Clinicaloutcomesfromworldwidecohort.In:NorthAmericanSpine
SocietyPre-MeetingCourse.2009.
[15]ReganJJ,HartjenCA,DryerRF,DiRisioDJ.ACADIATMfacetarthroplastypilot
study:twelvemonthsfollow-upresultsfor20patientsatfourcenters.In:Spine ArthroplastySocietyAnnualGlobalSymposium.2009.
[16]PalmerDK,InceogluS,ChengWK.Stemfractureaftertotalfacetreplacement inthelumbarspine:areportoftwocasesandreviewoftheliterature.SpineJ 2011;11:e15–9.
[17]CharlesYP,PersohnS,SteibJP,MazelC,SkalliW.Influenceofanauxiliaryfacet systemonlumbarspinebiomechanics.Spine2011;36:690–9.
[18]SerhanHA,VarnavsG,DoorisAP,PatwardhanA,TzermiadianosM. Biomechan-icsoftheposteriorlumbararticulatingelements.NeurosurgFocus2007;22:E1. [19]LuWW,LukKDK,HolmesAD,CheunKMC,LeongJCY.Pureshearpropertiesof lumbarspinaljointsandtheeffectoftissuesectioningonloadsharing.Spine 2005;30:E204–9.
[20]HasegawaK,ShimodaH,KitaharaK,SasakiK,HommaT.Whatarereliable radiologicalindicatorsoflumbarsegmentalinstability?JBoneJointSurgBr 2011;93:650–7.
[21]vanSolingeGB,vanderVeenAJ,vanDieënJH,KingmaI,vanRoyenBJ. Ante-riorshearstrengthoftheporcinelumbarspineafterlaminectomyandpartial facetectomy.EurSpineJ2010;19:2130–6.
[22]BisshopA,MullenderMG,KingmaI,JiyaTU,vanderVeenAJ,RoosJC,etal. Theimpactofbonemineraldensityanddiscdegenerationonshearand stiffnessofthelumbarspinefollowinglaminectomy.EurSpineJ2012;21: 530–6.
[23]Gardner-MorseMG,StokesIA.Structuralbehaviorofhumanlumbarspinal motionsegments.JBiomech2004;37:205–12.
[24]SchillingC,KrügerS,GruppTM,DudaTM,BlömerW,RohlmannA.Theeffectof designparametersofdynamicpediclescrewsystemsonkinematicsandload bearing:aninvitrostudy.EurSpineJ2011;20:297–307.
[25]MelnykAD,WenTL,KingwellS,ChakJD,SinghV,CriptonPA,etal.Loadtransfer characteristicsbetweenposteriorspinalimplantsandthelumbarspineunder anteriorshearloading:aninvitroinvestigation.Spine2012;37:E1126–33.
Powered by TCPDF (www.tcpdf.org) Powered by TCPDF (www.tcpdf.org) Powered by TCPDF (www.tcpdf.org) Powered by TCPDF (www.tcpdf.org) Powered by TCPDF (www.tcpdf.org) Powered by TCPDF (www.tcpdf.org) Powered by TCPDF (www.tcpdf.org) Powered by TCPDF (www.tcpdf.org)