© Pascale Marier-Deschênes, 2019
Codéveloppement d'outils d'information pour
promouvoir les échanges sur la sexualité en contexte de
réadaptation en traumatologie
Mémoire
Pascale Marier-Deschênes
Maîtrise en sciences cliniques et biomédicales - avec mémoire
Maître ès sciences (M. Sc.)
Codéveloppement d’outils d’information
pour promouvoir les échanges sur la sexualité
en contexte de réadaptation en traumatologie
Mémoire
Pascale Marier-Deschênes
Sous la direction de :
Marie-Eve Lamontagne, directrice de recherche
Marie-Pierre Gagnon, codirectrice de recherche
ii
Résumé
Entre le tiers et la moitié des personnes vivant avec un traumatisme craniocérébral (TCC) éprouveraient des difficultés de fonctionnement sexuel. Bien qu’il soit recommandé qu’une discussion portant sur la sexualité soit menée durant la réadaptation de ces personnes, la plupart des programmes québécois de réadaptation en traumatologie rapportent que cette pratique n’est pas implantée. De plus, il n’existe pas d’information vulgarisée et en français sur le sujet, qui pourrait être consultée par cette clientèle et utilisée par les professionnels de la réadaptation pour soutenir une discussion. Le but de ce projet était de codévelopper des outils d’information à l’intention des adultes ayant subi un TCC modéré ou grave (TCCMG) et leurs proches pour favoriser les échanges sur la sexualité en réadaptation. Deux séries de groupes de discussion et d’entrevues individuelles ont d’abord été menées. Les participants étaient a) des adultes ayant subi un TCCMG dans les cinq dernières années; b) des conjoints de personnes ayant un TCCMG. La première série d’entretiens visait à cibler le contenu et la forme du matériel à développer. Un prototype d’outil s’appuyant sur ces données a été créé, puis présenté aux mêmes participants lors d’un second entretien. Compte tenu des préférences identifiées et des difficultés liées à la lecture chez cette clientèle, la création d’une présentation narrée de type Prezi, abordant différents aspects de la sexualité, a été privilégiée. Les modifications et ajouts à apporter ont été ciblés. Cinq présentations narrées, un dépliant et une liste à cocher aidant l’individu à identifier ses préoccupations et à les partager ont finalement été développés. L’expérience de l’utilisateur liée à ces outils a ensuite été évaluée positivement auprès de six autres personnes ayant un TCCMG. L’implication des usagers dans le projet a permis la création de matériel dont le contenu et la forme sont adaptés à leurs besoins.
iii
Abstract
Individuals with traumatic brain injury (TBI) are more likely to deal with sexual dysfunctions, to engage in sexual activities less frequently and to report a diminished sexual quality-of-life and satisfaction than healthy adults. Accordingly, addressing potential sexual issues during the rehabilitation of these individuals is recommended. However, most Quebec trauma rehabilitation programs report that this practice is not implemented. In addition, no French information on the subject is sufficiently accessible in terms of form and content to be understood by clients and used by rehabilitation professionals to support a discussion. The goal of this project was to co-create informative resources with adults with moderate to severe TBI (MSTBI) and life partners to foster exchanges on sexuality in rehabilitation. Two rounds of consultations including focus groups and individual interviews were first conducted. Participants were (a) adults who sustained a MSTBI in the last five years; b) partners of persons with a MSTBI. Preferences for the resources’ content and form were explored during the first round of consultations. Participants identified several subjects to be covered and showed preference for audiovisual content over written information. A prototype of a narrated Prezi presentation was first developed based on participants’ priorities. During the second round of consultations, participants’ impressions of the prototype and needs for modifications were documented. Changes were made accordingly, and additional resources were created. The user experience was positively assessed with six other participants during a third round of consultations. This patient-oriented project led to the development of a sexuality information toolkit matching the interests and needs of adults with MSTBI.
iv
Table des matières
Résumé ... ii
Abstract ... iii
Table des matières ... iv
Liste des figures ... vii
Liste des tableaux ... viii
Liste des sigles ... ix
Remerciements ... xi
Avant-propos ... xii
Introduction ... 1
Prévalence et incidence du traumatisme craniocérébral ... 1
Répercussions du traumatisme craniocérébral ... 1
Objectifs et étapes du projet ... 4
Cadre théorique ... 5
Chapitre 1 - Talking about sexuality in the context of rehabilitation following traumatic brain injury: an integrative review of operational aspects ... 7
1.1 Résumé ... 7 1.2 Abstract ... 7 1.3 Introduction ... 8 1.4 Methods ... 9 Search strategy ... 9 Inclusion criteria ... 10 Exclusion criteria ... 10
Study selection and data extraction ... 10
Level of evidence and quality assessment ... 11
Data analysis ... 11
1.5 Results ... 11
Categories ... 14
1.6 Discussion ... 19
Prerequisites to discussing sexuality... 20
How to conduct the discussion ... 20
Who should lead the discussion ... 21
v
1.7 Limitations and future directions ... 21
1.8 Conclusion ... 22
1.9 Ackowledgments ... 23
1.10 References ... 23
Chapitre 2 – Creation of a post-TBI sexuality information toolkit: a patient-oriented project ... 27
2.1 Résumé ... 27
2.2 Abstract ... 27
2.3 Introduction ... 28
2.4 Method ... 29
2.4.1 Study design and methods ... 29
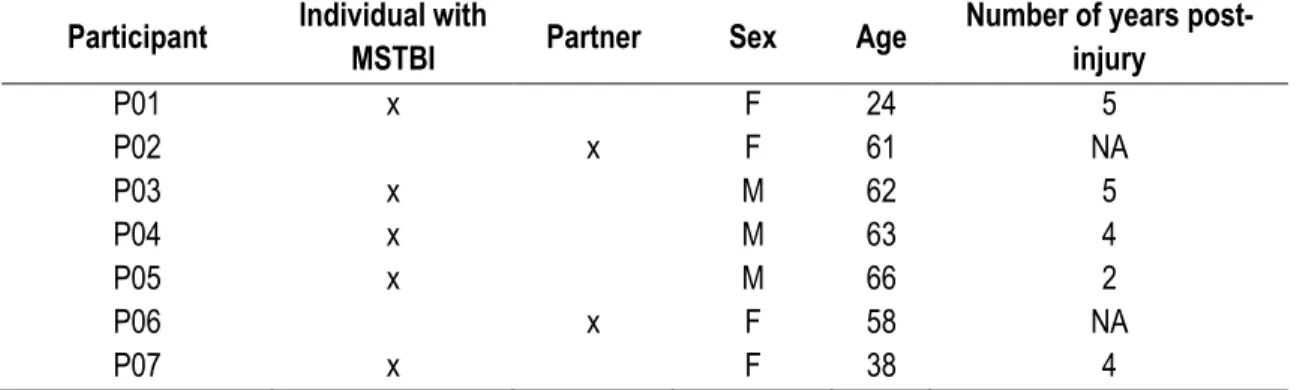
2.4.2 Participants ... 30 2.4.3 Procedure ... 31 2.4.4 Data collection ... 31 2.4.5 Data analysis ... 32 2.5 Results ... 32 2.5.1 Study participants ... 32
2.5.2 Preferred form of tools to be created ... 32
2.5.3 Subjects to be covered by an information toolkit ... 33
2.5.4 Prototype development ... 37
2.5.5 Perception of the prototype ... 38
2.5.6 Modifications of the prototype and creation of additional tools ... 39
2.6 Discussion ... 40 2.7 Limitations ... 42 2.8 Conclusion ... 42 2.9 Declaration of interest ... 43 2.10 Acknowledgements ... 43 2.11 References ... 43
Chapitre 3 – User experience of a post-TBI sexuality information toolkit ... 49
3.1 Résumé ... 49
3.2 Abstract ... 49
3.3 Introduction ... 50
3.4 Method ... 50
vi 3.4.2 Procedure ... 51 3.4.3 Data analysis ... 52 3.5 Results ... 52 3.5.1 Usability ... 52 3.5.2 Usefulness ... 52 3.5.3 Desirability ... 53 3.5.4 Accessibility ... 53 3.5.5 Credibility ... 53 3.5.6 Findability of information ... 53 3.6 Discussion ... 53 3.7 Conclusion ... 54 3.8 References ... 54 Discussion ... 56
Retour sur l’objectif 1 ... 56
Retour sur l’objectif 2 ... 57
Retour sur l’objectif 3 ... 59
Démarche globale ... 60
Évaluation de l’acceptabilité et dissémination ... 61
Futures avenues ... 62
Limites ... 63
Conclusion ... 64
Bibliographie ... 65
Annexe A – Lettres d’information et formulaires de consentement ... 69
Annexe B – Invitations à l’égard des individus et des proches ... 74
Annexe C – Liste de sujets fournie aux participants ... 76
Annexe D – Guides d’entretien ... 77
Guide d’entretien 1 ... 77
Guide d’entretien 2 ... 79
Guide d’entretien 3 ... 81
Annexe E – Liens vers les présentations Prezi ... 82
Annexe F – Feuille d’information ... 83
vii
Liste des figures
Phases du développement des connaissances, adapté du Knowledge to action framework de Graham (2006)
... 6
PRISMA flowchart of the integrative review ... 12
Operational aspects of a discussion about sexuality during the rehabilitation of individuals with TBI ... 12
Co-creation process ... 29
Prototype’s introduction screenshot ... 38
One Prezi presentation introduction screenshot ... 40
viii
Liste des tableaux
Description of included publications (n=17) ... 13 Description of the participants to the co-creation process ... 32 Description of the participants to the user experience assessment ... 52
ix
Liste des sigles
APT Amnésie posttraumatique CPG Clinical practice guidelines
MSTBI Moderate to severe traumatic brain injury GPC Guide de pratique clinique
PLISSIT Permission, Limited information, Specific suggestions, Intensive therapy TBI Traumatic brain injury
TCC Traumatisme craniocérébral TCCL Traumatisme craniocérébral léger
x
Le premier ennemi de
la connaissance n’est pas l’ignorance,
c’est l’illusion de la connaissance.
Stephen Hawking
xi
Remerciements
Qui eût cru que la nécessité d’asseoir des triplets dans le bain me mènerait au doctorat ? Le hasard fait parfois si bien les choses.
Lorsque Marie-Eve m’a proposé de faire une maîtrise en février 2016, elle a réussi en quelques jours à ouvrir une porte que je tentais de garder bien fermée depuis un moment. Trois ans plus tard, il n’y a pas une semaine qui passe sans que je me sente privilégiée de réaliser des études dans des conditions si optimales. Marie-Eve et Marie-Pierre, merci pour tous ces échanges qui m’ont amenée à me dépasser. Merci d’avoir crû en mes idées et de m’avoir appuyée dans la réorientation du projet. Merci pour vos lectures et relectures, mais également pour votre intuition dans le fait de m’obliger, parfois, à lâcher prise. Je suis consciente de l’énergie que vos rôles requièrent, et je vous suis très reconnaissante d’avoir choisi de me soutenir. Marie-Eve, je tiens à souligner la chance exceptionnelle que j’ai eue de te rencontrer. Sans ta volonté de m’offrir un contexte de travail propice à la conciliation étude-famille, et ton soutien à la diffusion des résultats de ma maîtrise dans différents congrès, nous savons toutes deux que la suite des choses serait bien différente pour moi. Tu as été et tu demeures l’une des personnes les plus déterminantes dans ma vie. Merci.
Je tiens également à souligner le soutien constant de ma famille et belle-famille dans ma démarche. Un merci tout spécial à ma mère, qui a su, depuis toujours, promouvoir l’importance du sentiment d’avoir accompli ce que je pouvais, au-delà de celle des résultats aux évaluations. Maintenant que cette étape tire à sa fin, je peux certes affirmer que j’ai fait ce que j’avais à faire.
Il va sans dire que le soutien de mon amoureux a été essentiel à la réalisation de mon projet. Simon, merci d’être l’homme, le conjoint et le père exceptionnel que tu es. Tu es mon pilier.
Les derniers remerciements reviennent à tous ces gens, près de moi, qui ont fait partie de mon quotidien et qui y ont ajouté beaucoup de positif à leur façon. Myriam, Mélissa, Chantal, Julien, Claudia, Élody et tant d’autres collègues appréciés, vous avez largement contribué à une ambiance de travail stimulante et agréable et ça n’a pas de prix.
xii
Avant-propos
Les trois articles intégrés à ce mémoire ont été rédigés par l’auteure du présent document, qui en est première auteure. Ces trois manuscrits ont été révisés par Dre Marie-Eve Lamontagne, directrice de recherche, et Dre Marie-Pierre Gagnon, codirectrice, qui sont respectivement deuxième et troisième auteures. Par ailleurs, le premier manuscrit a également été révisé par Dr Jhon Alexander Moreno, expert dans le domaine de la sexualité chez la population adulte ayant subi un traumatisme craniocérébral. Il est quatrième auteur de l’article. Ce premier manuscrit, qui figure au chapitre 1, a été soumis à la revue Sexuality and Disability le 13 décembre 2018 et a été accepté pour publication le 27 mai 2019. Il s’intitule: Talking about sexuality in the context of
rehabilitation following traumatic brain injury: an integrative review of operational aspects. Le deuxième
manuscrit intitulé Co-creation of a post-TBI sexuality information toolkit : a patient-oriented project se trouve au chapitre 2. Il a été soumis à la revue Disability and Rehabilitation le 30 mai 2019. Un troisième manuscrit intitulé
User experience of a post-TBI sexuality information toolkit a par ailleurs été soumis au Journal of Participatory Medicine le 29 mai 2019. Il figure au chapitre 3.
1
Introduction
Prévalence et incidence du traumatisme craniocérébral
Le traumatisme craniocérébral (TCC) survient lorsque le cerveau frappe la boîte crânienne soudainement et violemment ou lorsqu'un objet perce le crâne et pénètre dans le tissu cérébral[1]. Les principales causes du TCC sont les accidents de la route, les agressions, les chutes et les accidents de sport[2]. Chaque année, environ 69 millions (95% IC 64–74 millions) d’individus subissent un TCC à travers le monde[3]. En Amérique du Nord, l’incidence annuelle des TCC est estimée à 1299 cas par 100 000 individus (95% IC 650–1947)[3]. L’Enquête sur la santé dans les collectivités canadiennes réalisée en 2010-2011 révélait que 133 000 personnes vivaient avec un TCC au pays[4]. En raison de cette incidence élevée qui excède celles des lésions médullaires, du cancer du sein, de la sclérose en plaques et du VIH/SIDA réunies[5], les TCC sont qualifiés d’épidémie silencieuse[6].
Ce type de traumatisme représente la principale cause de morbidité et de mortalité liée à une blessure à l’échelle mondiale[7]. Bien que la grande majorité des décès liés aux TCC soient enregistrés dans les pays à faible revenu ou à revenu intermédiaire[8], les chiffres demeurent substantiels pour l’Amérique du Nord. À titre d’exemple, un estimé de 56 000 morts liées à un TCC était dénombré aux États-Unis en 2013[2].
Le TCC représente de plus un grave problème de santé publique. Les répercussions socioéconomiques de cette problématique se chiffrent en milliard de dollars chaque année à l’échelle mondiale[7] compte tenu des séquelles entraînées à long terme sur les plans physique, cognitif, émotionnel et comportemental. Au Canada, le total des coûts directs associés au traumatisme craniocérébral atteignait approximativement les 151,7 millions de dollars pour les années 2000-2001. Ceci incluait 150,7 millions (99,3%) en soins hospitaliers, 0,3 million (0,2%) en soins prodigués par des médecins et 0,7 million (0,5%) en médication[9]. En 2013, aux États-Unis seulement, 2,5 millions de visites aux urgences liées à un TCC ont été enregistrées, de même qu’environ 282 000 hospitalisations[2].
Répercussions du traumatisme craniocérébral
Lors de la prise en charge, la sévérité neurologique du TCC est évaluée. Celle-ci peut être considérée comme légère, modérée ou grave. Cette classification est principalement déterminée en fonction de trois variables, soit : 1) le score à l’échelle de Glasgow, qui est un indicateur de l’état de conscience; 2) la durée de la perte de conscience; et 3) la durée de l’amnésie posttraumatique (APT), au cours de laquelle l’individu n'est pas en mesure de se souvenir de manière constante des événements quotidiens. Ces indicateurs ne devraient pas être pris séparément pour déterminer la sévérité du TCC.
2
Un TCC sera donc jugé léger si le score à l’échelle de Glasgow est entre 13 et 15; si la durée de l'altération de conscience est de moins de 30 minutes; et si la durée de l’APT est de moins de 24 heures[10]. Les conséquences du TCC léger (TCCL) peuvent être relativement mineures et temporaires. Les symptômes physiques ressentis peuvent inclure des maux de tête, de la confusion, des étourdissements, des vertiges, de la nausée, des vomissements, de la fatigue, des changements dans les habitudes de sommeil, des problèmes d’élocution et des difficultés d’équilibre. Des conséquences sensorielles peuvent aussi être perçues, soit : une vision floue, un bourdonnement dans les oreilles, un mauvais goût en bouche, des changements dans l’odorat, de même qu’une sensibilité à la lumière et aux sons. Des répercussions sur le plan cognitif et psychologique peuvent aussi être observées, soit : des difficultés sur les plans de la mémoire, la concentration, l’attention et la pensée, des symptômes dépressifs et de l’anxiété, ainsi que changements ou sautes d’humeur[11]. Chez une minorité d’individus, ces symptômes peuvent persister et se chroniciser, influençant ainsi la qualité de vie des individus ayant subi un TCCL.
Un TCC sera par ailleurs considéré comme modéré si le score à l’échelle de Glasgow est entre 9 et 12; si la durée de l’altération de conscience est entre 30 minutes et 6 heures; et si la durée de l’APT est entre 1 et 14 jours. Le diagnostic d’un TCC grave reposera quant à lui sur un score entre 3 et 8 à l’échelle de Glasgow, un coma de plus de 6 heures et une APT se prolongeant au-delà de deux semaines[10]. Les individus qui subissent un TCCMG peuvent présenter les mêmes symptômes que ceux d’un TCCL, auxquels peuvent s’ajouter de nombreuses autres manifestations. Sur le plan physique, ceci inclut les troubles de la conscience préalablement décrits, des maux de tête persistants ou qui s’amplifient, des vomissements répétés, une diminution du contrôle vésical et intestinal, des convulsions, la dilatation de l’une ou des deux pupilles, un manque de coordination, des perturbations du langage et des troubles de sommeil et d’éveil[11]. Sur le plan sensoriel, les dysfonctions les plus fréquentes incluent la perte de l’audition, les engourdissements et les troubles de la vision. Sur le plan cognitif et psychologique, une profonde confusion pourrait être notée, de même que de l’agitation, des déficits marqués de l’attention, du traitement de l’information, des fonctions exécutives, de l’orientation et de la mémoire. Des problèmes sur les plans émotionnel, comportemental, et de la personnalité sont également rapportés[12]. D’autres répercussions ou comorbidités liées à l’évènement traumatique incluant des incapacités motrices, des blessures et fractures, ainsi que de la douleur peuvent s’ajouter au portrait clinique.
Les besoins des usagers à la suite d’un TCCMG sont donc souvent multiples et complexes. Le processus de réadaptation de ces individus requiert l’intervention d’une équipe spécialisée et interdisciplinaire. Une telle équipe inclut idéalement les professions suivantes : orthophoniste, ergothérapeute, physiothérapeute, travailleur social, neuropsychologue, psychologue, infirmières, médecin de familiale et/ou physiatre, technicien ou assistant en réadaptation, nutritionniste, technicien en loisir et pharmacien[12]. Ces cliniciens sont formés à reconnaître les déficits résultant du TCCMG et à trouver des moyens d’y remédier. Les clients et leur famille
3
identifient généralement l’optimisation de l'autonomie de l’individu comme priorité, et les professionnels travaillent donc tous pour que l’individu réalise des gains sur le plan des capacités fonctionnelles. Les principaux objectifs concernent généralement la marche, la communication, les activités de la vie quotidienne, dont l'alimentation, l’habillement et l’hygiène, ainsi que la régulation du comportement et l’intégration sociale. Cependant, il existe un domaine de fonctionnement qui fait rarement l'objet de discussions, mais qui demeure néanmoins un domaine d’importance pour de nombreuses personnes, peu importe la gravité ou le type d’atteintes, soit celui de la sexualité.
Plusieurs des répercussions préalablement identifiées, incluant les dommages potentiels au lobe frontal et temporal, de même que les changements sur les plans physique, hormonal, cognitif, émotionnel et de l’humeur, peuvent entraîner des difficultés sexuelles[13, 14]. Parmi les plus communes, on note la baisse du désir, la baisse de la capacité à devenir excité et à maintenir l’excitation, et la difficulté ou l’incapacité à atteindre l’orgasme[14, 15]. Ces répercussions sont rapportées à la fois chez l’homme[16-19] et chez la femme[18, 20] et sont plus fréquentes chez les individus ayant subi un TCC que chez la population en général[21]. Une diminution de la qualité de vie sexuelle, une hausse de l’insatisfaction sexuelle et une baisse de la satisfaction liée à la relation amoureuse sont aussi documentées[22]. Ces difficultés peuvent être accompagnées ou non d’un désintérêt à l’égard des activités sexuelles[19]. Une diminution de la fréquence des rapports sexuels[23] serait par ailleurs plus marquée chez les individus souffrant de dépression à la suite du TCC[24]. À cet effet, la dépression serait l’un des prédicteurs négatifs les plus sensibles de la dysfonction sexuelle post-TCC[23, 25] avec l’âge plus avancé des individus[26]. À l’inverse, bien que ce soit moins fréquent, une hypersexualité est une répercussion parfois observée[27].
D’autres changements secondaires au TCC peuvent également affecter la sexualité et la fréquence des rapports sexuels. Sur le plan physique, la fatigue significative et persistante ressentie par 30% à 75% des individus ayant subi un TCC qui peut avoir un impact sur la fréquence désirée et réelle des relations, ainsi que sur l’importance accordée à la sexualité. Certaines personnes vivent en outre de la douleur, des difficultés de mobilité et de positionnement, et des problèmes d’équilibre. Par ailleurs, des sensations perçues comme étant agréables avant l’accident peuvent par la suite être perçues comme étant désagréables. Une absence de sensation, ou une sensation plus faible qu’auparavant est aussi documentée[18]. Sur le plan psychologique, une perception négative de l’image corporelle, modifiée à la baisse en lien avec l’accident subi, affecte l’estime de soi et contribue au sentiment d’être peu attirant[14, 18]. Les difficultés cognitives peuvent par ailleurs entraîner une diminution de la capacité à fantasmer qui se répercute sur le désir, l’excitation, et l’atteinte de l’orgasme[28].
Sur le plan relationnel, les répercussions du TCC entrainent de nombreux changements au sein du couple[19, 29]. L’impression que l'individu ayant subi le TCC est un inconnu compte tenu des modifications liées à la
4
personnalité, les difficultés de communication, les changements de rôles préalablement occupés par les partenaires, l’isolation sociale sont tous des facteurs qui font obstacle à l’intimité entre les partenaires[19]. En ce sens, des difficultés sexuelles incluant une dysfonction sexuelle ou des insatisfactions liées au fonctionnement sexuel peuvent également être survenir chez le ou la partenaire de l’individu ayant un TCC[23]. Le fonctionnement sexuel du ou de la partenaire serait fortement associé à celui de l’individu ayant subi un TCC. Sans surprise, une baisse de la satisfaction sexuelle est ainsi fréquemment rapportée[29].
Il est important que les difficultés susmentionnées soient discutées avec un médecin. Un déficit en testostérone, par exemple, ou des symptômes dépressifs peuvent être en cause. Des tests sanguins et un bilan médical complet s’imposent. Les difficultés sexuelles peuvent par ailleurs être liées ou amplifiées par la prise de certains médicaments. Par exemple, les antidépresseurs, les neuroleptiques de 2e génération, certains médicaments antispasmodiques et les benzodiazépines peuvent avoir de tels effets indésirables[12]. Selon la source du problème, des solutions pourront donc être envisagées.
Dans le cadre de la réadaptation des adultes ayant subi un TCCMG, la plupart des professionnels adopteraient une approche réactive vis-à-vis la présence de dysfonctions sexuelles chez leurs patients[30]. Ils en discuteraient ainsi principalement si l’individu ayant subi un TCC ou le couple aborde la question. Pourtant, informer et faire de l’éducation auprès des personnes en réadaptation et leurs proches au sujet de la sexualité fait partie d’une approche holistique à adopter en réadaptation[31]. Des études révèlent d’ailleurs que la grande majorité des cliniciens perçoivent qu’il s’agit d’une composante importante qui devrait faire partie intégrante du programme de réadaptation [14, 32]. Les impacts directs et indirects du TCC sur le fonctionnement sexuel justifient la nécessité d’informer et outiller les patients, qu’ils soient célibataires ou en couple. L’étude de Moreno, Gan [33] met en lumière que cette clientèle voudrait que les difficultés sur le plan de la sexualité soit prises en compte lors de la réadaptation.
Objectifs et étapes du projet
Le but du projet est de codévelopper des outils d’information sur la sexualité post-TCC adaptés aux besoins des adultes ayant subi un TCCMG et leurs proches, pour favoriser les échanges sur la sexualité en réadaptation. Les trois objectifs du projet, lesquels sont respectivement présentés dans les trois chapitres suivants, sont :
1. réaliser une revue intégrative sur la façon d’aborder la sexualité en contexte de réadaptation à la suite d’un TCC;
2. codévelopper des outils d’information sur la sexualité post-TCC avec et pour les individus ayant subi un TCCMG et de leurs proches;
5
La revue intégrative réalisée examine comment aborder la sexualité post-TCC en contexte de réadaptation. Les aspects documentés, incluant comment discuter de sexualité, qui devrait tenir la discussion, à quel moment et avec quels outils constituent le fondement théorique sur lequel s’appuie la seconde étape du projet.
La cocréation d’outils d’information favorisant une discussion sur la sexualité repose ensuite sur les besoins et les attentes des utilisateurs potentiels, soit des individus ayant subi un TCCMG et des proches. Les participants sont donc invités à orienter la forme (p. ex. vidéo, présentation Prezi narrée, affiche, etc.) et le contenu (p. ex. communication portant sur la sexualité, effets de la médication, contraception, gestion des comportements à risque) des outils en développement. La production des outils est réalisée individuellement, puis améliorée de façon itérative grâce à la perspective d'individus ayant un TCCMG et des proches.
L’expérience des utilisateurs est finalement évaluée auprès d’un groupe distinct de participants pour déterminer si le contenu des outils développés est : utile, utilisable, attrayant, repérable, accessible et crédible. Des modifications additionnelles peuvent ensuite être réalisées au besoin.
Cadre théorique
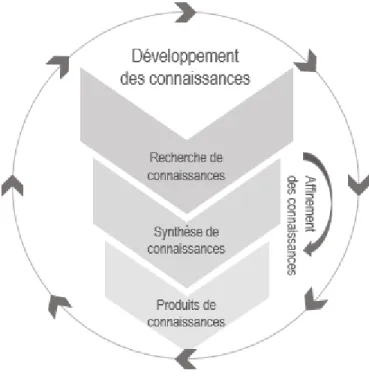
Le modèle du Cycle des connaissances à la pratique[34] (traduction du Knowledge to action framework) permet de situer les étapes phares du projet d’un point de vue théorique dans le cadre d’une action en transfert de connaissance. Ce projet s’inscrit tout particulièrement dans les phases du Développement des connaissances, présentées au centre du modèle[35] (Figure 1). Ceci est préalable, dans le présent contexte, à la mise en œuvre d’une pratique, qui consiste à informer les personnes ayant un TCCMG sur la sexualité post-TCC par l’entremise de matériel adapté à leurs besoins. Les étapes du développement, qui incluent a) la recherche de connaissances; b) la synthèse de connaissances; et c) les produits de connaissances permettent de réaliser un affinement progressif des connaissances sur le sujet. L’information qui en résulte est ensuite, en théorie, mieux arrimée aux besoins des utilisateurs que celles présentées dans les études primaires. À cet effet, la revue intégrative réalisée (Synthèse des connaissances) permet d’abord de faire une synthèse des informations existantes sur le sujet de la sexualité discutée dans le cadre de la réadaptation à la suite d’un TCC. Le contenu est ensuite clarifié et épuré puis bonifié de façon itérative selon les besoins des utilisateurs pour être présenté en un format adapté à la pratique, soit des outils à l’intention des patients (Produits de connaissances).
6
Fig. 1 Phases du développement des connaissances, adapté du Knowledge to action framework de Graham (2006).
Sur le plan des phases du Cycle d’action, la démarche est uniquement centrée sur la sélection et le développement d’une pratique. Il n’est pas attendu que l’implantation formelle soit réalisée dans le cadre du présent projet de maîtrise. Une étape d’évaluation conclut toutefois la démarche, et pourrait permettre l’amélioration des ressources d’information a posteriori. Il faudra prévoir de façon ultérieure et à l’extérieur du cadre de cette maîtrise des activités formelles d’implantation et d’évaluation afin de conclure le Cycle de la connaissance à la pratique.
Cette action en transfert de connaissances est à l’intention directe du patient (patient-direct knowledge
translation intervention). À cet effet, la création de matériel d’information sur la santé est une intervention
reconnue qui, par l’engagement des patients, tend à favoriser leur connaissance, leur expérience, leur utilisation des services, leurs comportements liés à la santé et leurs résultats de santé[34]. Plus spécifiquement, le développement d’information adaptée aux personnes ayant un faible niveau de littératie aurait des effets bénéfiques à la fois sur la connaissance de ces individus et sur leurs comportements liés à la santé[36].
7
Chapitre 1 - Talking about sexuality in the context
of rehabilitation following traumatic brain injury: an
integrative review of operational aspects
1.1 Résumé
Malgré les recommandations invitant les professionnels à discuter de sexualité avec leurs patients ayant subi un traumatisme craniocérébral (TCC), peu d’adultes bénéficient d’un tel entretien en réadaptation. Pour identifier ce qui favoriserait ces échanges, une revue intégrative des aspects opérationnels d’une discussion sur la sexualité post-TCC en contexte de réadaptation a été réalisée dans sept bases de données. Une double sélection a été effectuée, suivie de l’examen des références, des articles ayant cité les documents retenus et des articles similaires identifiés par les bases de données. Dix-sept documents ont été sélectionnés. Huit documents (47,1%) avancent que le sujet est la responsabilité de toutes les disciplines de la réadaptation. Cinq documents (29,4%) indiquent que la sexualité devrait être discutée dès le début de la réadaptation. Neuf documents (52,9%) soutiennent que de la documentation écrite ou d’autres types de ressources (vidéo, sites Web) portant sur la sexualité post-TCC devraient être offertes.
1.2 Abstract
An integrative review of the literature reporting operational aspects (how, when, who, with what) of rehabilitation professionals’ discussion of sexuality with individuals with mild to severe traumatic brain injury (TBI) was conducted. Searches were carried out in seven databases. Records published from 2000 to 2017 were screened and selected (n=504). The methodological quality of empirical studies was evaluated using the Mixed Methods Appraisal Tool. Seventeen full-text articles, book chapters, books, and essays were included and analysed in this integrative review. Prerequisites for discussing sexuality were identified. The PLISSIT model's usefulness in getting professionals to talk about sexuality was highlighted by nine sources (52.9%). An interdisciplinary team approach, with different aspects of sexuality covered by specific professions, was principally endorsed. Five sources (29.4%) reported that the best timing to initiate a discussion about sexuality would be during early rehabilitation. Nine sources (52.9%) supported the provision of written materials or other supporting resources, such as websites and videos. To integrate sexuality as a component of TBI rehabilitation, professionals need to be aware of their role, the information and education that should be provided, the appropriate timing, the tools that might be helpful, and the support from their organizations. There is a need for more intervention studies to assess the efficacy, alternating or combining different operational aspects identified in this review.
8
1.3 Introduction
Sexuality is an increasingly important aspect to include in traumatic brain injury (TBI) rehabilitation. Two recent clinical practice guidelines (CPG) promoted the inclusion of a discussion about sexuality with individuals with TBI [1,2]. In 2016, the Canadian CPG for the rehabilitation of adults with moderate to severe TBI recommended the following practice (https://braininjuryguidelines.org/modtosevere/) [1]:
A discussion about sexuality should be carried out with individuals following traumatic brain injury. The discussion should be initiated by an appropriately trained clinician and should cover the following aspects of sexuality: physical aspects (e.g., positioning, sensory deficits, erectile dysfunction, drugs, disruption to menstrual cycle) and psychological aspects (e.g., communication, fears, altered roles, disinhibition, threats to safety, and sense of attractiveness).
CPGs provide recommendations recognized as essential pillars of the quality of care improvement. However, the results of a cross-sectional study conducted in 2016 in 29 TBI rehabilitation programs in Quebec and Ontario (Canada) revealed that 21 (72.4%) do not include a discussion about sexuality with individuals with TBI [3]. Just like in other countries [4-8], rehabilitation professionals in Central Canada are not proactively addressing sexuality concerns in individuals with TBI. Rehabilitation programs rarely include sex therapists in the rehabilitation team [9], and individuals with TBI can have difficulties identifying a professional to address sexuality concerns. The majority of TBI professionals consider they are not sufficiently qualified to address sexual issues and further training is needed [10-12]. Moreover, without a specific professional obligation to address sexual issues, the responsibility is both everyone’s and no one’s. Therefore, team members rarely take charge of systematically addressing sexuality with individuals with TBI. Considering the evidence suggesting that sexual issues are common after TBI [13-17] and that individuals with TBI express a need to address their sexuality concerns [18], the implementation of a discussion about sexuality is a necessary step to promote positive sexual health outcomes in individuals with TBI and their partners [19,20]. Sexuality is an integral aspect of the human experience and sexual satisfaction reflects on the quality of one’s life [21]. A majority of healthcare professionals agree that this is an important topic to be covered in rehabilitation [6,22,23]. To support the implementation of the Canadian TBI CPG recommendation about sexuality, an understanding of the operational aspects involved in the discussion about sexuality in the context of TBI rehabilitation is urgently needed. Operational aspects include a response to the following questions: a) How to hold the discussion?; b) Who should lead it?; c) When should professionals and individuals with TBI address the subject?; and d) What tools could support the discussion? Providing clear guidelines about the most appropriate context for a discussion about sexuality, the professionals that should be involved, the best timing, and the tools supporting it would facilitate service delivery and prevent or reduce professionals’ common feeling of embarrassment and lack of confidence to address the topic [24].
9
A discussion is defined by the Oxford English Dictionary Online [25] as the “Treatment of a subject, in speech or writing, in which the various facts, opinions, and issues relating to it are considered; the action or process of talking about something in order to reach a decision or to exchange ideas”. Based on Simpson’s description of the five areas of sexuality-related service provision [26], such a discussion involves exchanges of information on both parts about different aspects of sexuality and education. It might result in referral to specialist sex therapists, but it excludes assessment and the provision of treatment.
Important pieces of information about how to operationalize a discussion about sexuality in rehabilitation are scattered and important aspects needed by professionals to adequately plan such a service are partially described by previous studies [8]. For example, Moreno, Gan, Zasler, and McKerral (2015) explored the perceptions of 38 individuals with TBI using a questionnaire regarding sexuality and service delivery [18]. Participants in this study mentioned that it would be appropriate that professionals from different backgrounds address sexuality and reproductive health [18]. The results of the study suggested that a discussion on the topic should not be the responsibility of a single rehabilitation team member and that sexuality needs after TBI are best addressed using an interdisciplinary approach. Dyer and das Nair (2014) conducted four focus groups with a total of 24 rehabilitation professionals to explore their perceptions and experiences talking about sexuality in the context of TBI [6]. The results of the study indicate that professionals do not need to be experts in sexual issues to open the dialogue and that a more proactive approach is needed to effectively deal with this sensitive subject in TBI rehabilitation. All these authors partially address the question, but a broader coverage of the subject is required to adequately plan services in rehabilitation. To our knowledge, previous studies have not extensively documented the dimensions involved in the operationalization of a discussion about sexuality in the context of the rehabilitation of individuals with mild to severe TBI. Improving the# understanding of operational aspects (how, who, when, with what) can help rehabilitation professionals adopt a proactive approach. Thus, the objective of this integrative review is to identify and synthesise the literature exploring how rehabilitation professionals should discuss sexuality with individuals having sustained a mild to severe TBI.
1.4 Methods
The current study is an integrative review of the literature [27,28]. This type of review is conducted with a systematic approach; thus, the literature search stage followed the steps from the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram [29]. The Research ethics board of the CIUSSS
de la Capitale-Nationale approved the larger study in which this review was conducted.
Search strategy
This integrative review of the literature was conducted from May to July 2017. The research question was: “What are the operational aspects (how, who, when, with what) of a discussion about sexuality between rehabilitation
10
professionals and individuals who sustained a mild to severe TBI?” The authors did not have any a priori hypotheses. In the current study, TBI is understood according to the definition of The Brain Injury Association of America, as: “An alteration in brain function, or other evidence of brain pathology, caused by an external force.” [30] Seven databases (Cochrane Library, PubMed, Embase, PsycINFO, Web of Science, CINAHL, and PEDRO) were searched using free text terms, Boolean operators, and truncation. Keywords used to perform a wide search were sexual* AND traumatic brain injury. In the Cochrane Library, PubMed and Embase, the search strategy was sexual*[Title/Abstract] AND traumatic brain injury[Title/Abstract]. This strategy was adapted to each database’s research field choices. The keywords and search strategies used were: sexual*[Abstract] AND traumatic brain injury[Abstract] in CINAHL, (sexual* and traumatic brain injury).ab in PsycINFO, TOPIC: (sexual*) AND TITLE: (traumatic brain injury) in Web of Science, and (sexual* and traumatic brain injury) in PEDRO. Data were limited by timeframe, from January 2000 to July 2017 to focus on contemporary studies.
To identify further sources, a secondary search consisting of the three following steps was conducted: a) screening of the reference lists of included publications; b) citations searches performed through Google Scholar for records meeting the inclusion criteria, and c) screening of the 25 similar references suggested by the databases, where available.
Inclusion criteria
The following inclusion criteria were used to screen and select the sources: a) quantitative/qualitative/mixed methods studies, literature reviews, discussion papers (expert opinions), books, theses, and essays; b) published in English or in French (both official languages in Canada) between January 2000 and July 2017, and c) reporting operational aspects of a discussion about sexuality between rehabilitation professionals and adults with mild to severe TBI.
Exclusion criteria
References were excluded from the review if they were: a) studies describing general aspects of post-TBI sexual functioning; b) papers focusing on the assessment and treatment of inappropriate sexual behavior and sexual dysfunction, c) articles regarding assessment tools and measures; and d) studies focusing on the partner or the family of individuals with TBI.
Study selection and data extraction
First, two reviewers (PMD and MEL) screened eligible titles and abstracts independently based on inclusion and exclusion criteria. After agreeing on the screening outcome, they reviewed full-text publications for inclusion. A third reviewer (MPG) was involved in case of disagreements in the selection of full-text sources. A pretested extraction grid was used and populated by the first author (e.g., authors, publication title, year of publication,
11
level of evidence, and operational aspects involved in a discussion of sexuality following TBI). Open coding was used to identify categories as needed.
Level of evidence and quality assessment
The level of evidence of each document was assessed using the rating system for the hierarchy of evidence for intervention/treatment questions [31]. Two raters used the Mixed Methods Appraisal Tool (MMAT) to evaluate the methodological quality of the empirical studies identified [32,33]. The MMAT was chosen for its utility to assess the quality of qualitative, quantitative, or mixed methods studies. This tool includes two screening questions and nineteen quality components for five different types of research designs. Two team members independently rated each study according to quality criteria and using a number of stars between zero and four (****), representing the overall quality score (i.e., More stars indicate a higher quality). In case of disagreements, raters reached an agreement following a discussion.
Data analysis
Publications were analysed using both a deductive and an inductive approach to thematic analysis [34]. Categories related to the research question were identified, as well as those that emerged from selected full-texts. Data relationships were identified within each category. Categories and codes were added as they appeared. Discussions were held periodically between reviewers to reach a consensus on emerging codes and categories. Both categories and codes were reviewed and refined following an iterative process to detect recurrence, overlaps, complements, and contradictions.
1.5 Results
The initial search yielded 504 results (Figure 1). After removing duplicates, 253 records were reviewed based on the relevance of the content of their titles and abstracts. Inter-reviewer agreement was 96.4% (κ = 0.83). According to the guidelines, Cohen’s kappa ranging from 0.80 to 0.90 indicates a strong level of agreement between two judges[35]. Titles and abstracts review led to the rejection of 225 records (88.5%), and the review of 28 full-text publications. After this stage, 11 articles or books were included, and inter-reviewer agreement reached 0.93% (κ = 0.86). The secondary search involving the screening of references, citations, and similar articles suggested by the database led to the inclusion of six more references. Together, a total of 17 full-text articles, book chapters, books, and essays were included in the review (i.e., one book, three book chapters, seven descriptive cross-sectional studies, three non-systematic literature reviews, and three expert opinion pieces with levels of evidence from six to seven) [31].
12 Fig. 1 PRISMA flowchart of the Integrative review
As shown in Table 1, of the 17 sources, there were six empirical cross-sectional studies to be rated with the MMAT. Of those, one study obtained two stars (MMAT score = **), and five studies obtained three stars (MMAT score = ***). The remaining 11 non-empirical sources could not be analyzed using the MMAT.
13 Table 1. Description of included publications (n=17)
Authors Year Addressed categories Publication/
study type
Level of evidence
MMAT score
Prerequisites How Who When With what
Downing and Ponsford 2016 x x Quantitative descriptive
cross-sectional study VI ***
Moreno, Gan, Zasler and
McKerral 2015 x x x x Quantitative descriptive cross-sectional study VI ** Moreno, Arango-Lasprilla and McKerral 2015 x x Quantitative descriptive cross-sectional study VI ***
Moreno and das Nair 2015 x x x x Qualitative descriptive cross-sectional study VI ***
Dyer and das Nair 2014 x x x x Qualitative descriptive
cross-sectional study VI ***
Simpson and Long 2004 x x x x Qualitative descriptive
cross-sectional study VI *** Chateauneuf 2014 x x x x Essay - Qualitative descriptive cross-sectional study VI ---
Aloni and Katz 2003 x x x x x Book VII ---
Sandel, Delmonico and
Kotch 2013 x x x x x Book chapter
VII ---
Zasler and Martelli 2011 x x x Book chapter VII ---
Sander 2011 x Book chapter VII ---
Sander 2010 x x x x x Expert opinion VII ---
Simpson 2001 x x x x x Expert opinion VII ---
Connell, Coates and
Wood 2014 x
Non systematic literature review
VII
--- Moreno, Arango Lasprilla,
Gan and McKerral 2013 x x x x
Non systematic literature review
VII
---
Oddy 2001 x x Non systematic literature
review
VII
---
14
Categories
Operational aspects to hold a discussion about sexuality included five different predetermined or emergent categories: a) What are the prerequisites for discussing sexuality? (Prerequisites), b) How should the discussion be conducted? (How), c) Who should lead the discussion? (Who), d) When is the best time to hold the discussion? (When), and e) What tools could support the discussion? (With what). Figure 2 illustrates the categories.
Fig. 2 Operational aspects of a discussion about sexuality during the rehabilitation of individuals with TBI
a) What are the prerequisites for discussing sexuality?
Prior to asking clinicians to promote positive sexuality outcomes and address sexual issues during rehabilitation, the literature highlights a number of aspects to be considered. The “Framework of action to enhance the sex lives of people with traumatic brain injury” by Simpson (2001) provides insight into the prerequisites. There are
15
five areas involved in sexuality-related service provision in the context of TBI [26]. Service provision includes information, assessment, referral, education, and treatment. The organizational structure must include agency policy and procedures, staff training, inter-service networks, legislation, as well as resource and knowledge development to foster a sustainable service provision. Ten sources (58.8%) stressed the importance of increasing professionals’ level of sensitivity and comfort by providing staff with training about sexuality [6, 18, 26, 36-42]. Three (17.6%) of these ten sources actively promoted training the staff working in the TBI rehabilitation program, even professionals whose work is not directly related to sexual health [6, 26, 38]. Two sources (11.8%) emphasized the need for staff training to cover aspects relevant to all four levels of the PLISSIT model [26,38]. Among the topics to be covered in the training, it is recommended to include the importance of sexuality as a health outcome [40], the development of sexuality across the life span [6,39], the human sexual response [39], personal dimensions of sexuality [36], sexual identity [38], and cultural differences [6, 36, 39]. In addition, training should include topics more specific to sexuality and disability [18,38] such as the possible causes of sexual dysfunction [37], the impact of TBI on sexual function [6,38,39], and the effects of medication on sexuality [6]. The need to teach how to talk about sexuality in the rehabilitation setting [37] and strategies to conduct an interview and open the discussion [26] was also highlighted. This included the explanation of the PLISSIT model [26], the identification and management of sexual risks [6] and the preservation of self-esteem, self-confidence and body image [38]. Aspects related to self-management skills and soft skills were also highlighted, such as the openness to differences [36] and attitudinal issues [38,39]. There were other training topics recommended in the literature, such as the importance of learning about appropriate resources for sexual exploration [6], treatment options [37], contraception [6], and the realities of lesbian, gay, bisexual, and transgender individuals with TBI [6].
A qualitative study highlighted that the content of the training should be oriented towards an “exposure-based approach” to building skills in addressing sexuality [6]. Participants in the study expressed that increasing the level of comfort in talking about sexuality could not be achieved by solely attending lectures and receiving information. They have to experience the discussion through the educational process. Aloni & Katz (2003) also stressed the value of a desensitization process, complementary to education about the sexuality of individuals with TBI [38]. Either ongoing supervision [6,38] or continuing education should be provided following the initial training [18,38]. In line with this, some authors recommended strategies involving the organization of group discussions or workshops [39], case studies allowing to find appropriate responses to actual [18] and fictitious situations [36], as well as role play to simulate discussions about sexual issues [37]. The creation of a sexuality committee gathering staff from different disciplines, who can provide support to rehabilitation teams was also suggested [26].
16
Another aspect included in Simpson’s framework and endorsed by three other authors is the development of organizational policy and procedures related to sexuality [6,26,39,42]. Clear guidelines describing the facility’s approach to addressing sexuality contributes to the provision of consistent services to individuals with TBI [6,26]. This should be accompanied by procedures to be followed for common demands and controversial practices, written in line with the relevant legislation [26]. To facilitate decision-making, it is advised that aspects not to be covered by the rehabilitation team be identified through the facility’s policy. To facilitate referrals, it is also recommended to develop a reference network between the rehabilitation facility and sexual health specialists or therapy services (23.5%) [6,18,26,42]. Simpson (2001) highlights the importance to train the specialists about the impact of TBI to help them tailor their approach to common impairments in individuals with TBI [26]. Furthermore, it is recommended that facilities provide readily available sexuality-related resources [6,26,42], such as leaflets, brochures, and videos. If none can be identified, the development of new resources designed for the staff’s needs should be a priority to facilitate the discussion.
b) How should the discussion be conducted?
Adoption of the PLISSIT model
A total of 52.9% of the sources supported the utility of the PLISSIT model to help professionals to talk about sexuality with individuals with TBI [6,18,26,38,39,42-45]. Developed by Annon in 1976 for the field of sexology, the PLISSIT model provides a phased approach that can also be used by health and rehabilitation professionals in the context of TBI [46]. The Permission level implies that through language, attitudes, and actions, professionals create a positive environment allowing individuals with TBI to initiate the conversation about sexuality during the rehabilitation process [43]. Limited Information includes the provision of general, yet precise information, and education about sexuality following TBI. Specific suggestions refer to the use of a wide range of techniques and approaches in addressing the individual with TBI’s unique sexual issues, such as making focused recommendations, providing counseling, and initiating social skills training [38]. The Intensive Therapy level is appropriate when a higher level of expertise is needed to address sexual dysfunctions that could not be solved through previous levels of intervention [43]. It relies on specialized experience and training, and thus might not be available in all facilities [26]. Nevertheless, Simpson (2001) stressed that rehabilitation teams should, at a minimum, be able to provide interventions at the first three stages (i.e., Permission, Limited Information, and Specific Suggestions) [26].
Recommendations for specific attitudes and behaviors
A total of 41.2% of the sources provided general recommendations about attitudes and behaviours to be adopted by professionals. It was suggested that they should be warm and empathetic [26,42] while opening up the
17
discussion to normalize the fact that sexual issues are common after TBI and that there are available solutions [37,47,48]. A non-judgmental style in the staff’s comments and attitudes will increase comfort in addressing sexuality issues and help individuals with TBI to avoid feeling ashamed or embarrassed [26,39,47]. In 17.6% of cases, it is reported that treating the subject like any other activity of daily living and discussing frankly potential sexual difficulties contributes to allowing permission to discuss them [37,42,48]. Also, seven sources (41.2%) recommended being proactive when addressing sexual concerns with individuals with TBI [6,18,26,36,38,43,45]. Including a question about sexuality in at least one formal rehabilitation assessment tool was considered useful to help professionals address the topic. This inclusion was supported by 29.4% of the sources [6,26,37,44,47].
Provision of information and education
In line with the PLISSIT model, 58.8% of the sources suggested providing limited information about commonly occurring changes in the sexuality of individuals with TBI [18,26,37-41, 43,48,49]. Also, 64.7% of the sources stressed the importance of education on sexually transmitted diseases, contraceptive methods, and sexual abuse [18,26,36,37,39-43,47,48], while another 64.7% encouraged providing general and specific suggestions on ways to deal with sexual concerns [18,26,37,38,40-43,47-49]. This includes, for example, alternative strategies to obtain sexual satisfaction [37], including different positions and hands-free devices [48], as well as the provision of information on continence management [26]. Once different aspects of sexuality following TBI are covered, seven sources (47.1%) emphasized the importance of recommending a comprehensive medical examination to exclude or treat any physical causes of post-TBI sexual changes [26,37,39,40,42,47-49]. Medication side effects were suggested as a potential source of sexual dysfunction in 41.2% of the sources [18,37-39,42,47,49].
Identification of the recipients of information
As carefully mentioned by Sander [37], “a sensible guideline is that the person with injury should always be the recipient of information on sexuality”(p.10). Three articles (17.6%) highlighted that if the individual with TBI is in a relationship, both partners should have the opportunity to discuss sexuality with a professional during rehabilitation [49] or receive sexuality related education [37,45]. Three sources (17.6%) mentioned that information and education could be provided to the individual, the partner, as well as caregivers and family members [18,39,48] to prevent loss of information due to attention and memory problems [37]. Two other references (11.8%) stressed the importance of interviewing the couple when the individual with TBI has a partner [38,42].
18
Aloni & Katz (2003) suggested that group sessions were beneficial in post-TBI sexual rehabilitation [38]. However, two studies (11.8%) reported that individuals with TBI show preference for one-on-one conversations [36,41]. Another study reports divided opinions among professionals, some of whom are in favour of providing more private spaces for individual discussion while others believe that group interactions could foster peer-support [6]. Two sources (11.8%) also mentioned that group discussions are an alternative to individual formats, but information and education about sexuality can be provided using both strategies [41,43].
c) Who should lead the discussion?
A total of 47.1% of sources indicated that discussing sexuality is the responsibility of all rehabilitation disciplines [6,18,26,38,41,43-45] and 29.4% specifically mentioned that the individual with TBI should have the opportunity to choose the professional with whom to hold the discussion [6,18,38,43,45]. Also, eight references (47.1%) pointed out that the best option would be an interdisciplinary team approach, with different aspects of sexuality covered by specific professions [18,26,36,38-40,43,44]. Another approach included the identification of one or two professionals who might be more comfortable with sexuality and rehabilitation to systematically address the topic with individuals with TBI [37]. The role of occupational therapists in increasing independence in self-care activities, including sexual activities was also acknowledged [48]. In addition, 11.8% of sources supported the relevance of having a sex therapist as a permanent staff member on the interdisciplinary team or a consultant available upon request [36,38]. Given the limited availability of sexologists in rehabilitation centers, this seems unfeasible as a general recommendation but nevertheless appropriate for an Intensive Therapy phase of the PLISSIT model of sexual intervention. A similar idea was brought up in relation to the need to have a physician responsible for supervising the management of sexuality-related issues [37].
d) When is the best time to hold the discussion?
While opinions are divergent on this subject, 29.4% of the sources indicated that the best timing to initiate a discussion about sexuality would be during early rehabilitation [37-39,42,43] and 5.6% suggested that the subject should be brought up before sexual concerns are identified [26]. During a focus group held with individuals with TBI and their caregivers, divergent opinions on the moment to provide information about sexuality were represented [37]. While some participants preferred receiving information before discharge from inpatient rehabilitation, another group believed it would be preferable to wait until problems arise, which tends to happen when the individual with TBI is back at home. Still, earlier interventions were considered better than late intervention strategies. Another document highlighted the possibility that the initial phases of rehabilitation might be too early for a comprehensive discussion about sexuality. Consequently, it supported the option of addressing sexual issues through outpatient services [8]. Chateauneuf (2015) also pointed out that it takes time to develop a relationship of trust, given the intimate and personal nature of sexuality [36]. Sandel, Delmonico &
19
Kotch [39] stated that: “learning readiness needs to be determined on an individual basis; the timing, topic areas, amount, and method of education should be individualized” (p.926). These results showed that there is a variety of points of view on the question.
e) What tools could support the discussion?
A total of 52.9% of sources supported the provision of written materials or other supporting resources, such as websites and videos [6,26,37-41,48,49]. A qualitative analysis of online sources indicated that little information is specifically designed for individuals with TBI, as opposed to the information available for informal caregivers and families [40]. The lack of materials for women, single people, and non-heterosexual individuals was also highlighted.
Information provided should be in a clear and simple language, and written materials should be adapted to individuals with TBI [37,40]. The authors of one study highlighted the relevance of providing an online pamphlet (i.e., Sexual Functioning and satisfaction after Traumatic Brain Injury - an Education Manual [50]) as well as a tip card (i.e., Intimacy, Sexuality and Sex after Brain injury [51]) to individuals with TBI to facilitate the discussion [49]. For 23.5% of sources, two formal programs created for professionals are useful in addressing sexuality following TBI [18,38,41,43]: Simpson’s You and Me sex education program and Aloni and Katz’s extensive treatment program for sexual difficulties after TBI [38]. These two resources provide education on post-TBI sexuality, as well as information on the treatment of sexuality-related issues.
1.6 Discussion
The goal of this review was to appraise operational aspects of a discussion about sexuality between rehabilitation professionals and individuals with TBI (e.g., the appropriate setting, its content, the professional who should lead it, and the tools or materials that could support it). An initial discussion about sexuality is necessary to open the subject and allow permission to identify and treat potential sexual problems post-TBI. The review allowed identifying different strategies used by professionals to address sexuality concerns with individuals with TBI. It provides a detailed and relevant synthesis of information including the appropriate setting to talk about sexuality, its content, the professional who should hold it, and the tools or materials that could support it. For some of the operational aspects identified, it was possible to recognize convergent perspectives.
The MMAT analysis showed little variability in the quality of available evidence: 83.3% of the few empirical studies included were considered well conducted, with three stars out of four. The common aspect impacting the quantitative studies’ quality was the low response rate (i.e. below the 60% response rate threshold indicated in the MMAT). Most of the studies (66.7%) that were evaluated included information on four out of five categories (prerequisites, how, who, with what).
20
Prerequisites to discussing sexuality
As mentioned in the TBI CPG recommendation [1], discussions about sexuality should be held by appropriately trained clinicians. Staff training is therefore considered to be the main prerequisite to start a conversation about sexuality in rehabilitation settings. However, a high percentage of professionals surveyed in three different studies [10-12] report the lack of or insufficient sexual health education during and after their academic training. Considering the limited time allotted for sexuality-related training in rehabilitation settings, it would be unrealistic to cover the broad range of recommended topics. However, education to enhance the level of comfort in introducing physical aspects (e.g., erectile dysfunction, negative drug effects, disruption to menstrual cycle, sensory deficits) and psychosocial aspects (e.g., communication, altered roles, threats to safety, sense of attractiveness) of sexuality should include theoretical knowledge, and practice with discussions, role playing, and interpersonal skills training. Beyond the provision of theoretical knowledge, training should be an opportunity to gain practical knowledge about the “know how” involved in discussing sexuality [6]. Another recent study showed that training based on the team members’ specific needs (e.g., education on talking about sex), led to a more proactive behavior in all newly trained professionals [52]. An initial training session might, therefore, consist of a balance of different learning approaches to better prepare professionals for broaching the topic of sexuality with individuals with TBI. A further empirical exploration of this approach is needed. Other organizational elements described by Simpson in his framework of action to enhance the sex lives of individuals with TBI stand out as key aspects in enabling professionals to discuss sexuality.
How to conduct the discussion
Addressing sexuality should be done consistently with all individuals with TBI during their rehabilitation. Including a question about sexuality in at least one formal rehabilitation assessment would signify the validity of the topic in TBI rehabilitation. Initially, the subject should be addressed directly with the individual with TBI. For people in a relationship and once professionals have granted permission to address the subject, further discussion could include both the individual with TBI and the spouse or partner. It has been highlighted that partners can also experience sexual dysfunction [53]. Providing information and education to both partners might enable the couple to reach out for support if they identify sexual issues during outpatient rehabilitation or later at discharge. Although less strongly endorsed, giving information to the caregiver or a family member of single individuals remains an area of interest. It would better prepare family and friends to the potential repercussions since sexual issues and dysfunctions might be observed once the individual is back home rather than during inpatient rehabilitation [37]. However, the benefits of this approach should be further explored empirically.
21
Who should lead the discussion
More than 40% of sources vouched for a shared responsibility between all rehabilitation professionals to address sexuality in the rehabilitation of individuals with TBI. In practical terms, to avoid a situation where addressing sexuality is everyone’s and no one’s business, team efforts are required to agree on a procedure that will consistently give individuals with TBI the opportunity to receive information on sexuality, and address the topic with a professional. Whether this is achieved by identifying a number of professionals in the team who are most at ease with talking about sexuality or by giving the mandate to all professionals to inquire about individuals’ willingness to address the subject with them, the important thing is to reach a point of team commitment to addressing sexuality [37]. In this context, all rehabilitation staff should be generally knowledgeable of sexuality issues. The PLISSIT model provides a useful graded structure for the provision of services that can be used to illustrate to professionals that they do not have to be experts to legitimately discuss sexuality. It also acknowledges the possibility to address problematic situations through team meetings or supervision sessions. Since specialized sexuality knowledge is rarely available on hand in rehabilitation settings, teamwork must be valued and supported by the organization and program managers [6,38].
When should the discussion be held
This category is the only one that was not covered by empirical studies. The information available was only retrieved from expert opinion pieces and reviews, and should, therefore, be considered with more caution. The appropriate moment for a discussion about sexuality remains ambiguous. There is no consensus about the specific timing that is more beneficial to address and successfully treat sexual concerns in individuals with TBI. However, most authors advice the “as soon as possible” approach. They suggest that, in line with the call to formally include sexuality in the rehabilitation program, the possibility of discussing it must be mentioned early during the rehabilitation process and reaffirmed on different occasions (e.g., before the first visit home, before the end of inpatient rehabilitation). This would prevent individuals from returning home without having received any information or education about sexuality during rehabilitation. Providing written materials along with other sources of information (videos, websites) would also help professionals and individuals with TBI to address more comfortably this delicate subject while ensuring information is available when the need for it arises.
1.7 Limitations and future directions
This first integrative review of the literature reporting operational aspects to facilitate a discussion about sexuality between rehabilitation professionals’ and individuals with TBI aims at describing how such a service can be offered and orchestrated. Increasing the understanding of operational aspects necessary to initiate and foster a discussion is helpful for effective service provision. In this regard, it provides rehabilitation teams with some general guidelines to plan and include the discussion about sexuality in the rehabilitation program.