© Rebecca Francois, 2018
Adaptation and validation of the multi-dimensional
measure of informed choice to cardiopulmonary
resuscitation (CPR) and invasive mechanical ventilation
(IMV)
Mémoire
Rebecca Francois
Maîtrise en épidémiologie - avec mémoire
Maître ès sciences (M. Sc.)
Adaptation and validation of the
Multi-Dimensional Measure of Informed Choice to
cardiopulmonary resuscitation (CPR)
and invasive mechanical ventilation (IMV)
Mémoire
Rebecca François
Sous la direction de:
iii
Résumé
La majorité des aînés canadiens préfèrent recevoir des interventions de fin de vie non agressives. Pour eux, leur qualité de vie est plus importante que la durée. Les études montrent que les préférences des patients âgés ne sont pas souvent inscrites dans leurs dossiers médicaux. Par conséquent, des interventions agressives comme la réanimation cardiorespiratoire (RCR) et la ventilation mécanique invasive (VMI) sont utilisées plutôt que des soins de confort.
La prise de décision partagée (PDP) est une approche contribuant à diminuer la surutilisation de certaines interventions médicales par des décisions plus éclairées. Lors d’une décision critique sur une intervention de santé, la PDP permet au patient et à son médecin de travailler ensemble pour faire le choix le plus approprié. Les décisions éclairées favorisent des meilleurs effets sur la santé par la réduction de conflit décisionnel, la diminution de l’anxiété et une amélioration de la satisfaction du patient.
Les outils d’aide à la décision utilisés dans le contexte de la PDP facilitent la discussion entre un médecin et son patient. Ils ne sont pas limités au contexte de la PDP, car ils peuvent être une ressource en santé très utile, pour aider les patients confrontés à des décisions de santé difficiles et complexes.
Vu que la PDP et les outils d’aide à la décision supportent la prise de décision informée, des outils validés et multidimensionnels doivent être créés et validés pour des personnes qui font face à des décisions des interventions de fins de vie agressives.
Cet article détaille l’adaptation et la validation du Multi-Dimensional Measure of Informed Choice à la RCR et à la VMI avec des aînés canadiens francophones.
iv
Abstract
Most elderly Canadians wish to avoid aggressive life-sustaining interventions at the end of their lives because they favor quality of life over quantity when they consider the potential suffering that may come with attempts to prolong their lives. Nonetheless, studies show that patient preferences for the care they receive at end-of-life (EOL) often go unrecorded in their medical dossiers and aggressive life-sustaining interventions such as cardiopulmonary resuscitation (CPR) and invasive mechanical ventilation (IMV) are used in lieu of the comfort care that the patient may prefer.
Shared decision-making (SDM) is an approach that research shows leads to patient informed decisions. When faced with the need to make a critical decision about care plans, treatment options, or the uptake of a medical intervention/procedure, SDM allows a patient and their physician to work together to make the most appropriate choice for the patient. This has been shown to lead to improved patient health outcomes such as decreased decisional conflict, decreased anxiety, and higher patient satisfaction.
Patient decision aids (PtDAs) are health information tools that, when used in the SDM context, facilitate the conversation between a physician and their patient. PtDAs are not limited to use in shared decision making because they may also be valuable health resources to patients facing a difficult or complicated health decision.
Because both SDM and the use of PtDAs are shown to lead to patient informed decision-making, validated and multidimensional tools that measure informed choice are needed for those facing decisions about aggressive EOL medical interventions, especially the elderly. This paper explicates, in detail, our attempt to adapt and validate the Multi-Dimensional Measure of Informed Choice (MMIC) to CPR and IMV in an elderly French-Canadian population.
v
Table of Contents
Résumé ... iii
Abstract ... iv
Table of Contents ... v
List of tables ... vii
List of figures... viii
List of equations ... ix
Acronyms ... x
Acknowledgements ... xii
Preface ... xiii
1. Introduction... 1
1.1 End-of-life decision-making in Canada ... 1
1.2 Cardiopulmonary resuscitation (CPR) ... 1
1.3 Invasive mechanical ventilation (IMV) ... 2
1.4 Patient preferences in relation to life-sustaining interventions ... 2
1.5 Shared decision-making (SDM) ... 3
1.6 Patient decision aids (PtDAs) ... 4
2. Objectives ... 5
2.1 Primary objective... 5
3. The Multi-dimensional measure of informed choice (MMIC) ... 6
3.1 Informed value-based decision making using the MMIC ... 10
3.1.1 An informed decision ... 10
3.1.2 An informed value-based decision ... 11
3.1.3 An uninformed decision ... 11
3.1.4 An uninformed value-based decision ... 11
3.2 Use of the MMIC in other studies ... 11
3.2.1 MMIC study comparisons ... 12
3.2.2 Studies that validated their adapted MMIC ... 13
4. Psychometrics ... 17
4.1 Psychometric testing in the health sciences ... 17
4.1.1 Validity ... 17 4.1.1.1 Content validity... 18 4.1.1.2 Face validity ... 18 4.1.2 Reliability ... 19 4.1.2.1 Internal consistency ... 20 4.1.2.2 Test-retest method ... 21
4.1.2.1.1 Cronbach’s coefficient alpha (α) ... 21
4.1.2.1.2 Intraclass correlation coefficient (ICC) ... 23
4.1.2.2 Cohen’s kappa coefficient (κ) ... 24
4.1.2.3 Weighted kappa (κω) ... 25
5. Adaptation and Validation of the Multi-Dimensional Measure of Informed Choice to Cardiopulmonary Resuscitation and Mechanical Ventilation in an Elderly French-Canadian Population ... 26
vi
5.1 Résumé ... 27
5.1.1 Abstract... 28
5.2 Introduction ... 29
5.3 Methods... 30
5.3.1 Study design and setting ... 30
5.3.2 Adaptation of the original MMIC ... 30
5.3.3 Validity and reliability... 31
5.3.3.1 Phase 1 ... 31 5.3.3.2 Phase 2 ... 31 5.3.3.3 Phase 3 ... 32 5.3.4 Description of variables ... 33 5.3.4.1 Knowledge items ... 33 5.3.4.2 Attitude items ... 33 5.3.4.3 Socio-demographics ... 33
5.3.4.4 Informed decision making ... 34
5.3.4.5 Data Analysis ... 34 5.4 Results ... 35 5.4.1 Content Validity ... 35 5.4.2 Face validity ... 36 5.4.3 Test-retest population ... 37 5.4.4 CPR questionnaire ... 39 5.4.5 IMV Questionnaire... 39
5.5 Discussion and conclusion ... 42
5.5.1 Discussion ... 42
5.5.3 Limitations ... 44
5.5.4 Conclusion ... 45
5.5.5 Practice implications ... 46
5.5.6 Acknowledgements ... 46
5.5.7 Informed consent and patient details ... 47
5.5.8 Funding ... 47 5.5.9 Author contributions ... 47 5.5.10 References... 47 Chapter 5 Appendix ... 51 Appendix A ... 51 Appendix B ... 53 Appendix C ... 55 Appendix D ... 59 Appendix E ... 63
Discussion and Conclusion ... 66
Discussion ... 66
Conclusion ... 71
References ... 71
vii
List of tables
Chapter 2 Tables
Table 1 Original MMIC Knowledge Items ... 7
Table 2 Original MMIC Attitude Items ... 8
Table 3 RCT* studies that used the MMIC as a measure of informed choice ... 14
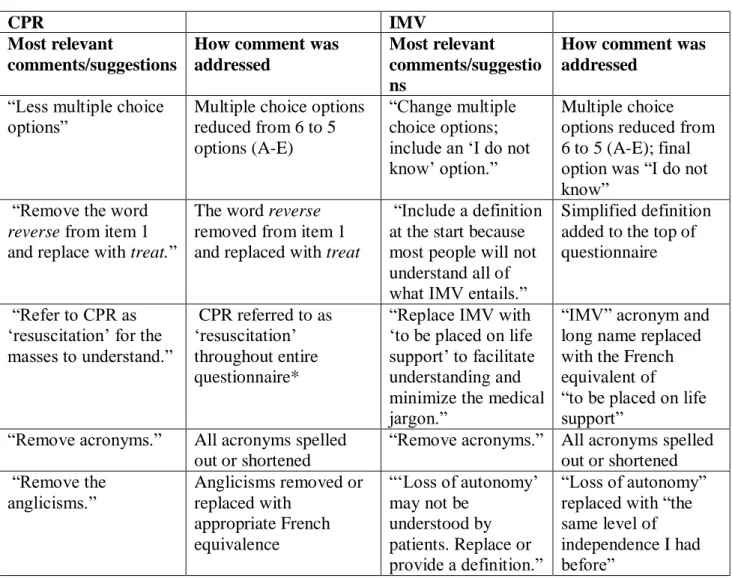
Chapter 5 Tables Table 1 Content Validity Most Relevant Expert Comments ... 35
Table 2 Face Validity Patient Comments ... 36
Table 3 Demographic characteristics of retirement home residents ... 37
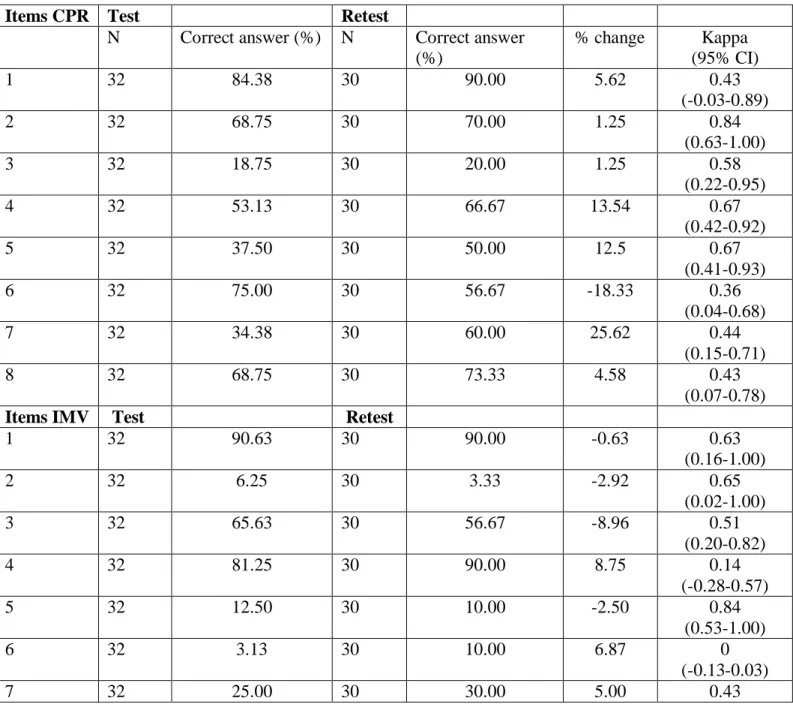
Table 4 Descriptive Statistics for Knowledge Items... 40
Table 5 Descriptive Statistics for Attitude Items ... 41
Table 6 Overall Reliability ... 41
Table 7 Cronbach’s coefficient alpha ... 42
Table 8 Levels of Informed choice for CPR and IMV % (n) ... 42
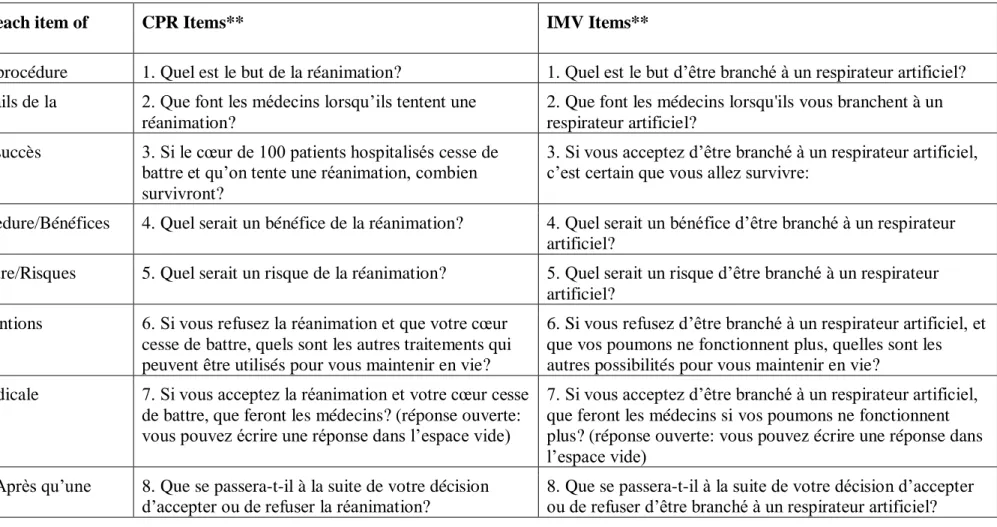
Mémoire Appendix: Table 1 This study’s two adapted MMIC questionnaires ... 76
Table 2 This study’s translated MMIC attitude items ... 77
viii
List of figures
Chapter 2 Figures:
ix
List of equations
Chapter 3 Equations:
Equation 1 : KR-20 equation ... 22 Equation 2 : Cronbach’s coefficient alpha equation ... 22 Equation 3 : Cohen’s kappa equation ... 25
x
Acronyms
CPR Cardiopulmonary Resuscitation
EOL End-Of-Life
IMV Invasive Mechanical Ventilation
MMIC Multi-Dimensional Measure of Informed Choice
PtDAs Patient Decision Aids
SDM Shared Decision Making
ICU Intensive Care Unit
ED Emergency Department
DSS Down Syndrome Screening
ICC Intraclass Correlation Coefficient
Abréviations
RCR La réanimation cardiorespiratoire
VMI La ventilation mécanique invasive
xi
“The Fear of the Lord is the beginning of knowledge...”
Proverbs 1:7
xii
Acknowledgements
I give thanks to God for He is good and I know that His love endures forever.
Thank you to my parents for raising me in the fear and admonition of the Lord; for their love, protection, and spiritual covering.
Thank you to the following individuals:
The research director of this project, for your time and efforts. Stéphane Turcotte for his statistical and epidemiological guidance.
Carrie Anna McGinn and Maude Dionne for their intellectual and administrative support and responsiveness in all aspects related to the organization of the study and the writing of this memoire.
A profound thank you goes to Mrs. Julie Bernard, the Director of Résidence Jazz-Lévis and to all the retirement home residents and ICU patients who participated in the different phases of this project.
To the experts who participated in the content validity phase of this project and to all the co-authors of the integrated article.
Finally, thank you to Dre Caroline Diorio (Director of the Department of Epidemiology at Université Laval) for her leadership and sagacity.
xiii
Preface
The article included in this memoire (chapter 5) has not yet been submitted for publication. The article’s references, in-text citations and sections are formatted according to the requirements of the targeted journal of publication, Patient Education and Counseling. As explained in the methods section of chapter 5, all phases of this study’s protocol were approved by the ethics committee of the Centre intégré en santé et services sociaux de Chaudière-Appalaches (CISSS CA) (Hôtel-Dieu de Lévis site) in Lévis, Québec, Canada: [Reference: 2017-001]. Permission to conduct the test-retest phase at the retirement home was given by the retirement home Director. Because this project was considered a “minimal risk” study, only verbal consent was required by patients and residents who agreed to participate.
This study has also been approved, by way of exemption, by the Comités d’éthique de la
recherche avec des êtres humains de l’Université Laval (CÉRUL). All documentation
attesting to these approvals, consents, and exemptions can be made available upon request. Finally, I am currently finishing a second article that describes in detail, the use of the MMIC as a measure of informed choice for CPR and IMV based off of the results of this study. It will present the proportion of test-retest participants who made an informed value-based decision vs. those who made an uninformed value-value-based or simply value-value-based decision. The informed choice percentages reported in chapter 5 only represent two classification of choices; however, the second article will classify participant choices according to the eight categories proposed by Michie et al., 2002.
xiv
Author Contributions to the integrated article are as follows:
Rebecca Francois is the principal author. She contributed to the study conception and
design, data collection and data management, as well as the statistical analysis and interpretation, and original article draft and subsequent revisions.
Patrick M. Archambault is the research director and contributed to the study conception
and design, data collection, article revision, and statistical analysis and interpretation.
The following co-authors contributed to article revision:
France Légaré Patrick Plante
Emmanuelle Bélanger Holly O. Witteman Alexis F. Turgeon Tom van de Belt
1
1. Introduction
1.1 End-of-life decision-making in Canada
At the end of their lives, most elderly Canadians wish to avoid aggressive life-sustaining interventions that could potentially prolong their life but not necessarily its quality [1]. For these elderly patients, quality and comfort at end-of-life (EOL) are most important, however, studies show that patient preferences for EOL care are going undocumented and unrealized [1–5]. In 2013, a multicenter cohort study in 12 Canadian hospitals found that although 11.9% of patients favored the use of life-sustaining medical care with resuscitation, 58.7% favored a mix of non-aggressive treatments (or “comfort care”) and full medical care but these preferences were only recorded in 4.5% of stated goals [2]. The study also found that the majority of patients could clearly communicate their preferences, but their wishes were not expressed due to ineffective communication between patients, family members, and their physicians [2,3].
That said, qualitative studies including those conducted by Giles and Miyasaki, 2009 [6], Workman and Mann, 2007 [7], and Heyland et al., 2009 [8] allude to the dissatisfaction of patients with EOL care provided within the intensive care units (ICUs) of Canada [6–8]. Much of this dissatisfaction stems from modifiable factors, among which the most important to patients and family members facing EOL decisions are: “Not to be kept alive on life support when there is little hope for a meaningful recovery,” “That information about your disease be communicated to you by your doctor in an honest manner,” and “To receive help making difficult treatment decisions” [1]. Unfortunately, these aspects of care are seldom conveyed to health care professionals and when they are, they go unspecified in treatment plans [2]. Nevertheless, even in cases where patients have clearly outlined and readily available advanced directives, they do not curb overexposure to aggressive forms of EOL medical care [3].
1.2 Cardiopulmonary resuscitation (CPR)
Cardiopulmonary Resuscitation (CPR) is an aggressive life-sustaining intervention. According to the American Heart Association (AHA), CPR is defined as: “…an emergency lifesaving procedure performed when a person stops breathing or the heart stops beating.”
2
CPR is needed when an individual suffers cardiac arrest (CA) and if initiated early by a bystander, CPR has been shown to increase a person’s chances of surviving [9].
In-hospital CPR survival rates vary by study but according to Peberdy et al., 2003 [10] using the National Registry of Cardiopulmonary Resuscitation (NRCPR), the adult in-hospital survival rate of CPR after cardiac arrest was 17% [10]. In addition to having a low in-hospital survival rate, for those who do survive, the secondary physical effects of CPR (rib fracture, damage to internal organs, and brain damage) bring into question the dignity of its use on some individuals under certain circumstances, namely, elderly ICU patients who are often times frail, terminally ill, or suffering from an underlying chronic condition [11].
1.3 Invasive mechanical ventilation (IMV)
A second aggressive life-sustaining intervention used in ICUs is invasive mechanical ventilation (IMV).
As described by Cheifetz, 2003 [12], “mechanical ventilation refers to the use of life-support technology to perform the work of breathing for patients who are unable to do so, on their own” [12]. These life-sustaining technologies may include nasal prongs or a mask, which will provide breathing support via a patient’s nose or mouth (non-invasive mechanical ventilation) or may include the invasive forms of IMV that require the physician to “bypass the patient’s upper airway with an artificial airway [such as:] endotracheal tube [ETT], laryngeal mask airway, or [a] tracheostomy tube” [12]. Regardless, however, of whether a patient is receiving invasive or non-invasive mechanical ventilation, research suggests that there is no significant difference in the all-cause mortality rate for the elderly; although, non-invasive mechanical ventilation is shown to have a lower 90-day mortality rate [13].
1.4 Patient preferences in relation to life-sustaining interventions
CPR and IMV are considered life-sustaining medical procedures but are overwhelmingly unfavored by elderly patients who prefer comfort care at EOL [14]. Unfortunately, both
3
procedures seem to be overused in many Emergency Department (ED) and ICU settings [15]. Consequently, the use of these two interventions does not correspond with patient preferences signifying that: patients are undergoing medical procedures that are inconsistent with their values, physicians are requesting medical procedures without consulting their patients, and both lead to the inappropriate misuse and overuse of hospital resources and medical procedures [16].
1.5 Shared decision-making (SDM)
One of the most effective methods in decreasing the misuse of medical interventions and that allows patients to receive care in-line with their values is through shared decision making (SDM) [17,18]. SDM is a decisional model that has grown in recognition and implementation among physicians and health care practitioners and scientists, alike [19,20]. SDM involves the equal participation of the patient and their physician when making a decision concerning the patient’s medical care, treatment plans, or screenings. Unlike the paternalistic decisional model where the physician is responsible for the final decision with little to no input from the patient or the autonomist decisional model where the patient makes the final decision, in the SDM model the physician and the patient work together to reach a final decision that values the patients preferences while also respecting the medical evidence and advice of the physician [17,18,20–22]. In a SDM approach, the physician contributes invaluable medical knowledge necessary for the patient to make an informed decision; however, the SDM approach similarly validates patient values, which are equally indispensable for a patient to make a fully informed value-based decision [23].
In addition to increased patient knowledge and less chance of litigation for the physician, SDM leads to patient informed decision-making and informed consent. Patients who make informed decisions about their health have better overall health outcomes, less decisional conflict, less anxiety, higher satisfaction with their healthcare provider, higher adherence levels, and they do not undergo unnecessary procedures [24]. The value and impact of patient informed decision-making continues to be researched in different domains, but studies are showing consistent results as to the positive effects of both SDM and informed
4
decision making on patient health. That is why, validated and multidimensional tools that can assess the quality of patient decisions is of paramount importance for vulnerable population groups facing decisions about life-sustaining interventions like CPR and IMV.
1.6 Patient decision aids (PtDAs)
The shared decision-making process can be facilitated by the use of patient decision aids (PtDAs). PtDAs serve as evidence-based tools to present information about specific medical interventions or tests [25]. They provide a clear definition of the procedure, they help the patient weigh the risk-benefits (sometimes represented using pictograms to assist patient comprehension), and they clearly explain alternative options available to a patient [26,27]. Moreover, it is important to note that patient decision aids help facilitate doctor-patient conversations and interactions in the SDM context but do not replace them.
A 2016 systematic review by van Weert et al., 2016 [28] evaluated the effectiveness of decision aids for older adults and found that the use of decision aids among the elderly increased their risk perception, participation in decision making and knowledge, in addition to decreasing decisional conflict levels. Van Weert et al., 2016 also affirmed the need for future research to evaluate the decision aids used for older adults facing healthcare treatment decisions and acknowledged the fact that although, decision aids are created to impact patient knowledge, few studies exist that describe how knowledge or attitude measures are established [28]. This is a gap that this study serves to bridge in adapting and validating a multidimensional assessment tool for aggressive medical interventions.
5
2. Objectives
This memoire has one objective:
2.1 Primary objective
To adapt the Multi-Dimensional Measure of Informed Choice (MMIC) to cardiopulmonary resuscitation and invasive mechanical ventilation for an elderly population of intensive care unit patients and to evaluate the psychometric properties of both adapted questionnaires.
6
3. The Multi-dimensional measure of informed choice (MMIC)
Measurement tools such as questionnaires, tests, or surveys can assess the congruence between a patient’s stated preferences, their level of knowledge, and their subsequent behavior regarding a specific medical intervention or diagnostic test. In so doing, these tools can also evaluate the impact of patient decision aids in the SDM context, allowing researchers and physicians to refine and better adapt information so that patients receive relevant support to make informed value-based decisions [29,30]. One such tool is the Multi-Dimensional Measure of Informed Choice (MMIC) questionnaire. The MMIC is a 9-item questionnaire that uses knowledge, attitude, and uptake (behavior) to measure informed choice [31].
The original MMIC was developed by Marteau et al., 2001 [32] to measure if pregnant women were making informed decisions about choosing to accept or decline prenatal Down’s syndrome testing [31,33]. The first 8 items are multiple choice questions that determine an individual’s knowledge (Table 1), while the final question uses 4 Likert scales to measure an individual’s attitude toward the targeted intervention or diagnostic test (Table 2). The 8 knowledge items provide a general assessment of a person’s knowledge level concerning the intervention. Each item is scored as either “0”, representing an incorrect response or “1” denoting a correct response for a total possible score that ranges between 0 and 8. Michie et al. 2002 [33] divides these total knowledge scores to represent either “poor” or “good” knowledge using the sample median as the cut-off point; therefore, individual’s with a total score higher than 4 are said to have “good” knowledge while those with a total score equal to or lower than 4 are classified as having “poor” knowledge [33]. The final item classifies an individual’s attitude as “positive” or “negative” toward the intervention using a 4-item Likert scale based on the Theory of Planned Behavior (TPB); Michie et al., 2002 [33] uses “attitude” as a surrogate for “values.” The Likert scale options are: “Beneficial vs. Harmful” (1-7), “Important vs. Unimportant” (1-7), “A good thing vs. a bad thing” (1-7), and “Pleasant vs. Unpleasant” (1-7) (Table 2). Again, the median is used to dichotomize attitudes. Total attitude scores above the denoted median are considered positive and total scores at or below the median are classified as negative attitudes [33].
7
Table 1 Original MMIC Knowledge Items including the guidelines that informed their construction
1989 RCP guidelines Original MMIC Items for Down syndrome [31]
Information about the condition(s) being screened for.
1. Which of these conditions do you think that the test screens for? (you may tick more than one box for this question)*
The meaning of a low risk result. 2. If 100 women decided to have the
screening test, about how many do you think would have a low-risk result? *
The percentage of women who are likely to have a low risk result.
3. What do you think a low-risk result means? *
The meaning of a high risk result. 4. Again, imagine that 100 women undergo the test. About how many do you think would have a high-risk result? *
The percentage of women who are likely to have a high
risk result.
5. What do you think a high-risk result means? *
The risks of miscarriage from further tests (e.g. amniocenteses) that will be offered to women who have a high risk result.
6. Imagine 100 women with a high-risk result. About how many do you think will be found to have a baby with Down’s syndrome? *
The percentage of women with a high risk result who have a baby with Down’s syndrome.
7. Some women are offered further tests (amniocentesis or CVS, which involve inserting a fine needle into the womb). What are the possible consequences of this test? The fact that a termination of pregnancy
(abortion) is offered if further tests show that the baby does have Down’s syndrome.
8. If further tests show that the baby
definitely does have Down’s syndrome, what would a woman be offered: *
8 Table 2 Original MMIC Attitude Items
Original MMIC Attitude Items for Down syndrome
For me, having the screening test for Down’s syndrome when I am 15 weeks pregnant will be:
(a) Beneficial 1 2 3 4 5 6 7 Harmful (b) Important 1 2 3 4 5 6 7 Unimportant (c) Bad thing 1 2 3 4 5 6 7 Good thing (d) Pleasant 1 2 3 4 5 6 7 Unpleasant
9
Marteau et al., 2001 [31,33] also created a 3-dimensional typology of eight cells to help classify the choices represented by the MMIC (Figure 1). If a patient is measured to have “good” knowledge about an intervention, a positive attitude toward the intervention, and they accept to undergo the proposed treatment or test (positive uptake), then they have made an informed value-based decision and would be grouped in Cell 1 [31,33]. Likewise, if a patient is measured to have “good” knowledge about the intervention, a negative attitude toward the intervention, and they decline to undergo the proposed test (negative uptake), then they have also made an informed value-based decision and would be grouped in Cell 4. These two cells (1 & 4) represent those who have made the most informed choice because their decision reflected their values [31,33].
If an individual is measured to have “poor” knowledge about an intervention or test, regardless of whether their attitude is consistent with their uptake, they have made an uninformed decision, albeit a value-based one. Other variations of choices exist, however, according to the original authors, these choices lack the coherence to be considered “informed” and must therefore be considered “uninformed” decisions [31,33]. A few of these cells also raise several questions and according to the authors, seem “problematic.” Cell 6, for example, represents an individual who has poor knowledge, a negative attitude but they chose to accept the procedure. The authors suggest that such an individual would have declined the test if they were better informed [33]. An additional hypothesis should consider the role of outside forces on an individual’s decision such as family and social pressure to accept an intervention even if it is against a person’s values and they do not know much about it. Cell 3 is another cell considered problematic because it represents those who have good knowledge and a positive attitude, but they chose to decline the test [33]. Again, it can be hypothesized that those who fall in this category may be making decisions because of peer pressure and fear of how they may be viewed for making a decision against “the norm.”
10
3.1 Informed value-based decision making using the MMIC
The 3-dimensions suggested by Michie et al., 2001 [33] to classify decisions comes from the O’Connor and O’Brien Pallas definition of « effective decision-making » which states that:
“An informed choice is one that is based on relevant knowledge, consistent with the decision-maker's values and behaviourally implemented.”
Therefore, when knowledge and attitude are assessed along with uptake, an individual’s decision can be categorized into one of four groups:
3.1.1 An informed decision
An informed decision is a decision made with relevant and accurate information (“good knowledge”) about the topic for which the decision must be made.
Figure 1 The Marteau et al (2001) decisional matrix that classifies a choice according to the breakdown of its 3-dimensions: knowledge, attitude, and uptake
11 3.1.2 An informed value-based decision
An informed value-based decision is a decision made with relevant and accurate information (“good knowledge”) about the topic and the decision maker’s personal values and preferences toward the medical intervention or procedure match their final decision to accept or decline the intervention.
3.1.3 An uninformed decision
An uninformed decision is a decision where the individual has poor knowledge irrespective of whether uptake reflects attitude.
3.1.4 An uninformed value-based decision
A decision can be value-based but uninformed. Decisions that fall under this category have been made with poor knowledge, but the individual’s attitude does reflect their uptake. So, those with positive attitude do accept the medical intervention and those with negative attitudes decline the medical interventions; but both do so with a poor level of knowledge about the intervention they have accepted or declined.
3.2 Use of the MMIC in other studies
In a Cochrane Systematic Review about the use of decision aids for treatment or screening decisions, out of 10 studies that sought to measure informed choice, 8 used a modified version of the MMIC or applied the underlying 3-dimensional typology of knowledge, attitude, and uptake to measure informed choice [34]. One study was not included in the systematic review, but did use the MMIC to measure informed choice [35].
Of these nine studies, three were about Down syndrome or prenatal testing for fetal abnormalities (Dormandy et al., 2006, Björklund et al., 2012, Nagle et al., 2008) [35–36, 38], three studies looked at informed choice among women for mammography screening (Korfage et al., 2013, Mathieu et al., 2007, and Mathieu et al., 2010) [39–41], two studies focused on informed choice for colorectal cancer screening (Steckelberg et al., 2011 and Trevena et al., 2008) [42,43], and one study was about informed choice for bowel cancer screening (Smith et al., 2010) [44] (Table 3). Informed choice was the primary outcome for eight of the nine studies and all study designs were randomized controlled trials (RCTs)
12
with either 2 or 3-arm groups. Six studies (Dormandy et al., 2006 [35]; Björklund et al. 2012 [36]; Nagle et al. 2008 [38]; Korfage et al. 2013 [39]; Steckelberg et al. 2011 [42] & Smith et al. 2010 [44]) adapted the MMIC to their subject area, which ranged from the omission of items, the addition of items or the complete adaptation of the questions to a different diagnostic test. Three studies out of the nine (Mathieu et al. 2007 [40]; Steckelberg et al. 2011 [42]; Smith et al. 2010 [44]) validated their adapted measures of informed choice in a pilot test before use in the intervention group (Table 3).
3.2.1 MMIC study comparisons
Consistently, knowledge about the intervention and informed choice concerning the decision or intention to accept or forego screening were significantly higher in the intervention groups, which received a decision aid, than in the control groups. (Table 3) In eight studies, informed choice within the intervention groups ranged from 34-76% (Table 3). Trevena et al., 2008 [43] reported the lowest percentages of informed choice of 20.9% and 5.8% in the intervention and control arms, respectively [43]. The authors do not provide a possible reason for low rates of informed choice; however, they do mention that they had unavoidable low recruitment rates due to ethical restraints. Nonetheless, all studies reported that individuals in the intervention groups had higher percentages of informed choices, showed lower decisional conflict, and lower levels of anxiety. One study (Mathieu et al., 2007 [40]) reported that the use of a decision aid did not alter patient screening habits [40]. Unfortunately, this is in stark contrast to the other studies, which revealed that the use of a decision aid not only increased negative attitudes toward the intervention, but also, decreased uptake of medical procedures. The study that reported unaltered screening levels, reported that they were in partnership with BreastScreen NSW, which specified that they wanted to know how the use of a decision aid would impact the demand for their services [40].
There are several differences between the aforementioned studies and the project that this paper presents. For these nine studies, measuring informed choice about a diagnostic test after the intervention of a decision aid was either the primary or secondary outcome. This study’s primary outcome was to assess the psychometric properties of the MMIC adapted
13
to two medical interventions used in ICUs. Furthermore, our populations varied in both age and sex.
3.2.2 Studies that validated their adapted MMIC
In the study conducted by Smith et al., 2010 [44], knowledge questions were pilot tested in a low-literacy population to measure if participants would understand two facets: conceptual knowledge and numerical knowledge. Conceptual knowledge was used to test if participants understood “the underlying concept” associated with bowel cancer and numerical knowledge was used to measure if participants understood the average number of people affected by bowel cancer [44]. Knowledge questions were informed by the guidelines for screening set forth by the UK General Medical Council [44]. Steckleberg et al., 2011 [42] adapted the MMIC for colorectal cancer screening and pilot tested the questionnaire in a separate sample population of 62 individuals who met the same inclusion criteria as the study [42]. Finally, Mathieu et al., 2007 [40] does not provide a detailed description of their validation steps aside from the fact that minor changes were made to their questions after being pilot tested in a sample of 70 women [40].
Gourounti and Sandall, 2011 [45] is the only published study that culturally adapted the MMIC to prenatal Down syndrome testing for a Greek population and assessed its psychometric properties [45] in the same way that this study sought to adapt and validate the MMIC to CPR and IMV in a francophone population. A comparison of both studies is provided in table 3 of the memoire appendix.
14 Table 3 RCT* studies that used the MMIC as a measure of informed choice
Study 1** Study 2 Study 3 Study 4 Study 5 Study 6 Study 7 † Study 8 † Study 9 †
Title Informed Choice in antenatal Down syndrome screening: A cluster-randomised trial of combined versus separate visit testing Audiovisual information affects informed choice and experience of information in antenatal Down syndrome screening – A randomized controlled trial Use of a decision aid for prenatal testing of fetal abnormalities to improve women’s informed decision making: a cluster randomized controlled trial A decision aid to support informed choices about bowel cancer screening among adults with low education: randomized controlled trial Effect of evidence based risk information on “informed choice” in colorectal cancer screening: randomized controlled trial Informed Choice about breast cancer prevention: randomized controlled trial of an online decision aid intervention Informed Choice in Mammography Screening Helping women make choices about mammography screening: An online randomized trial of a decision aid for 40-year-old women Randomized trial of a self-administered decision aid for colorectal cancer screening
Authors Dormandy et al., 2006
Björklund et al., 2012
Nagle et al., 2007 Smith et al., 2010 Steckelberg et al., 2011 Korfage et al., 2013 Mathieu et al., 2007 Mathieu et al., 2010 Trevena et al., 2008 Study Design
Cluster RCT RCTa 3-arm Cluster
RCT
RCT RCT RCT RCT RCT RCT
Primary Outcome
Informed Choice Informed Choice Informed Choice and Decisional Conflict Informed Choice and Preferences for Involvement in Screening Decisions
Informed Choice Informed Choice Informed Choice Knowledge Informed Choice and Integrated
15 Secondary Outcomes None Attitude, knowledge, and experiences of information Anxiety, depression, attitudes to the pregnancy/fetus, and acceptability of the resource Decisional Conflict Decision Satisfaction Confidence in Decision Making Anxiety, interest in screening, worry about developing bowel cancer, acceptability of materials Knowledge and a combination of actual and planned uptake None Decisional conflict and Anxiety Intention and Informed Choice Test Uptake, Decision Aid Acceptability, and Psychological Outcomes Use of the MMIC Yes; To measure informed choice using: Knowledge Attitude Uptake Yes; To measure informed choice using: Knowledge Attitude Uptake Yes; To measure informed choice using: Knowledge Attitude Uptake Yes; To measure informed choice using: Knowledge Attitude Uptake Yes; To measure informed choice using: Knowledge Attitude Uptake Yes; To measure informed choice using: Knowledge Attitude Uptake No; conceptual use of the 3 dimensions: Knowledge Values Intention No; conceptual use of the 3 dimensions: Knowledge Values Intention No; conceptual use of the 3 dimensions: Knowledge Values Intention
Adapted Yes; two additional questions added to
the knowledge scale and two questions added to
the attitude scale
Yes, including the exclusion of 1 knowledge item
from original MMIC
No Yes Yes Yes Yes Yes Yes
Validated Yes, in previous studies No No Yes; knowledge questions were pilot tested on a low-literacy population before Yes No Yes No No
16 main trial Population 37 Midwives 982 Women in gestational weeks Women in gestational weeks 1-11 Women in early pregnancy consulting a General Practitioner
Men and Women between 55 and 64 years old with
low educational attainment, eligible for bowel
cancer screening
Men and Women members of target group for colorectal cancer screening Women 40 to 74 years old Women aged 70 to 71 years old who regularly participated in mammography screening Women aged 38 to 45 years old not previously diagnosed with breast cancer
Men and Women aged 50 to 74
years old
Mean Age 28.5 32.2 46.3 Not Reported 61 61.6 70 Not Reported Not Reported
Percent Informed Choice Combined visit n=203: 43.7% Separate visit n=223: 43.3% Intervention n=17 9: 71.5% Control n=197 : 62.4% Intervention n=165 : 76% Control n=165 : 65% Intervention n=357 : 34% Control n=172 : 12% Intervention n=785 : 44% Control n=792 : 12.8% Intervention n=383 : 53% Control n=102 : 6% Intervention n=3 51: 73.5% Control n=357: 48.8% Intervention n=9 1: 71% Control n=110: 64% Intervention n=1 34: 20.9% Control n=137: 5.8% Comparati ve Statistica Not reported χ2 p=0.062 2.08b (1.14-3.81) 22c p<0.001 31.2 (25.7-36.7); p<0.001d χ2 = 71.97 p<0.001 24.72c P<0.001 χ2 = 1.37 p=0.24 P<0.0001
*Randomized Controlled Trial
**Study not included in the Stacey, et al., 2017 Cochrane Systematic Review *** Down syndrome screening
a Difference between percentages of informed choice in intervention group vs. control group b Adjusted OR (95% CI)
c % difference
d % difference (99% CI); p-value
†Study did not retain the same item length found in the original MMIC, therefore, it cannot strictly be considered an adaptation or use of the MMIC; it did, however, measure informed choice using the 3-dimensional typology created by the original authors of the MMIC
17
4. Psychometrics
The field of psychometrics is the employment of different strategies to determine the validity and reliability of an assessment tool [46,47]. These assessment tools are designed with the express purpose of being measurement instruments for a particular domain; however, their measurement capabilities need to be validated. Psychometric testing allows researchers to validate tools they desire to use to draw unbiased information from people groups, devices, or organizations [46,47].
4.1 Psychometric testing in the health sciences
In the health sciences, questionnaires, tests, or surveys are widely used as assessment tools to measure an individual’s behavior, knowledge, or attitude (such as informed choice, anxiety, depression, or intent) as it pertains to their personal health or community health. In order for an assessment tool to be widely accepted, it must undergo extensive psychometric testing to establish that it is both reliable and valid for its specific area of use. Researchers evaluate the accuracy of the information included in their assessment tools (validity) and measure its overall constancy and stability (reliability) in obtaining consistently truthful responses after repeated use [48]. The two psychometric properties used to gage the performance of questionnaires are validity and reliability [48].
4.1.1 Validity
The validity of a questionnaire, test, or survey refers to how well and to what extent the content within each instruments reflects the chosen topic of interest; in other words, how well does the content within a questionnaire actually measure what it intends to measure [49–52].
There are numerous sub-concepts of validity such as external or internal validity (forms of experimental validity and not test validity) and several methods for establishing a questionnaire’s, test’s, or survey’s level of validity. This chapter will present and discuss: content validity and face validity.
18
4.1.1.1 Content validity
Content validity, as the name suggests, is the validation of a questionnaire’s content. The only way to establish content validity when there is no pre-established authority for a subject matter is through expert consensus [48,49]. Experts are used to validate the pertinence and suitability of each question included in a questionnaire, survey, or test by finding general consensus from their collective knowledge base [49].
The underlying notion in content validity testing is that each item in a questionnaire is taken from a larger pool of relevant items that can be used to assess a precise construct. Therefore, the items included in the questionnaire should represent a subset of relevant information from a larger collection of possible questions for that particular topic [48]. Experts are ultimately used to legitimize the subset of questions chosen to represent the overall construct. Finally, because there is no direct measure of content validity, it will always carry some subjectivity even though there is unanimity.
4.1.1.2 Face validity
An additional test of validity comes in the form of face validity. This topic is extremely controversial, as some researchers do not believe it to be a true source of validity testing and others believe it to be a useful component to validity. According to Mosier, 1947 [53], face validity has different forms. During the course of this study, face validity was employed as “appearance of validity.” Mosier describes appearance validity as the following:
“In this usage, the term “face validity” implies that a test which is to be used in a practical situation should, in addition to having pragmatic or statistical validity, appear practical, pertinent and related to the purpose of the test as well; i.e., it should not only be valid but it should also appear valid. This usage of the term assumes that “face validity” is not validity in any usual sense of the word but merely an additional attribute of the test which is highly desirable in certain situations [53].”
In this study, face validity was used to gage whether or not the tool created can be understood by the target population; is it indeed valid for the group of individuals by whom it will be used. This may include a range of factors from simplifying language to changing aesthetics of how the form is presented. There is concern among researchers that using face validity allows laymen, or those with little area expertise or knowledge, to have undue
19
influence over the content of a form, jeopardizing the content validity; however, face validity should not be seen as another form of content validity testing where instead of engaging experts, laymen are used to validate content. Face validity should simply serve as a method for identifying to what extent the entire test, questionnaire, or survey (content, structure, and aesthetics) is useable or understood by the study population.
For example, if a researcher creates a depression survey intended for use in a low-literacy population and includes long and weighty questions filled with medical jargon, instead of eliciting the necessary data for the project, study participants may not even be able to complete the survey because it is not tailored to their level of education. Studies such as Dormandy et al., 2007 [54] allude to the usefulness of creating assessment tools suitable for low-literacy populations and how the use of pictograms in place of lengthy questions increases comprehensibility [54]. If the researcher had done face validity testing on a small sample of the target population, it may have revealed the difficulty that that population has completing the survey. Participants would have been given the opportunity to express why they found it difficult and suggest changes to make it more “user-friendly” such as the incorporation of pictograms to facilitate comprehension.
4.1.2 Reliability
Reliability is the second property of psychometric testing. The reliability of any assessment tool refers to the degree to which it can generate consistent results on numerous administrations [47,48,55]. According to classical test theory, any score obtained from an individual (the observed score) is influenced by two notions: the true score and the error score. An observed score represents the value obtained by a study participant while the true score represents what the obtained value would have been with no error present. The error score includes random error and systematic error. Both random and systematic errors are collectively known as the measurement error [47,48,55].
Random errors, unlike systematic errors, affect a study haphazardly and fluctuate with every measurement causing them to influence observed scores in different ways. Systematic errors are stable and affect the observed scores consistently for each measurement. Though both are undesirable, no matter how well designed a study may be
20
there is bound to be some amount of systematic error because it cannot be entirely excluded, only reduced. This reduction in systematic error is most effective during the study design phase when there is a greater chance of eliminating misunderstandings and biases before study implementation.
Like validity, reliability contains a myriad of sub-concepts with several methods to its evaluation. For this project, five main methods of reliability testing will be presented and discussed: Internal Consistency (measured by Cronbach’s Coefficient Alpha), and Test-retest reliability measured using the Intraclass Correlation Coefficient (ICC), Cohen’s Kappa Coefficient (κ) and Weighted Kappa (κω).
4.1.2.1 Internal consistency
Disagreement exists concerning an accurate and universal definition for internal consistency as a psychometric property. Many definitions have been presented, published, and adapted; however, the debate over what internal consistency refers to within an assessment tool is not universal. For the purposes of this paper and the project, we use the definition by Schmitt which asserts that internal consistency is the interrelatedness of a set of items within a test [56].
Since internal consistency is the “interrelatedness” of a set of items, the goal of internal consistency testing is to quantify and understand to what extent items in an instrument correlate with one another. As explained earlier, validating content through expert consensus is founded on the notion that for each construct, there is a collective set of appropriate items possible to include within a tool. Content validation seeks to ensure that the chosen items for an instrument come from said pool and therefore reflect accurate and appropriate information for the topic and target audience. This would also suggest that any two items or more chosen from the larger pool of possible items should correlate well with one another because they all come from the same bank of questions for a construct. Measurements of internal consistency quantify this relationship between the items and allow researchers to establish the degree of the item correlation (inter-item correlation) [57].
21
4.1.2.2 Test-retest method
The test-retest method is often presented as a measure of internal consistency, when in all reality it is in fact more of an indicator of stability. Test-retest reliability measures the consistency of the tool overtime; in other words, the extent to which the tool can yield the same responses from the same individuals after a specified amount of time has elapsed between administrations [48]. If the administered form is reliable, the obtained scores should correlate even after time has passed because the scores are believed to represent the same true score for each individual [48]. Depending on the study and what needs to be measured, the chosen time interval of a test-retest varies from a few hours to several months. Nonetheless, Marx et al., 2003 found that there were no statistically significant differences in the test-retest reliability of two time intervals (2 days and 2 weeks) in their study that compared different test-retest times for health status instruments.
4.1.2.1.1 Cronbach’s coefficient alpha (α)
The most common measure used to evaluate internal consistency is Cronbach’s coefficient alpha. Briefly, Lee Cronbach created coefficient alpha in 1951 as a way of measuring the internal consistency of a scale or test that was not limited to items with dichotomous values. Alpha corresponds to a number between 0 and 1[58,59]. Unlike other reliability indexes, alpha does not necessitate two administrations of the scale it is testing and therefore, offers more flexibility for researchers and study design.
22
Cronbach’s alpha was also not the first measure of internal consistency. The earliest method was the split-half method by William Brown in 1910. This method of measuring internal consistency requires the researcher to “split” the test in half (for example, all the odd numbered items vs. the even numbered items or the top half vs. the bottom half) and calculate the degree of correlation between both halves. The clear flaw in using the
split-half method is that any instrument with several items can have over 100 or even 200 possible combinations and each would yield a significantly different correlation score [57]. Furthermore, dividing an instrument in half decreases its length by 50%, which will in turn underestimate the strength of its reliability [57]. In 1937, researchers Kuder and Richardson proposed a new measure of internal consistency called the KR-20 to compensate for the uncertainty found in the split-half methods [60]. In the KR-20 equation
n represents the number of items, pk is the proportion of individuals who answered item k
correctly, qk are the number of individuals who responded incorrectly to item k, and Vtest
represents the variance of the total scores [60]. Therefore, KR-20 can be seen as providing a mean score for all the possible split-half pairings, a trait which coefficient alpha also maintains.
Although, it was an improvement on the spit-half method, KR-20 is limited to dichotomous items, for which Cronbach found a solution with the coefficient alpha. Coefficient alpha’s equation is: Equation 1 : KR-20 equation 𝛼 = 𝑛 𝑛 − 1(1 − ∑ 𝑝𝑘𝑞𝑘 𝑉𝑡𝑒𝑠𝑡 ) (1)
Equation 2 : Cronbach’s coefficient alpha equation 𝛼 = 𝑛
𝑛 − 1(1 −
∑ 𝑉𝑖𝑡𝑒𝑚 𝑉𝑡𝑒𝑠𝑡 )
23
where n is the number of items, Vitem is the sum of all the item variances and Vtest is the variance of the total scores [58].
When using coefficient alpha, researchers should consider several essential truths about alpha’s characteristics. Firstly, Cronbach’s alpha is not a measure of validity. It is strictly used to measure the internal consistency of items in an instrument, so it is a measure of reliability. It can be used with continuous data, setting it apart from other measures of internal consistency such as split-half and KR-20. Thirdly, as equation 2 demonstrates, alpha is a function of the number of items in the instrument it is measuring; as you increase the number of items, you are also artificially increasing your alpha. Therefore, a high coefficient alpha may not necessarily be due to items that are highly correlated but rather to having too many items in a questionnaire, test, or survey. If alpha is unusually high, an issue of redundancy may exist within the scale. Finally, as with all reliability tests, the scores obtained from alpha are reflective of the population in which they were calculated and not of the instrument itself because “a scale may have excellent reliability with one group and only marginal reliability in another” [57].
Several studies suggest standard cut-offs for alpha. Primarily, an acceptable alpha can range between 0.70 and 0.90 depending on the study and the design of the instrument [61]. Scores higher than .90 bring into question the possibility of redundancy within a scale and therefore, the need to remove repetitive questions if item length is adequate.
4.1.2.1.2 Intraclass correlation coefficient (ICC)
The intraclass correlation coefficient (ICC) is another statistical test of internal consistency that evaluates test-retest reliability by measuring inter(intra)-rater reliability. There is no universal definition for ICC because each ICC coefficient corresponds to a specific estimate depending on if the calculations are for a sample or population and if what is being rated is consistent for all raters. The intraclass correlation coefficient will be explained in light of the fact that SPSS was used for all calculations of ICC in this project. There are six different coefficients generated by SPSS. Each is either one-way random or two-way random measurement. One-way random refers to the fact that the calculation does not
24
differentiate between the rater and the ratee, seeing both as having one effect and that the ratings come from a population rather than a sample [62]. In a two-way random calculation it is also assumed that the ratings come from a population, however, this time, two effects are calculated for the rater and the ratee, separately [62].
“Two-way Random” or “ICC 2” was used to measure our test-retest reliability because it “assumes that the mean rater error =0” and calculates the intra-rater mean to provide a measure of consistency rather than a measure of absolute agreement [62].
4.1.2.2 Cohen’s kappa coefficient (κ)
Cohen’s Kappa Coefficient (κ) is a measure of reliability used for interrater or intra-rater agreement testing for nominal scales [63]. Testing of interrater agreement estimates the level of reliability among several raters evaluating the same events. For example, interrater reliability would be measured if three radiologists assessed 50 different x-rays and a researcher needed to know to what extent their appraisals match; the level of agreement among the three raters. Intra-rater reliability measures the level of agreement of the values given to several events by the same rater. Researchers would measure intra-rater reliability, for example, among 12 participants of a study who answered 20 of the same questions at four different times. In this example, each of the 12 participants answered a total of 80 questions and researchers now want to know the extent to which each individual’s responses are consistent (reliable) in how they answered the same questions four different times. They would use intra-rater reliability because they want to know the level of agreement within the responses of a single individual [64].
There are several methods used to measure rater agreement but most are limited in use by the number of raters or ratings employed for them to be accurate reliability estimates. Before the introduction of Cohen’s Kappa, there was no reliability measure that corrected estimates for chance. The most common way of assessing agreement was by simply calculating the percent agreement between or within raters without taking into account the amount of agreement that existed simply due to chance. In 1960, however, Jacob Cohen introduced kappa as a statistic able to mathematically account for the agreement reached between or within raters due to chance [63, 64].
25 Cohen’s Kappa equation is as follows:
where 𝑝𝑜 is the proportion of observed agreement and 𝑝𝑒 is the proportion of expected agreement due to chance [63].
Interrater reliability measures to what extent raters assign the same value to the same variables in an assessment tool. Agreement between individuals charged with “scoring” items becomes extremely important in healthcare when we consider that healthcare practitioners are used to evaluate X-Rays, CT scan images, or Pap smear results which all require subjective consensus among trained practitioners [64]. In the course of this study, Kappa is used to measure intra-rater reliability among participants of a test-retest.
4.1.2.3 Weighted kappa (κω)
Although, Cohen’s kappa coefficient corrects for chance, in a rater matrix, “it treats all disagreement cells the same”. This can be problematic for a researcher or for a study where a disagreement between two variables being measured is much more severe than disagreement between another two variables being considered; that is kappa does not take into account possible “partial” agreements that may be present in an ordinal scale. Therefore, Cohen modified his kappa coefficient to create weighted kappa (κω), “a chance-corrected proportion of weighted agreement” [65]. In this study, weighted kappa is used to measure the attitude Likert scales of both questionnaires.
Equation 3 : Cohen’s kappa equation
𝜅 =𝑝𝑜− 𝑝𝑒 1 − 𝑝𝑜
26
5. Adaptation and Validation of the Multi-Dimensional Measure
of Informed Choice to Cardiopulmonary Resuscitation and
Mechanical Ventilation in an Elderly French-Canadian
Population
Rebecca Francois1,3,4, France Légaré2,5,6, Patrick Plante7, Emmanuelle Belanger8, 9, Holly O. Witteman1,2, Alexis F. Turgeon10,11, Tom van de Belt12, Patrick M Archambault1, 2, 3, 4, 10, 11
1
Université Laval, Québec, QC, Canada
2 Département de médecine de famille et médecine d’urgence, Université Laval, Québec, QC,
Canada
3 Centre de recherche de Centre intégré en santé et services sociaux de Chaudière-Appalaches
(Hôtel-Dieu de Lévis)
4 Centre intégré en santé et services sociaux de Chaudière-Appalaches, (Hôtel-Dieu de Lévis),
Lévis, QC, Canada
5
CIUSSS de la Capitale Nationale, Québec, QC, Canada
6 Centre de recherche du CHU de Québec –Université Laval, Axe santé des populations et
pratiques optimales en santé, Québec, QC, Canada
7 Université TÉLUQ, Québec, QC, Canada 8
Brown University School of Public Health, Providence, RI, USA
9 Center for Gerontology and Healthcare Research, Department of Health Services, Policy &
Practice
10
CHU de Québec – Université Laval Research Centre, Population Health and Optimal Health Practices Research Unit (Trauma-Emergency-Critical Care Medicine), Université Laval, Québec, QC, Canada
11 Department of Anesthesiology and Critical Care Medicine, Division of Critical Care
Medicine, Université Laval, Québec, QC, Canada
12
Radboudumc Reshape Innovation Center, Radboud university medical center, Nijmegen, The Netherlands
27
5.1 Résumé
Objectif: Adapter et valider le Multidimensional Measure of Informed Choice (MMIC) à la
réanimation cardiorespiratoire (RCR) et la ventilation mécanique invasive (VMI) auprès des aînés aux soins intensifs.
Méthodes: Adaptation et validation du MMIC à la RCR et la VMI en trois phases: la
validité du contenu, la validité apparente, et fiabilité test-retest à une semaine.
Résultats: Neuf experts ont participé à la validité de contenu. Dix patients ont participé à la
validité apparente. Trente-deux aînés en résidence ont participé au test-retest. Le Kappa indique un item de connaissance non reproductible pour la RCR (κ=.36) et deux items de connaissance non reproductibles pour la VMI (κ=.14 and 0). La cohérence interne des items d’attitude est élevée (α > 0.90).
Conclusion: Chaque questionnaire a été adapté pour une population
Canadienne-francophone. Les construits de connaissance étaient fidèles après une semaine. Au niveau d’item, trois n’ont pas montré une fiabilité intra-évaluateur. L’attitude pour la RCR n’était pas stable.
Mots clés: Validation • fiabilité • la réanimation cardiorespiratoire • la ventilation
mécanique invasive • fin de vie • MMIC • la prise de décision éclairées • la consentement éclairées • la prise de décision partagée
28 5.1.1 Abstract
Objective: To adapt and validate a questionnaire to cardiopulmonary resuscitation (CPR)
and invasive mechanical ventilation (IMV) in an elderly Canadian intensive care unit (ICU) population.
Methods: Mixed-method study that adapted and validated the 9-item multi-dimensional
measure of informed choice (MMIC) to CPR and IMV in 3 phases: content validity, face validity, and a test-retest at 1-week. Intraclass correlation (ICC) measured temporal stability of both knowledge and attitude constructs, and coefficient alpha measured internal consistency of the attitude items.
Results: Two adapted questionnaires with validated content by nine experts for CPR and
IMV. Thirty-two residents participated in the test-retest at 1 week. Kappa revealed one unstable knowledge item for CPR (κ=.36) and two unstable knowledge items for IMV (κ=.14 and 0). Overall knowledge constructs for CPR and IMV were stable (p=0.08 and
p=0.84, respectively). CPR attitude construct was not stable (p=0.01).Internal consistency for the attitude items was high (α > 0.90).
Conclusion: Each questionnaire was adapted to CPR and IMV for a French-Canadian
population. Both questionnaire knowledge constructs were reliable after re-administration but at the item level, three items did not show intrarater agreement. CPR attitude construct was not stable.
Practice Implications: More work is needed to adapt the MMIC for decision making in
ICUs.
Keywords: Validation • reliability • cardiopulmonary resuscitation • invasive mechanical
ventilation • end-of-life • MMIC • informed choice • informed consent • shared decision making
29
5.2 Introduction
Two potentially overused life-sustaining interventions at end-of-life (EOL) for elderly Canadians are cardiopulmonary resuscitation (CPR) and invasive mechanical ventilation (IMV) [1,2]. Studies indicate that up to as many as 72% of elderly patients are receiving these aggressive interventions at EOL, which may be care inconsistent with their personal values and preferences [1,3–6]. Studies also suggest that the overuse of both interventions stems from a lack of patient knowledge about outcomes, the risks and benefits of these medical procedures as well as from failure to have patient values clarified, preferences expressed and, when stated, accurately documented in their medical charts [1,4,5,7–9]. One of the ways to bridge the divide that exists between patient preferences and the actual care they receive is by helping patients make informed decisions through shared decision making (SDM) [10,11]. Shared decision making is a decisional model where the patient and the physician work together to arrive at a final decision about an intervention or diagnostic test, that not only appreciates the evidence put forth by an expert clinician or a care team, but also considers the patient’s values and preferences concerning the options [12–15].
In so doing, shared decision making increases patient knowledge and informs their decisions, which has been known to lead to higher patient satisfaction, better health outcomes, the more appropriate use of medical interventions, less medical errors, less litigation, and even reduced healthcare costs [16–19]. However, few studies have evaluated if shared decision making leads to informed decisions by patients and/or surrogate decision makers when facing decisions about whether or not to use life support in the intensive care unit [20]. Moreover, there currently is no validated instrument to measure informed decision making about life sustaining interventions in the intensive care unit.
The multidimensional measure of informed choice (MMIC) is an assessment tool used to measure the congruence between a patient’s knowledge, attitude, and uptake [21]. Originally developed to measure informed choice about prenatal Down syndrome screening, the MMIC is based off of the O’Connor and Pallas definition of an “effective decision” [22]. An informed choice to undergo an intervention occurs when an individual