THE MULTISYSTEMIC BURDEN OF CHRONIC
OBSTRUCTIVE PULMONARY DISEASE: A
LONGITUDINAL STUDY
Mémoire présenté
à la Faculté des études supérieures de l'Université Laval dans le cadre du programme de maîtrise en Médecine Expérimentale
pour l'obtention du grade de Maître es Sciences (M.Sc.)
FACULTE DE MEDECINE UNIVERSITÉ LAVAL
QUÉBEC
2010
La MPOC est une maladie chronique, mais évitable et traitable, en expansion et dont la principale cause est le tabagisme.
Contrairement à ce que nous avons l'habitude de penser, la MPOC n'est pas seulement une maladie pulmonaire, mais également une maladie qui entraîne des changements dans des nombreux organes et systèmes. Beaucoup de recherches ont été effectuées dans ce domaine et il semble que l'inflammation est le lien entre les manifestations au niveau pulmonaire et ceux au niveau systémique comme la perte de poids, la perte de masse musculaire, et la diminution de la qualité de vie.
Dans mon projet, on s'est intéressé à l'obésité associée à la MPOC et à son rôle protecteur sur la survie comme le suggère le "paradoxe de l'obésité". Effectivement, dans la cohorte que j'ai suivi de façon prospective, les patients avec un index de masse corporelle (IMC) supérieur à 25 kg/m2 ont eu une meilleure survie que ceux ayant un faible IMC
(moins de 25 kg/m2). Après voir corrigé les courbes de survie pour les facteurs
confondants les plus significatifs, nous avons été en mesure de démontrer que cet effet protecteur d'un IMC supérieur n'était pas dû à la pure accumulation de masse graisse, mais davantage à une moindre gravité de la maladie, à une meilleure capacité à l'effort et à une
■y
Abstract
COPD is a chronic but preventable and treatable disease directly related to smoking and whose prevalence continues to progress. COPD is now a major burden for healthcare systems throughout the world.
Contrary to traditional thinking, COPD is not just a lung disease as it involves many extrapulmonary organs and systems. Much research has been performed in this area and inflammation could be the link between the lung disease and its systemic manifestations like body weight loss, muscle wasting, and diminished quality of life.
My project was essentially focused on the obesity associated to COPD and its protective role on the survival as reflected in the "obesity paradox". In the cohort I followed prospectively, patients with higher body mass index (BMI) (over 25 kg/m2) had indeed a
better survival than those with low BMI (less than 25 kg/m2). After correcting the survival
curves for significant confounding factors, we were able to show that this protective effect of a higher BMI was not due to pure fat accumulation but much more to a lesser disease severity, a better exercise capacity and a higher muscle mass in the patients with BMI values over 25 kg/m2.
Avant-Propos
Life is tough. That's what I've learned throughout my existence. But life is also great when things turn out the way we want them to. So I am more than happy to sit here in front of my computer and express my feelings of gratitude towards all those wonderful people that helped me along this beautiful and exciting journey in the world of medical research.
When Dr. Maltais kindly accepted to guide my first steps through the world of clinical research, I new there will be days of joy and days of hard work coming, but I did not know that I was also winning a family by joining this wonderful team. I want to thank my research director Dr. François Maltais for his help and good advices, who made it all possible. I also want to thank my co-director Dr. Yves Laçasse, the study nurses Marthe Bélanger, Brigitte Jean, Josée Picard and especially Marie-Josée Breton who I have constantly "harassed" with my questions. I also thank to Micheline Paquin, Sarah Bernard Marie-Eve Paré and Annie Michaud for sustaining me in my research projects. I also would like to thank: Karine Marquis, Mariève Doucet, Louis Laviolette, Didier Saey, Véronique Pépin, and Richard Débigaré for their good and friendly advices and for their fore-work on the data that I used in my research.
I wish to thank my husband for always standing by me, for his constant encouragements and patience. I also thank my parents for their support. And above everything, I owe it all to my son Henry Wayne who made everything worthwhile.
Table of contents
RÉSUMÉ Il ABSTRACT Ill AVANT-PROPOS IV TABLE OF CONTENTS VI
LIST OF ABBREVIATIONS VIM
LIST OF TABLES IX LIST OF FIGURES X INTRODUCTION 11 CHAPTER 1 : ABOUT CHRONIC OBSTRUCTIVE PULMONARY DISEASE 13
Summary 13 Definitions 14 Disease severity and classification of COPD 16
Epidemiology 17 Aetiology and risk factors 18
Pathophysiology 19 a. Intraluminal factors 20
b. Factors within the bronchial wall 20 c. Abnormalities of peribronchial tissue 21 d. Abnormalities of the pulmonary vascular system 22
Clinical presentation and comorbidities 22
Clinical evaluation 24 a. Medical history 24 b. Physical examination 24
Investigation 25 a. Spirometry 25
b. Other tests 25 Treatment 26 a. Smoking cessation 26 b. Pharmacological treatment 26 c. Non-pharmacological therapy 28 Follow-up 30 Natural history and prognostic factors 30
CHAPTER 2: NUTRITIONAL PROBLEMS IN COPD 35
Summary 35 Body weight loss and its prognosis in COPD 36
Obesity in COPD: a new reality 37 a. Obesity-associated health concerns 38
b. The obesity paradox 39 CHAPTER 3: HYPOTHESES 41
CHAPTER 4: OBJECTIVES AND METHODOLOGY 42
CHAPTER 5: ARTICLE SCIENTIFIQUE 43
Abstract 44 Introduction 45 Material and methods 46
Statistical analysis 48
Results 49 Discussion 51 References: 55 CHAPTER 6: CONCLUSION, PERSPECTIVE 64
List of Abbreviations
FVC FEV, LTOT COPD Pa02 PaC02 mmHg Sa02 MTCSACT BMI ATS ERS PEV RRForced vital capacity
Forced expiratory volume in one second Long-term oxygen therapy
Chronic obstructive pulmonary disease The pressure of oxygen in arterial blood
The pressure of carbon bioxide in arterial blood Millimetres of mercury
Oxygen saturation
Midthigh muscle cross sectional area Body mass index
American Thoracic Society European Respiratory Society Proportion of explained variation Estimated relative risks
List of tables
TABLE 1 - SUBJECTS CHARACTERISTICS ACCORDING TO THE BMI* 57
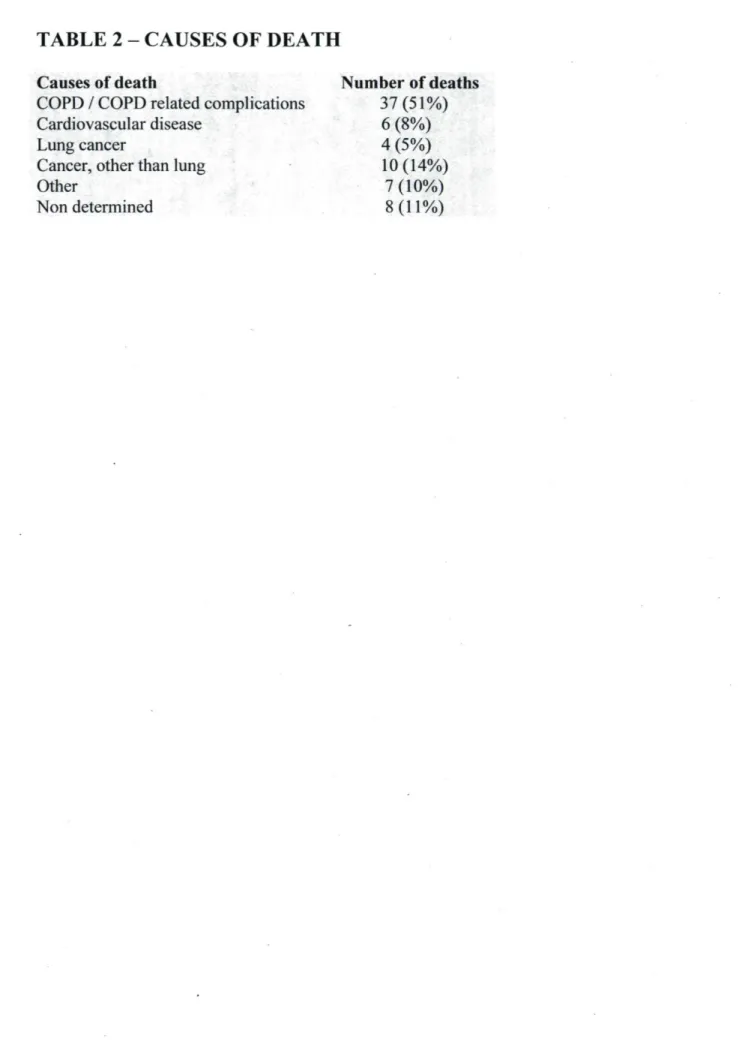
TABLE 2 - CAUSES OF DEATH 58 TABLE 3 - SUBJECTS CHARACTERISTICS ACCORDING TO THE SURVIVAL
STATUS* 59 TABLE 4 - DETERMINATION OF IMPORTANT VARIABLES TO EXPLAIN
MORTALITY: UNIVARIATE ANALYSIS 60 TABLE 5 - DETERMINATION OF IMPORTANT VARIABLES TO EXPLAIN
MORTALITY - MULTIVARIATE ANALYSIS 61 TABLE 6 - CLASSIFICATION OF COPD SEVERITY ACCORDING TO THE
ATS/ERS AND GOLD 67 TABLE 7 - THE MEDICAL RESEARCH COUNCIL DYSPNEA SCALE 68
FIGURE A -VENN DIAGRAMS DEPICTING THE SUBSETS OF DISEASE THAT COMPOSE CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) AND
THE RELATIONSHIPS BETWEEN THEM 15 FIGURE B - RISKS OF MORTALITY FOR VARIOUS MEN IF THEY SMOKE AND
THE EFFECTS THAT SMOKING AND STOPPING SMOKING CAN HAVE ON
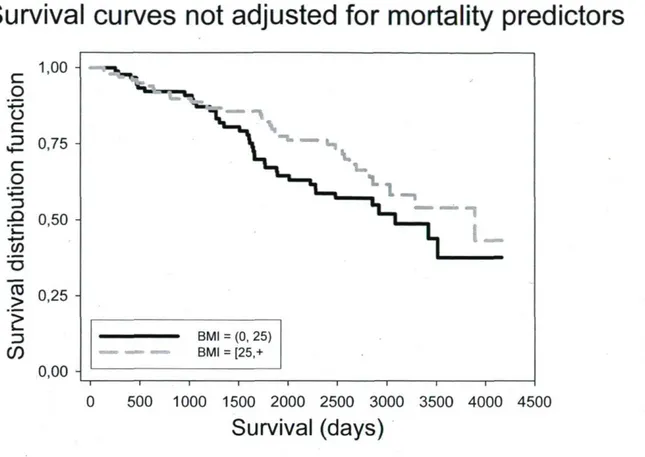
FEV. 19 FIGURE 1 - SURVIVAL CURVES FOR THE TWO BMI GROUPS, NOT
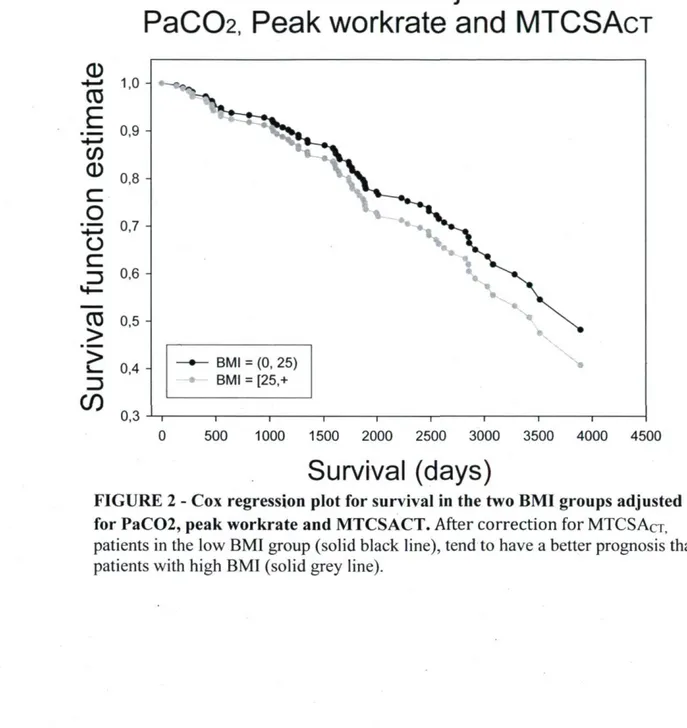
ADJUSTED FOR MORTALITY PREDICTORS 62 FIGURE 2 - COX REGRESSION PLOT FOR SURVIVAL IN THE TWO BMI
Emphysema and chronic bronchitis have afflicted humanity from ancient times. In 1679 Theofile Bonet described the "voluminous lungs" characteristic for emphysema, followed by Giovanni Battista Morgagni who also described 19 cases of patients with "turgid" lungs. As Laënec so beautifully illustrated, the lungs of the patients suffering from emphysema were hyperinflated and did not empty well. He also noted the mucus fluid filling the trachea and the bronchi1.
In our days, chronic bronchitis and emphysema are jointly named chronic obstructive pulmonary disease (COPD) and smoking is recognised as by far the most
-y
important étiologie factor of this condition . Alarmingly, COPD is becoming a global health epidemic. Even though a "preventable and treatable disease" as characterized by ATS/ERS Task Force3, it is predicted to advance from the sixth to the third commonest
cause of death worldwide in 2020 and to become the fifth most common cause of chronic disability worldwide by 20204.
COPD is characterized by progressive airflow limitation associated with abnormal inflammatory response that leads to the destruction of lung parenchyma, narrowing of small airways and lost of elastic recoil. Besides progressive airflow limitation, air trapping and progressive shortness of breath, COPD has also significant systemic repercussions3,4 like
increased oxidative stress, increased plasma levels of proinflammatory cytokines and circulating inflammatory cells, weight loss, skeletal muscle dysfunction, coronary artery disease, endothelial dysfunction, depression, altered autonomic nervous system and bioenergetic metabolism of the brain and high prevalence of osteoporosis5.
This work opens with an overview of COPD. The first chapter defines the disease and presents its classification, epidemiology, étiologie and risk factors and pathophysiology. Patient-oriented aspects like clinical presentation and evaluation, investigation, differential diagnosis, prevention, treatment, follow-up and prognostic factors are discussed.
The second chapter offers an overview of the systemic effects of chronic obstructive disease as presented in the scientific literature.
The third and the forth chapter present the objectives and the hypotheses of the present work.
The fifth chapter addresses one of the COPD co-morbidities: obesity. Even though the "classic" medicine teaches us that obesity is a risk factor for many diseases and it shortens life expectancy, in recent years, the so-called "obesity paradox" is gaining more and more attention. Overweight and obesity have been shown to be associated with longer survival in chronically ill patients with chronic heart failure and kidney disease undergoing maintenance dialysis '7. On the other hand, it is now well-known that weight loss is
associated with increased mortality in COPD patients8"10. As it is unclear whether this
positive association between body weight and survival is due to fat accumulation or to confounding factors, we investigated in a cohort of 190 subjects if being fatter is really a better option in COPD patients. This chapter represents an original article that will be presented for publication to a scientific journal.
COPD is a slowly progressing disease that not only compromises the lungs but also extends to several other important organ systems. Recognising the multisystemic character of the disease and the way the natural history and the clinical features interact, will allow a better understanding of COPD, improved prevention for its related systemic manifestations and hopefully a more effective therapeutic approach.
Chapter 1: About chronic obstructive pulmonary disease
Summary
COPD is a chronic disease reaching epidemic proportion among the population. The main étiologie factor is smoking, which entertains a chronic state of inflammation and over the years results in the destruction of lungs parenchyma (emphysema) and/or chronic airflow obstruction and airway secretion production (bronchitis).
Patients suffering from COPD often present late in the disease course and their principal symptom is dyspnea. The clinical evaluation is based on spirometry and disease staging is traditionally based on forced expiratory volume at 1 second (FEVi). Since numerous studies have revealed the multisystemic character of COPD and the importance of comorbidities, more complex tools are needed for a more complete and more realistic evaluation of these patients.
Even though COPD is characterized by a continuous and faster decline of lung function than seen by aging alone, smoking cessation is always worth since it is the only intervention that can slow down the progressive decline in lung function.
Definitions
As described by the American Thoracic Society/European Respiratory Society ATS*/ERS* and Global Initiative on Obstructive Lung Disease (GOLD)*, COPD is a preventable and treatable disease state characterized by airflow obstruction that is not fully reversible. The airflow limitation is due to chronic bronchitis or emphysema and it is generally progressive, sometimes accompanied by airway hyperreactivity and an abnormal inflammatory response triggered by noxious particles or gases, mostly cigarette smoking. Although primary a lung disease, it also produces significant systemic consequences3'"'12.
Chronic bronchitis is a clinical diagnosis, defined by the presence of chronic productive cough for 3 months in each of two successive years in a patient in whom other causes of chronic cough have been ruled out.
Emphysema is a pathologic diagnosis characterised by abnormal permanent enlargement of the airspaces distal to the terminal bronchioles with destruction of their walls and without obvious fibrosis ' .
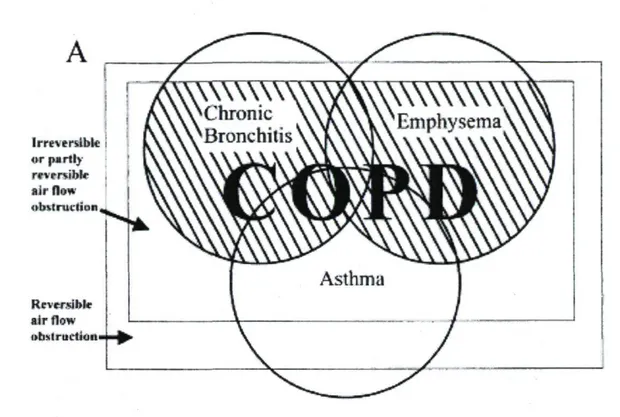
The ATS/ERS consider asthma a different clinical entity view its different pathogenesis and response to therapy compared to COPD. Asthma patients with poorly reversible airflow limitation should be treated as asthma even though they might be indistinguishable from COPD patients (See figure A).
* ATS : American Thoracic Society * ERS: European Respiratory Society
I r r e . e r s i b l . o r pu rt I v rfvrrw-.H. air now ubitruclion RcvctaM. air flew ubslruirlicil.
Figure A - Venn diagrams depicting the subsets of disease that compose chronic obstructive pulmonary disease (COPD) and the relationships between them. The picture above shows the modified version of the American Thoracic Society's COPD definition.
Disease severity and classification of COPD
The hallmark of COPD is airflow limitation that is not fully reversible. In patients showing symptoms of cough, sputum production and dyspnea or having a history of exposure to COPD risk factors, a forced expiratory volume in one second (FEVi) / forced vital capacity (FVC) < 70% confirms the presence of the disease.
Both ATS/ERS and GOLD have proposed a classification into four stages, based on post-bronchodilator FEVi and theFEV|/FVC ratio (see table 6).
Stage I refers to subjects with mild COPD, in whom the airflow limitation begins to show in spirometry results (FEVi/FVC <70% with FEV| > 80% predicted). The attended persons might not even by aware their lung function is abnormal at this stage and chronic cough and sputum production are not always present.
Stage II represents moderate COPD. At this stage, airflow limitation is worsening (FEVi between 50 and 80 % predicted) and the symptoms progression especially on exertion determines the patients to seek medical attention.
Patients with Stage III, severe COPD experience increased shortness of breath and repeated exacerbations. Spirometry shows a pronounced airflow limitation: FEVi between 30 to 50% predicted.
Stage IV represents the patients with very severe COPD, to whom exacerbations may be life-threatening and quality of life is seriously impaired. FEVi drops below 30% in these patients and chronic respiratory failure may be present".
Even though this classification is convenient for educational reasons, a staging system offering a more complete image over the health status and disease severity would allow a more objective evaluation of the COPD patients.
The grading of breathlessness is associated with survival in patients with COPD. It can be assessed by the Medical Research Council (MRC) dyspnea scale. This scale ranges from
0 to 4, with 0 indicating shortness of breath occurring only with strenuous exercise and 4 indicating the patient is too breathless to leave the house (see table 7).
Celli et al. developed the so-called BODE index whose scoring system is calculated from BMI, the degree of airflow obstruction (FEVi) and dyspnea (MRC dyspnea score) and the exercise capacity (distance in meters walked in 6 minutes). The BODE index is ranged from 0 to 10 points, a higher score indicating worse disease, and it has been shown to be a better predictor of all-cause mortality than FEVi among COPD patients14.
Epidemiology
The prevalence of COPD is difficult to estimate as it varies a lot depending on the definitions used. The extent to which COPD is a cause of death is probably underestimated too, as it is difficult to attribute death to a single cause in COPD patients. Also, in mortality databases, many COPD-related deaths are falsely attributed to other causes such as congestive heart failure or pneumonia12'15' . Both healthcare providers and patients tend to
underestimate the morbidity of COPD and the disease is usually diagnosed first when clinically apparent and already moderately advanced2;3. The 2005 Canadian Community
Health Survey found that 4.4% of the Canadians aged 35 years or older had COPD based on self-reported diagnoses. The prevalence among men was 3.9% and 4.8% among women15.
COPD is currently the fourth leading cause of death in the United States and Canada and its incidence is increasing. World Health Organisation (WHO) predicts that by 2020 COPD will rise to be the 5th most prevalent disease worldwide and the 3rd most common
cause of death17. Alarming is also the new trend of growing mortality due to COPD among
women, which has doubled in the last 20 years .
COPD patients are very expensive for the society with the costs per Canadian
1..
Aetiology and risk factors
Tobacco smoking is the most important cause of COPD accounting for 80% of the risk of developing COPD and it is associated with a 2 to 20 fold increase in the risk of death from COPD. The rate of decline in lung function strongly correlates with smoking and with the amount smoked.
Since only 15-30% of active cigarette smokers develop COPD and never smoker account for 23% of COPD patients, there are other risk factors besides smoking to consider. There is evidence that points to interactions with environmental factors and a genetic predisposition to COPD.
Increased airway responsiveness and allergic phénotype predict an accelerated decline in lung function, which makes it an important COPD risk factor19.
Occupational exposure to environmental dust as seen in gold and coal miners and occupational exposure to organic antigens like in the case of agricultural workers are also common causes of COPD.
Deficiency of antioxidant vitamins (C and E) might permit tissue destruction because of lack of host defence against oxidative stress.
Genetic certainly plays a role in COPD development. The most investigated until now is the alpha-1-antitrypsin deficiency leading to an excess in neutrophil elastase and development of premature emphysema. Gene polymorphisms for tumor necrosis factor alpha (TNF-a), microsomal epoxide hydrolase, gluthathione S-transferase PI and transforming growth factor beta 1 have been associated with COPD development19.
The dysregulation of matrix metalloproteinases (MMPs) and of their tissue inhibitors (TIMPs) has also been associated to COPD development and is currently under investigation as a potentially new treatment target19.
Low birth weight and recurrent infections during childhood and adolescence translate into diminished peak value in early adulthood so that the normal aging-related decline in lung function starts from a lower peak value.
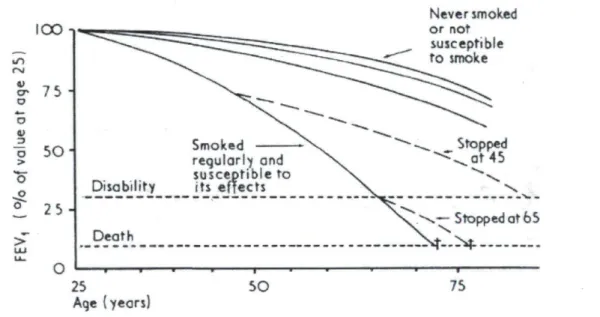
In terms of risk reduction, smoking cessation is certainly one very effective intervention. There is strong evidence that smoking cessation reverse the accelerated decline in lung function even though the lost FEVi will not be recovered20 (see fig. B) and
smoking cessation programs can lead to significant reduction in all-cause mortality in people with mild to moderate airway obstruction , as the Lung Health Study (LHS) trial has
? I *
shown" . Physical activity might help reduce lung function decline in active smokers and anti-inflammatory therapy is an interesting option still under investigation ' ' ' .
I O O I r. V cr O - H - H o 3 a > C» o o 75 -5 0 " 25 O Disability Death 25 Age {years} Smoked regularly and susceptible to its «fleets SO Never smoked or not susceptible to smoke Stopped at 65 75
Figure B - Risks of mortality for various men if they smoke and the effects that smoking and stopping smoking can have on FEVi
t=Death of irreversible chronic obstructive lung disease Adapted from Fletcher C, British Medical Journal, 197720
Pathophysiology
The defining characteristic of COPD is the airflow limitation due to bronchial obstruction. This is best measured by FEVi and FVC decrease. A decrease in the FEVi to FVC ratio can be the first sign of airflow limitation23.
a. Intraluminal factors
There is a chronic inflammation in the COPD and histological studies showed that most of it occurs in the peripheral airways (bronchioles) and lung parenchyma. The bronchial epithelium is infiltrated by macrophages, neutrophils and T-lymphocytes, predominantly CD8+ (cytotoxic) T cells. Cigarette smoke and other irritants stimulate the secretion of neutrophils-chemotactic factors like interleukin-8 and leukotriene B4 in the macrophages, so consequently more neutrophils are attracted in this cascade. Neutrophils and macrophages release multiple proteinases (neutrophil elastase, cathepsins, matrix metalloproteinases) who stimulate mucus secretion in the enlarged mucus secreting glands. A typical finding in chronic bronchitis is the goblet cell metaplasia with an elevated Reid index*.
Ciliated epithelial cells undergo squamous metaplasia, so that mucociliary clearance mechanisms are impaired. The result of these changes is an increase in airway secretions, defining chronic bronchitis but also seen in emphysematous patients. The secretions can form mucous plugs and obstruct the airflow, especially during exacerbations ' .
b. Factors within the bronchial wall
Since airways are exposed to a variety of inhaled toxins and pathogens, good repair mechanisms are important to restore the damaged epithelium and its functions. Generally, after airway mechanical injury, plasma proteins exudates onto the airway surface and polymerize to form a provisory matrix. Epithelial cells migrate from the edge of the wound to cover the epithelial defect and then differentiate into columnar cells with cilia and secretory granules. Although not completely understood, this repair process is regulated by a variety of chemotactic and growth factors like fibronectin and TGF-p.
Repair processes may fail to restore normal epithelial architecture and lead to tissue remodeling resulting in altered structure and function. Epithelial cells release factors that enable fibroblast recruitment and proliferation. Connective tissue is deposited in the
subepithelium and adventitia. Like any other scar, this peribronchiolar fibrotic tissue contracts and leads to the fixed airway obstruction characteristic for COPD and increases airway resistance. Hogg et al. observed a strong association between COPD progression and thickening of the airway wall following airway remodelling. Major sites of airflow limitation in COPD are the small airways, including bronchi and bronchioles less than 2 mm in internal diameter.
The airway smooth muscles become hypertrophied and hyperreactive as a consequence of the ongoing inflammation. The bronchoconstriction together with the airway wall oedema, inflammatory cell infiltration and the glandular hypertrophy may be responsible for the slight reversible airflow limitation we can ameliorate with treatment ' " .
c. Abnormalities of peribronchial tissue
The inflammation stimulates the secretion of proteases like neutrophil elastase, proteinase 3, cathepsins and matrix metalloproteinases. They can break down connective-tissue components, especially elastin, destroy the lung parenchyma and produce emphysema. Smokers who develop COPD seem to have lower levels of antiproteases (ai-antitrypsin, tissue inhibitors of matrix metalloproteinases) so the effects of the proteases are not efficiently neutralized. Cigarette smoke aggravates this imbalance by the means of oxidative stress pathway who damages antiproteases such as cti -antitrypsin and thus amplify proteolytic injury17. Smokers typically develop the so called centrilobular
emphysema that involves the center of the secondary lobule in the upper pulmonary lobes. The panacinar emphysema is due to congenital ai-antitrypsin deficiency (inhibitor of the neutrophil elastase) and touches upon the entire alveolus, predominantly in the lower half of the lungs26;3°.
In the healthy lung, the alveolar septa exert a radial traction force to the outer wall of the peripheral airways permitting the expansion of the airway diameter. In emphysema,
* The ratio of the thickness of the mucous gland layer to the thickness of the wall between the epithelium and cartilage is known as the Reid Index. A normal Reid index is less than 0.4 and is increased in chronic
destruction of these alveolar attachments diminishes the airway wall support and leads to narrowing of the lumen and increased resistance ' .
On the other hand, the emphysematous destruction of lung parenchyma is associated with loss of elastic recoil of the lung. The result is very compressible airways and marked increases in airway resistance .
d. Abnormalities of the pulmonary vascular system
In the pulmonary arteries, T lymphocytes (especially CD8+) invade the adventitia. It
seems that cytokines and growth factors released by inflammatory cells are responsible for remodeling of the arterial wall and impairment of the endothelial function. The internal diameter of blood vessels decreases following the proliferation of smooth muscle cells in the intima and also the deposit of collagen and elastic fibers in the wall. Remodeling of the arterial walls, endothelial dysfunction with reduced expression of endothelial nitric oxide synthase (eNOS), hypoxic vasoconstriction due to chronic hypoxia, destruction of the pulmonary capillary bed with the concomitant loss of parenchyma in emphysema are the main factors that lead to the apparition of pulmonary hypertension in patients with
c o p D3 0 ; 3 2 ; 3 3
Hogg et al. have described the presence of lymphoid follicles containing B cells in the wall of the small airways, surrounded by CD4+ T lymphocytes. This reaction seems to be
an immune response to the colonization and infection of peripheral airways27.
Clinical presentation and comorbidities
COPD is a slowly advancing disease that can develop silently for many years before the diagnosis is made. Many of the COPD symptoms are misinterpreted as signs of aging.
Dyspnea (breathlessness) is the most significant symptom in COPD patients and is usually the reason for searching medical advice. While extremely sedentary patients
unknowingly avoid exertional dyspnea by limiting their activities, most of COPD patients experience it as a persistent and progressive effort to breathe or gasping ' ' 5.
The bronchial obstruction prevents patients with COPD from emptying their lungs during the expiration, leading to hyperinflation with an increase in functional residual capacity and residual volume, accompanied by a FEVi decrease. Gas exchange is compromised as a result of the ventilation/perfusion inequality and patients become cyanotic because of hypoxemia ("blue bloater"). Later hypercarbia also settles in36. This
situation is improving with exertion in patients with chronic bronchitis due to mucus mobilization and improved ventilation/perfusion ratio, while it is exacerbated for patients with emphysema who lack respiratory reserve.
Chronic productive cough is another common feature in COPD patients. Initially the sputum production occurs only in the morning and as the disease advances it may progress throughout the day and it may become purulent during exacerbations ' 4'35.
Structural changes of the lung vessels are responsible for the onset of pulmonary hypertension, which in a long run, is the cause of right heart failure (cor pulmonale) in COPD patients30;32;33.
The last years of research have shown that inflammation in COPD is not limited to the lung, but is rather a systemic process that mobilizes an excess of cytokines and maintains oxidative stress. Up to 20% of patients with COPD loose weight and skeletal muscle mass, which decreases their chances of survival . In 1966, Burrows et al. identified the phénotype of emaciated patients suffering from pulmonary emphysema as "pink puffer"38.
There is evidence that a hospital diagnosis of COPD is associated with a higher rate of age-adjusted, in-hospital mortality for pneumonia, arterial hypertension, heart failure, ventilatory failure and thoracic malignancies16. In a cohort of COPD patients undergoing
pulmonary rehabilitation, arterial hypertension, chronic heart failure and coronary disease accounted for half of the COPD co-morbidity cases. Other comorbidities found in this study were diabetes, dyslipidemia and osteoporosis16.
An active lifestyle including at least some physical activity on a regular basis has been shown to diminish the risk of COPD related admissions and mortality39.
The role of obesity in COPD is a subject of high interest, especially as it is not clear yet whether the so-called "obesity paradox" known from the cardiology and the nephrology field also applies for COPD patients.
Clinical evaluation
a. Medical history
COPD typically develops insidiously and often remains undiagnosed for a long time. Still, cough, sputum production or dyspnea especially in a patient who has been exposed to tobacco smoke, occupational dust or occupational chemicals must raise the suspicion of COPD. Furthermore targeted history should inquire about past medical history of asthma, allergies, nasal polyps, respiratory infections in childhood and other respiratory diseases, and family history of COPD.
Dyspnea, which is the reason why most patients seek medical attention in the first place, relates well to other measures of health status when assessed with the MRC scale* and may help to predict resource utilisation and mortality more accurately than FEV]2.
b. Physical examination
During the early COPD stages, physical examination is usually normal except for sometimes prolonged expiration and wheezes on forced exhalation and doesn't allow for diagnosis. As the airway obstruction worsens, the physical exam may reveal signs of hyperinflation like tympanic percussion note, decreased breath sounds, as well as a distant heart sound, wheezes and crackles.
In severe COPD, limited motions of the diaphragm due to its depression, increased anteroposterior diameter of the chest, tachypnoea and a broken speech are typical findings
of the physical exam. Patients usually lean forward with their arms outstretched and support their weight on the palms to relieve dyspnea while they fully use their accessory respiratory muscles and expire through pursed lips. Hoover's sign*, cyanosis and asterixis as signs of severe hypercapnia may also be found.
In end-stage COPD, one should also search for peripheral oedema, neck vein distension and enlarged, tender liver as signs of right ventricular failure (cor pulmonale) secondary to pulmonary hypertension.
Investigation
a. Spirometry
Pulmonary function tests obtained by spirometry are the cornerstone of COPD diagnosis since they are highly reproducible and available and they allow determining disease severity, staging and progression as well as quantifying therapeutic response.
The most important values measured are FEVi and forced vital capacity (FVC)
while FEVi/FVC ratio less than 0.7 indicating airways obstruction with confirming the diagnosis in a patient with COPD compatible symptoms and no other explanation for the airway limitation.
Other parameters like decreased inspiratory capacity and vital capacity in the presence of increased total lung capacity, functional residual capacity and residual volume enrich us with information about hyperinflation. In emphysema, single breath carbon monoxide diffusing capacity (DLCO), a surrogate of lung parenchyma destruction, decreases with disease severity ' .
b. Other tests
Beside spirometry, other useful tests are available but not required for diagnosis. Chest radiography and computed tomography (CT) can be of help to detect emphysema in
advanced stages. Especially, high resolution CT (HRCT) is used when one is planning a lung volume reduction surgery.
Arterial blood gases reveal hypoxemia with or without accompanying hypercapnia, depending on disease severity and blood tests, are important to identify patients who develop polycythaemia, predisposing to vascular events2'34;35.
In patients who develop COPD at a young age (<45 years) or with a strong family history it might be of worth to perform an alpha-1 antitrypsin deficiency screening.
Treatment
a. Smoking cessation
As discussed previously in the risk factors section, there is strong evidence that smoking cessation can effectively reverse the accelerated decline in lung function seen in smokers so even if lost FEVi will not be recovered, this still remains an intervention of
90*71
strong benefit in terms of survival" ' and should be considered in the first place when approaching a COPD patient.
b. Pharmacological treatment
Bronchodilators
The most important agents in the pharmacologic treatment of patients with COPD are the bronchodilators. Even though they don't ameliorate the decline in lung function, they relax the airway smooth muscle and allow a better lung emptying during tidal breathing, residual volume reduction and less hyperinflation during exercise. Thus, bronchodilators reduce the perceived breathlessness, improve the exercise tolerance and overall health
3-41
status' .
Three major categories of bronchodilators are commonly used: p2-agonists (short- and long acting), anticholinergic drugs and methylxantines.
Short acting Bi-agonists (albuterol, metaproterenol) are less expensive and have a rapid onset of action. On the other hand, there is a certain risk of overuse when attempts to achieve maximal bronchodilation are made and they can cause tremor, reflex tachycardia and even hypokalemia in extreme cases '41'4 .
Long acting B2-agonists (formoterol, salmeterol) decrease the need for rescue medication use and increase the time between exacerbations. They also seem to improve health status to a grater extent than short acting P2-agonists. Currently, their role in the COPD management is an area of active research3;41.
Anticholinergic agents provide bronchodilation in the absence of sympathomimetic side effects. Tiotropium confers longer bronchodilation and reduces exacerbations and hospitalizations compared with both placebo and ipratropium3;41;42.
Theophylline is a weak bronchodilator with antiinflammatory properties whose use is controversial due to its narrow therapeutic index. It can also improve right ventricular performance in patients with cor pulmonale due to cardiac inotropic and pulmonary vasodilator effects41;42.
Corticosteroids
Although COPD is an inflammatory disease of the airways, it is generally much less responsive to corticosteroids than asthma. Inhaled corticosteroids may help reduce the exacerbation rate3'41*42 and are used in patients who remain symptomatic despite optimal
bronchodilation. Oral corticosteroids are used on short- term basis to treat acute exacerbation of the disease. The long-term use of oral corticosteroids is not recommended because of the associated side effects of these medications (such as pharyngeal candidiasis, cataracts, thinning of skin43.
Combination therapy
Combining medications of different classes offers the advantage of obtaining better results than with each drug alone. The effects of anticholinergics and p2-agonists are additive. Combination of short acting p2-agonists (salbutamol) with anticholinergics
(ipratropium) achieve superior broncho-dilation compared with either agent alone but do not improve dyspnea42. This combination (in one inhaler) is not available anymore in
Canada. Long acting p2-agonists and frequently used concomitantly with long-acting anticholinergics and are available in one inhaler. The combination of salmeterol plus fluticasone reduces the rate of decline in lung function and decreases the number of exacerbations thus slowing disease progression in patients with moderat-to-severe COPD, as shown in the TORCH trial42;44.
Future directions
Since inflammation plays a central role in developing COPD, novel therapies targeting inflammatory signaling pathways are being investigated.
Phosphodiesterase-4 (PDE-4) inhibitors are very promising. In a double-blind study, Roflumilast improved lung function and reduced exacerbations compared with placebo. Cilomilast was shown to maintain pulmonary function, improve health status and reduced the rate of COPD exacerbations during 24 weeks of treatment. Additional longitudinal studies will be needed before recommending their routine use in COPD patients with stable disease42;45;46.
The identification of the role of protease/antiprotease imbalance in the development of COPD encouraged the search for antiproteinases that could block the neutrophil elastase or the matrix metalloproteinases, in an attempt to cure COPD. Further research is needed in
i • 42
this area .
c. Non-pharmacological therapy
Long-term oxygen therapy (LTOT)
Supplemental oxygen therapy prolongs survival in COPD47'48. LTOT ameliorates
survival, exercise, sleep, and cognitive performance, quality of life and reduces hospitalization needs in hypoxic COPD patients3'42'44'49. From a physiological point of
view, the most important benefit is the improvement of pulmonary homodynamic (pulmonary hypertension, cor pulmonale). Survival event seems to be directly
proportionate to the number of hours per day the patient receives the oxygen (by nasal devices, at least 15 hrs. per day). The most accurate monitoring is made by blood gas analysis, which also permits early detection of hypercapnia3'41;42.
Pulmonary rehabilitation
The morbidity of COPD patients doesn't come uniquely from their lung function impairment, but also from several secondary systemic conditions such as: cardiovascular diseases, peripheral muscle wasting, skeletal muscle dysfunction, osteoporosis and depression. Pulmonary rehabilitation is performed in multidisciplinary programs, conceived to suit the needs of each patient and help recuperate physical and social performance; regain the autonomy.
Even though there is minimal effect on pulmonary function measurements, these programs are proven to improve dyspnea, exercise capacity, quality of life and decrease the number of hospitalizations and in the same time, they enhance patients' sense of control over their condition3;42;50;51.
Nutrition
About 50% of patients with severe COPD and 10-15% of patients with mild to moderate disease experience unexplained weight loss, most of it on the cost of skeletal muscle. This is of importance since fat free mass proved to be an independent predictor of mortality irrespective of fat mass ' .
The alterations in body composition that occur in COPD patients are unlikely to be due to decreased caloric intake, but rather to increased metabolic rate secondary to increased work of breathing, drugs, systemic inflammations and tissue hypoxia52;53.
Currently there is no evidence that nutritional supplementation offers any long-term benefit54.
Surgery
Lung volume reduction surgery (L VRS) is a surgical technique used in selected patients with emphysema and lung hyperinflation. Approximately 20-30% of lung volume is removed bilaterally in selected patients in an attempt to improve pulmonary function, exercise performance and dyspnea, but the results are rather modest. The National Emphysema Treatment Trial (NETT) revealed that the efficacy of LVRS varies among patient groups ' ' . The best results are obtained in patients with upper lobe predominant emphysema who also exhibit poor exercise performance. In this highly selected group of patients, LVRS may even improve survival.
Bullectomy is an older procedure, reserved to patients with severe bullous emphysema.
41
Usually a very large emphysematous bulla is removed to relieve dyspnea
Lung transplantation in well selected patients improves pulmonary function, exercise capacity and quality of life but not survival. Generally, 2-year survival rate after lung transplantation is reported to be 75% in COPD patients3;41;42.
Follow-up
Follow-up of COPD patients should include smoking cessation, physical exam and evaluation of their symptoms, assessment of drug treatment efficacy, and monitoring changes in spirometric parameters. The possibility of influenza vaccination should be discussed and the current therapy and prevention methods of future exacerbations should be
1 I . 1 T
reviewed ' .
Natural history and prognostic factors
The lung function develops gradually from birth to adulthood and achieves its peak around the age of 20-25 years of age in healthy subjects. This ascendant slope is followed by a physiologic decline. The forced expiratory volume in one second (FEVi) decreases
continuously and smoothly over an individual's lifetime, about 25 mL/yr in non-smokers, with the rate of loss slightly accelerating with aging20'55.
The natural history of COPD is characterized by a progressive, irreversible decline in lung function which surpasses the normal loss of FEVi per year. Thus, the FEVi decline is around 50 mL/yr in smokers and can increase as much as 100 mL/yr when severe obstruction develops. The FEVi decline is independent of its basal value, but the starting point seems to be relevant for the obstruction outcome. Thus, the unfortunate combination of a suboptimal development of the lung during childhood/adolescence and an accelerated lung function decline at a later age may lead to significant airflow limitation55.
Many smokers follow the same slope as the non-smokers and never develop severe airflow obstruction suggesting a certain resistance to the deleterious effects of smoke. By contrast, there is a population of "susceptible smokers" (about 15-30% of the active white cigarette smokers) who develop airflow obstruction and their FEVi decline follows a more abrupt slope than that of the non-smokers. In this population, smoking cessation makes all the difference, since even though the lost FEV] will not be recovered, the subsequent rate of loss of FEVi will return to normal. The sooner they stop smoking the better, since smoking cessation will not restore adequate function19'20.
Prognosis in COPD has been based on the severity of airflow limitation as measured with standard spirometry, since FE Vj is an excellent predictor of morbidity and mortality. Nevertheless, as the NHANES (National Health and Nutrition Examination Survey) study has shown, different outcomes are possible for patients with the same level of impaired function, depending on their status of current/former or never-smoker. Current/former smokers with GOLD level 3 or 4 had significantly worse outcomes than never-smokers with the same GOLD level56. Thus, disease classification based only on the airflow
limitation seems to be insufficient and other factors beside FEVi have to be taken into consideration when prognosis is made. The more complex BODE index aims to address this problem, as it reflects the BMI, dyspnea level and exercise capacity, beside the airway obstruction14;19;56.
In contrast to the FEVi that can be objectively evaluated by the means of standardized spirometry, the perception of dyspnea differs from one patient to another. Nevertheless, it is an even better independent predictor of mortality than FEVi and this is why it should be part of the evaluation of COPD patients49;5?.
A large proportion of COPD patients experience weight loss and there is an increased mortality associated to this phenomenon, independent of baseline BMI and disease severity. BMI has been proven to be an independent prognostic factor and being underweight increases all-cause mortality in subjects with COPD, especially in those with severe disease. Moreover, weight gain and being overweight improves prognosis, which made us wonder if the "obesity paradox" known from the cardiology and the nephrology field might apply for COPD patients too. This item will be treated more in detail in chapter five of this work. The weight loss usually involves both the fat and non-fat tissue. The fat free mass index (FFMI)* and midthigh muscle cross-sectional area are even better predictors of mortality than BMI and they can identify a subgroup of patients at risk despite normal BMI9;19;37;49;53;58-61.
Exercise capacity measured with the 6-minute walking test (6MWT) also correlates with mortality and in the setting of severe disease, it is an even better predictor of mortality than FEVi or BMI ' . Patients with similar degrees of airflow limitation can have different outcomes depending on their exercise capacity and the decline in 6MWT occurs independently of changes in FEVi, so these tests can be seen as complementary49'62.
Generic and respiratory-specific baseline Health related Quality of life (HRQL) scores were independently associated with both all-cause and respiratory mortality of COPD patients after adjustment for other relevant clinical and physiopathologic variables in a cohort of 321 male COPD patients. In this study, every four points increase in the SGRQ* score (which is a clinically relevant deterioration) was associated with a 5 fold increased risk of mortality49'63.
* FFMI : Fat free mass index (fat free mass divided by height (in m) squared to adjust for body surface area. * SGRQ: St. George's Respiratory Questionnaire
Increased airway hyper-responsiveness induced by histamine was found to predict mortality in COPD after adjusting for confounders but further research is needed in this
19;49
area
Acute exacerbations are a frequent reason of hospitalization of COPD patients and are characterized by an increase in dyspnea, cough and/or sputum. Usually they are due to bacterial or viral infections, even though the étiologie factor often remains unknown. The severity of an acute exacerbation can vary from increased symptoms that can be managed at home to respiratory failure and death. Exacerbations obviously play an important role in the disease progression of COPD but their influence on survival remains unclear and needs further exploration3;19;56.
Hypercapnia is a common finding in COPD with advanced disease secondary to severe ventilation-perfusion imbalance and the insufficient elimination of carbon dioxide by ventilation. Chronic but not acute hypercapnia is associated with a decreased survival in COPDpatients19;49.
Hypoxemia* while breathing room air is also a prognostic factor and there is evidence that oxygen supplementation improves survival proportionally to the number of hours of supplementation49.
COPD patients often present accompanying disorders that are not directly related to COPD and not part of the spectrum of the natural history of COPD. These disorders are commonly addressed as comorbidities and their relationship to COPD is gaining more and more attention as they have a great impact on the outcome of these patients. The two most important comorbidities in COPD mortality are cancer and cardiovascular diseases which account for almost two-thirds of COPD deaths compared to only one third attributable to respiratory failure. Mortality is higher among COPD patients with an increased level in terms of the comorbidity index (Charlson index*), which underlines once again the
* Hypoxemia: Pa02 < 55 mmHg or SaQ2 < 88%
* Charlson index: weighted index that takes into account the number and the seriousness of comorbid disease and predicts the 1 year mortality64
necessity of developing more comprehensive evaluation tools with a better capacity to assess for comorbidities16;49;64;65.
The large spectrum of prognostic factors in COPD derives from its multisystemic character and from the various comorbidities who accompany COPD. Chapters two, five and six of this work will elaborate more about these issues.
Chapter 2: Nutritional problems in COPD
Summary
Obesity is becoming more and more present in our society and its growing proportions have become alarming since obesity is known to be associated with increased risk factors for metabolic and cardiovascular disorders.
The same tendency of increasing BMI is seen in the COPD population exposing these patients to the above mentioned co-morbidities.
On the other hand, the so called "obesity paradox" leads to better survival in overweight/obese COPD patients. This chapter will discuss the possible reasons of this unexpected relation between survival and BMI and will emphasize on some nutritional particularities in COPD.
Body weight loss and its prognosis in COPD
Half of the COPD patients with severe disease and 10 to 15% of those with mild to moderate disease experience unexplained weight loss66'67. Data from survival studies have
shown reduced survival in underweight and normal-weight COPD patients when compared with overweight and obese patients53.
Wasting of body cell mass has an important impact on survival, as a decline of more than 40% of actively metabolising tissue is incompatible with life and it is a negative prognostic factor independent of the degree of lung function impairment present4 ' .
Furthermore, lower quality of life and lower exercise tolerance has been reported in malnourished patients who also complain of more intense dyspnea69. TNFct is clearly
involved in this declining process, as increased TNF-a and soluble TNF receptors were found in the plasma of COPD patients suffering from tissue depletion70.
About 26 to 47 % of the patients suffering from COPD experience malnutrition69.
Interestingly, gaining weight can reverse the unfavourable prognosis ' especially in normal-to-underweight (BMI < 25 kg/m2) subjects with severe COPD60.
Many efforts have been made to understand the causing mechanisms of the wasting process in COPD patients and further research is still needed. One explanation could be the chronic inflammation status that entertains a hypermetabolic regime with reduced energy intake (anorexia) and ubiquitin mediated proteolysis in the peripheral skeletal muscles. Inflammation can also alter the leptin metabolism and intervene in the regulation of caloric intake, as well as basal energy expenditure and body weight71'72.
Further metabolic disorders have been discovered in peripheral muscles of patients suffering from COPD. During submaximal exercise these patients experience premature
■71
acidosis associated with reduced oxidative capacity and there also is evidence of enhanced release of amino acids from the muscle during exercise in COPD patients . Following a cross sectional study, Nemery et al. reported over 20 years ago that smokers with airflow obstruction and thus susceptible to COPD were leaner than non-smokers, ex-smokers and ex-smokers without airflow obstruction75.
A recent study with primary care patients confirmed that low body weight was increased in patients with severe COPD, whereas among patients with mild to moderate COPD the prevalence of obesity was highest .
Celli et al. found BMI to be among the four most important predictor factors for mortality in COPD patients and included it in the BODE index that allows a more comprehensive evaluation of these patients14.
It is a real challenge to find out whether low body weight is a predisposing factor for COPD or it is merely a consequence of the declining health of these patients due to systemic effects of the disease. Determining the causal sense of this relation would be extremely interesting essentially because body weight is a potentially modifiable factor77
and an accessible target for nutritional intervention. The combined results of a retrospective and a prospective study showed that negative effect of low body weight can be reversed in some COPD patients78.
Obesity in COPD: a new reality
Obesity is becoming more and more prevalent in our society and some people even talk about epidemic proportions of this phenomenon. Indeed, studies based on self-reported BMI have shown that overweight has dramatically increased in Canada over the past 30 years ' so that in 2003, one third of the adult Canadian population was classified as overweight and around 15% were obese.
Traditionally we used to focus on the cachexia in patients with COPD but in accord with the new trend in our society, we currently face more and more obese COPD patients. Obesity is associated with certain health concerns in the general population and still, in some very well defined groups, it seems to be of benefice. The non-resolved mystery of the obesity paradox remains a dilemma and we'll comment on it in the present chapter in the context of COPD.
a. Obesity-associated health concerns
COPD Patients have a two- to threefold increased risk of death due to cardiovascular diseases and this association is independent of cigarette smoking, cholesterol or hypertension. Once more, the persistent systemic inflammation seems to be the link between the two pathologies, as cardiac and lung inflammation processes are remarkably similar5"69' and retrospective studies suggested that receiving low doses of
inhaled corticosteroids can reduce the risk of acute myocardial infarction in COPD patients by 32%82.
With dyspnoea as a common symptom for both cardiovascular disease and COPD and smoking as a common risk factor for both, it is quite difficult to determine the exact mechanisms linking the two diseases and a causative relationship ' .
Women suffering from COPD have a 1.8 fold increased risk of developing type-2 diabetes as compared with those who don't suffer from COPD, maybe due to oxidative stress, inflammation factors like CRP, IL-6 and TNF-a or steroid treatment. In the setting of hospital admission secondary to exacerbation, hyperglycaemia is a predictor of poor prognosis '.
Overweight/obese COPD patients are at risk for metabolic syndrome associated with dyslipidemia, inflammation, insulin resistance and cardiovascular disease especially if their fat accumulation has a visceral pattern83'84.
The exact mechanisms by which obesity ameliorates survival remain obscure and bring scientists in a big dilemma: on one hand, obesity is a known source metabolic and cardiovascular risk factors and on the other hand, it seems to be protective at least in certain selected populations, as it will be discussed below. This question requires further investigation.
b. The obesity paradox
In patients chronically affected by heart ' or kidney diseases , overweight and obesity paradoxically seems to prolong survival, a phenomenon referred to as the "obesity paradox" or "reverse epidemiology" ' ' .
This paradox seems to apply also for the COPD population with high BMI being a predictor of higher chances to survive. In a cohort of COPD patients enrolled in the Copenhagen City Heart Study, low BMI was an independent risk factor for mortality. Interestingly, in all three stages of COPD, the highest mortality was found in underweight patients. The strongest association was found in the group with severe disease (FEVi<50%), where underweight subjects had a 7 fold increased risk of mortality when compared with obese patients in the same group. As the authors themselves commented in
CO
the article, obese patients have reduced FEVi .
Obese patients, especially those with high abdominal fat accumulation experience impaired ventilatory lung function (reduction in forced expiratory volume in one second, FEVi and forced vital capacity, FVC). They also have an increased perception of strong dyspnea caused by reduced thoracic compliance due to fat deposition in the chest wall, diminished respiratory muscle strength and direct restrain of the diaphragm descent by the abdominal fat deposition88"90. In this setting, the dyspnea carries obese patients to seek
medical attention earlier than their lean counterparts. Since one of the causes for the delayed diagnosis of COPD is the silent development of disease in the first years, being brought to medical attention is definitely a positive element that sustains the obesity paradox.
Although COPD patients with higher BMI have a better survival than lean patients, this doesn't confer information about body composition. Thus, it is still unclear if this protection is offered by the fat free mass (FFM) component of BMI or by its fat constituent (FM) because the BMI lacks of discriminatory power to reflect body fat distribution91.
As opposed to starvation in which loss of body mass reposes mostly on the fat compartment, in COPD this loss occurs in the detriment of muscle mass just like in other chronic diseases.
Studies using different methods to approximate fat free mass have shown this to be a strong independent predictor of mortality in COPD37, regardless of fat mass53.
Epidemiological studies in the general population typically show U- or J-shaped
7'Q?
association between BMI and mortality ' . The U-shaped mortality curve can be dissociated into a J-shaped curve showing the association between fat mass and mortality and a reverse J-shaped curve showing the association between fat-free mass and mortality. So both high body fat and low fat free mass are independent predictors of mortality92. This
supports our hypothesis that it is not the FM that is protecting subjects with high BMI but it is rather the lean mass that infers a good prognostic factor.
Chapter 3: Hypotheses
1. Higher BMI is associated with better survival in COPD patients
2. The so-called protective effect of BMI is not due to the accumulation of fat tissue 3. The so-called protective effect of BMI can rather be explained by a group of confounding factors which are typically associated with overweight/obesity such as higher
o i
Chapter 4: Objectives and methodology
Our first objective was to prospectively follow a cohort of COPD patients and verify the hypothesis that a higher BMI would be reflected by a better survival.
Our second objective was to investigate the positive association between body weight and survival in a manner that would allow us to conclude about the possible causes of this relationship, specifically whether it is due to pure fat accumulation or to confounding factors.
The third objective derives from the second one and consists in pointing out the confounding factors.
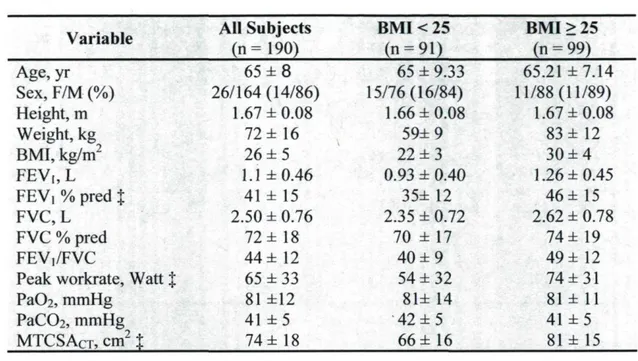
To do so, we have recruited 190 patients with stable COPD who underwent a CT scan of the right thigh to determine midthigh muscle cross-sectional area (MTCSACT). Anthropometric measurements, pulmonary function tests, arterial blood gas and exercise testing results were obtained. Two groups were formed based on the body mass index (BMI): one group of patients with BMI < 25 kg/m2 and another with BMI > 25 kg/m2.
Descriptive statistics were used to describe the study population at baseline followed by Student t tests in order to determine the differences among measured parameters in the two BMI groups. Following uni- and multivariate analyses, a regression model to predict survival was calculated. Basedon this analysis, the statistically significant confounding factors were identified.
Chapter 5: Article scientifique
OBESITY AND COPD: IS FATTER REALLY BETTER? Authors:
Roxana G Galesanu1, Sarah Bernard , Karine Marquis1, Yves Laçasse1, Paul Poirier1, Jean
■y 1
Bourbeau , and François Maltais
Affiliation :
'Centre de recherche, Institut Universitaire de Cardiologie et de Pneumologie de Québec, Université Laval, Québec, Canada. 2Respiratory, Epidemiology and Clinical Research Unit, Montreal Chest Institute of the Royal Victoria Hospital, McGill University Health Centre, McGill University.
RG Galesanu was recipient of a research training award of the Respiratory Health Network of the Fonds de la Recherche en Santé du Québec (FRSQ). This work was supported by the Respiratory Health Network of the FRSQ and by an unrestricted grant from GlaxoSmithKline, Canada.
Running head: Obesity and COPD
Word count: 2953
Address of correspondence: Dr François Maltais
Institut Universitaire de Cardiologie et de Pneumologie de Québec 2725 Chemin Ste-Foy Québec, Québec Canada G1V4G5 Tel: 418-656-4747 Fax:418-656-4762 E-mail: francois.maltais(2>med.ulaval.ca
Abstract
Objective: Overweight/obesity is associated with longer survival in chronically ill patients, a phenomenon refer to as the obesity paradox. We investigated whether the positive association between increased body weight and survival is due to fat accumulation or to confounding factors.
Methods: 190 patients with stable COPD with a longitudinal follow-up to assess survival status were enrolled. Anthropometric measurements, pulmonary function tests, midthigh muscle cross-sectional area (MTCSACT), arterial blood gas and exercise testing data were
obtained. Patients were categorized into two subgroups according to a body mass index (BMI) < or > 25 kg/m2.
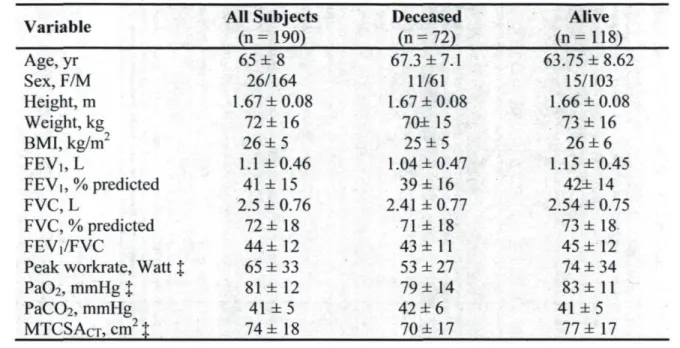
Results: 72 patients (38%) died during the mean follow-up period of 72 ± 34 months. Survival tended to be better in the overweight/obese patients but this difference did not
■j
reach statistical significance. Patients with a BMI > 25 kg/m had a better lung function and a larger MTCSACT than those with a BMI < 25 kg/m2 (p < 0.001). Overweight/obese
patients also had a significantly higher peak workrate than patients with a BMI < 25 kg/m2
(p < 0.001). PaÛ2 and PaCÛ2 were not significantly different in the two groups. When adjusted for PaC02, peak workrate and MTCSACT, patients with low BMI tended to have a
better survival.
Conclusion: These results suggest important confounders such as disease severity, exercise capacity and muscle mass should be considered when interpreting the association between increased BMI and survival in COPD.
Introduction
Chronic obstructive pulmonary disease (COPD) is becoming a global health epidemic. Even though a "preventable and treatable disease", COPD is expected to rise from the sixth to the third commonest cause of death worldwide in 2020 and to become the fifth most common cause of chronic disability worldwide by the same year . Besides progressive airflow limitation, air trapping and progressive shortness of breath, COPD also
4
has significant systemic repercussions , one of them being weight loss and skeletal muscle atrophy. These body composition abnormalities are associated with increased mortality, independent of lung function impairment .
The current global obesity epidemic is changing the nature of the nutritional abnormalities seen in patients with COPD. In fact, a rapidly growing proportion of patients with COPD do not exhibit low body weight but rather overweight and obesity . Based on the existing link between obesity and reduced life expectancy, systemic hypertension, type 2 diabetes, cancer, and cardiovascular diseases , it is tempted to speculate that body weight excess would also be deleterious for patients with COPD.
C O ~T
In patients affected from chronic heart ' or kidney diseases , overweight and obesity paradoxically seems to prolong survival, a phenomenon referred to as the "obesity
c o
paradox" or "reverse epidemiology" ' . From study to study, this observation appears to be robust and is valid up to a body mass index (BMI) of 40 kg/m2. The obesity paradox may
also exist in COPD, a statement based on the inverse relationship between mortality and BMI in this patient population ' . However, this finding is not universal .
Why would excess body weight protect against premature mortality in chronic diseases such as COPD? In a previous study we submitted that this epidemiological association could be explained by several confounding variables influencing the relationship between body weight and survival and that could not always be taken into
O O -1-1
account by statistical analyses . For example, we and others have reported that overweight or obese patients with COPD tend to get medical attention with better preserved expiratory flows and less hyperinflation compared to their lean counterparts. Obese patients
with COPD also tend to have greater muscle mass compared lean patients . These observations are important because of the high prognostic impact of these variables. If true, they would also suggest that accumulating fat may not be the reason why increased BMI may be associated with better survival in patients with COPD.
This study was undertaken to address the following questions: i) is overweight/obesity associated with better survival in COPD and ii) are there important confounding factors that should be taken into account when evaluating the relationship between survival and BMI in this diseases. We hypothesized that increased BMI would be associated with improved survival and that this relationship can be largely explained by confounders such as severity of lung impairment, muscle mass and exercise capacity that are not typically dealt with in large epidemiological studies looking at the relationship between body weight and survival in COPD. To test these hypotheses, we took advantage of a longitudinal cohort of patients with COPD that were recruited between 1995 and 2005 in our institution. Part of the data pertaining to this cohort has been published in an investigation of the role of muscle wasting and survival in COPD . Since this first publication, the cohort has been expanded and the follow-up has been prolonged.
Material and methods
Patient population
Patients with COPD were prospectively enrolled in this longitudinal cohort of patients as they enter the rehabilitation program of our institution between 1995 and 2005. The diagnosis of COPD was based on current or past smoking history and clinical evaluation and pulmonary function tests showing not fully reversible airflow obstruction (post-bronchodilator FEVi/FVC < 70%). Patients with asthma, cardiac failure as the primary diagnosis, dementia or unstable psychological conditions were excluded. The research protocol was approved by the ethics committee of the Institut Universitaire de Cardiologie et de Pneumologie de Québec and ail patients gave informed consent to participate in the study.
The 190 enrolled patients were categorized into two subgroups based on a body mass index (BMI) < (n = 91) or > 25 kg/m2 (n = 99). Cut-off limits were set as
recommended in the classifications for BMI adopted by the National Institutes of Health and World Health Organisation (WHO)12.
Anthropometric measurements
Body weight and height were measured in all patients and BMI was calculated as weight in kilograms divided by height in meters squared.
Computed tomography of the thigh
A computed tomography (CT scan) of the right thigh halfway between the pubic symphisis and the femoral condyles was performed with a fourth-generation Toshiba Scanner 900S (Toshiba Inc., Tokyo, Japan) according to the protocol described by Bernard et al . For technical reason, midthigh muscle cross-sectional area (MTCSACT) could not be
obtained in 3 patients.
Pulmonary function tests and arterial blood gases
Standard spirometry was performed according to the American Thoracic Society criteria1. The parameters retained for statistical analysis were the forced expiratory volume
in 1 second (FEVi), forced vital capacity (FVC), and the FEV|/FVC ratio. Equations used to predict normal values were those of Quanjer et al14. Arterial blood was drawn from
radial artery puncture while patients were breathing room air. Pa02 and PaC02 were measured with a blood gas machine (AVL 995; AVL Scientific Corp., Roswell, GA) in 175 patients.
Exercise testing
A symptom-limited incremental cycle exercise test was performed to determine peak exercise capacity. The exercise test was performed at room air seated on an electrically braked ergocycle (Quinton Corival 400; A-H Robins, Seattle, WA) and starting at a workrate of 10 watts. Each exercise step lasted 1 min and increments of 10 watts were used until maximal exercise workload was reached. Peak workrate was defined as the
highest exercise workload tolerated for at least 30 seconds was used as the marker of peak exercise capacity. For technical reasons, peak workrate was available in 169 patients.
Follow-up
Patients were followed for all-cause mortality until February 28 2007. We reviewed the medical chart of each patient in order to establish the cause of mortality. For patients deceased outside our hospital, these information were obtained from Institut de la statistique du Québec, a governmental organization to which all deaths in the province of Québec are reported.
Statistical analysis
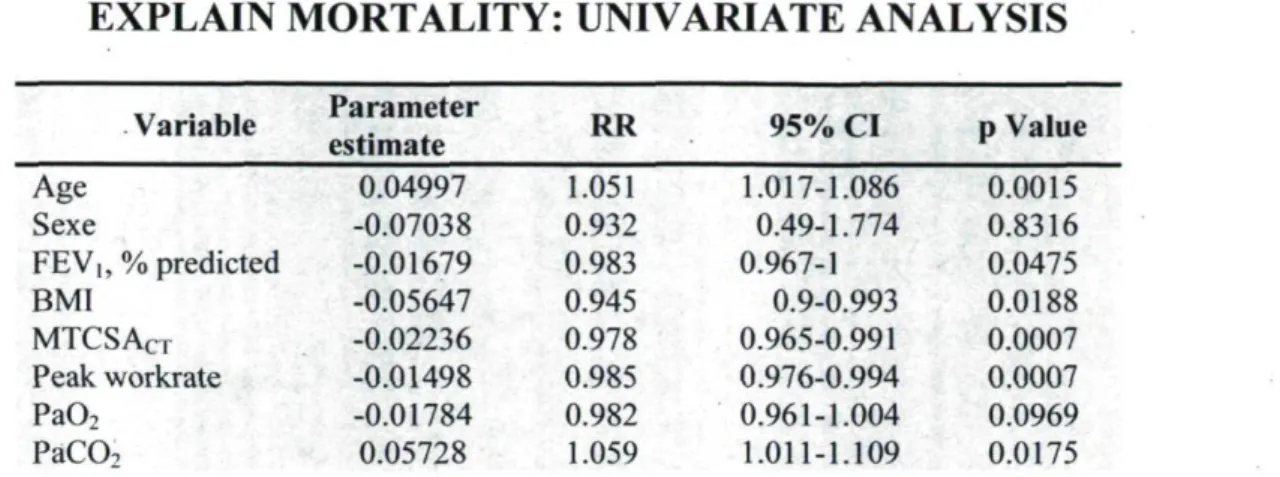
We used descriptive statistics to characterize the study population at baseline. Continuous variables are expressed as mean ± standard deviation while discrete variables are shown as percentage. The level of statistical significance was set at p < 0.05. Between-group comparisons were made using the Student t test or Mann-Whitney Rank Sum Test if the variables were not normally distributed as verified using the Shapiro-Wilk's statistic. Unadjusted survival curves according to the BMI subgroup were drawn from the Kaplan Meier statistics. We then conducted univariate analyses based on the Cox proportional hazards model in which each of the potential predictors of mortality were entered as independent variables (age, sex, FEVi, BMI, MTCSACT, peak workrate, PaÛ2, and PaC02)
and the survival status as the dependent variable. We then proceeded to multivariate analysis using stepwise regression and best subset models. Both methods pointed out
MTCSACT, PaC02 and peak workrate as important variables to predict mortality and they
were entered in the final regression model from which we constructed the adjusted survival curves. Data were analysed with the S AS software system (version 9.1, SAS Institute Inc., Cary, NC). The results of the regression analyses are listed in terms of estimated relative risks (RRs) (hazard ratios) with corresponding 95% confidence intervals (CIs).