HAL Id: hal-01256707
https://hal.archives-ouvertes.fr/hal-01256707
Submitted on 15 Jan 2016
HAL is a multi-disciplinary open access
archive for the deposit and dissemination of
sci-entific research documents, whether they are
pub-lished or not. The documents may come from
teaching and research institutions in France or
abroad, or from public or private research centers.
L’archive ouverte pluridisciplinaire HAL, est
destinée au dépôt et à la diffusion de documents
scientifiques de niveau recherche, publiés ou non,
émanant des établissements d’enseignement et de
recherche français ou étrangers, des laboratoires
publics ou privés.
Telemedicine framework using case-based reasoning with
evidences
Alsane Sene, Bernard Kamsu-Foguem, Pierre Rumeau
To cite this version:
Alsane Sene, Bernard Kamsu-Foguem, Pierre Rumeau. Telemedicine framework using case-based
reasoning with evidences. Computer Methods and Programs in Biomedicine, Elsevier, 2015, vol. 121
(n°1), pp. 21-35. �10.1016/j.cmpb.2015.04.012�. �hal-01256707�
To link to this article: DOI:
10.1016/j.cmpb.2015.04.012
http://www.sciencedirect.com/science/article/pii/S0169260715001108
This is an author-deposited version published in:
http://oatao.univ-toulouse.fr/
Eprints ID: 13953
To cite this version:
Sene, Alsane and Kamsu-Foguem, Bernard and Rumeau, Pierre
Telemedicine framework using case-based reasoning with evidences.
(2015) Computer Methods and Programs in Biomedicine, vol. 121 (n°1).
pp. 21-35. ISSN
0169-2607
O
pen
A
rchive
T
oulouse
A
rchive
O
uverte (
OATAO
)
OATAO is an open access repository that collects the work of Toulouse researchers and
makes it freely available over the web where possible.
Any correspondence concerning this service should be sent to the repository
administrator:
[email protected]
Telemedicine
framework
using
case-based
reasoning
with
evidences
A.
Sene
a,b,
B.
Kamsu-Foguem
a,∗,
P.
Rumeau
baLaboratoireGéniedeProduction(LGP),EA1905,ENIT-INPT,UniversitédeToulouse,47avenued’Azereix,BP1629, 65016TarbesCedex,France
bLaboratoiredeGérontechnologieLaGrave,CHUToulouse/Gérontopôle/UMR1027Inserm-UniversitéToulouse3, HôpitalLaGrave,PlaceLange,TSA60033,31059ToulouseCedex9,France
Keywords: Telemedicine Case-basedreasoning Evidencesources Medicaltaxonomy Oncology
a
b
s
t
r
a
c
t
Telemedicineisthemedicalpracticeofinformationexchangedfromonelocationtoanother throughelectroniccommunicationstoimprovethedeliveryofhealthcareservices.This researcharticledescribes atelemedicine frameworkwithknowledgeengineering using taxonomicreasoningofontologymodelingandsemanticsimilarity.Inadditiontobeing aprecioussupportintheprocedureofmedicaldecision-making,thisframeworkcanbe usedtostrengthensignificantcollaborationsandtraceabilitythatareimportantforthe developmentofofficialdeploymentoftelemedicineapplications.Adequatemechanisms forinformationmanagementwithtraceabilityofthereasoningprocessarealsoessential inthefieldsofepidemiologyandpublichealth.Inthispaperweenrichthecase-based reasoningprocessbytakingintoaccountformerevidence-basedknowledge.Weusethe regularfourstepsapproachandimplementanadditional(iii)step:(i)establishdiagnosis, (ii)retrievetreatment,(iii)applyevidence,(iv)adaptation,(v)retain.Eachstepisperformed usingtoolsfromknowledge engineering andinformation processing(naturallanguage processing,ontology,indexation,algorithm,etc.).Thecaserepresentationisdonebythe taxonomycomponentofamedicalontologymodel.Theproposedapproachisillustrated withanexamplefromtheoncologydomain.Medicalontologyallowsagoodandefficient modelingofthepatientandhistreatment.Wearepointinguptheroleofevidencesand specialist’sopinionsineffectivenessandsafetyofcare.
1.
Introduction
Telemedicineisaremotemedicalpracticeusing telecommu-nicationandinformationtechnologies.Itisanefficienttool forcollaborationbetweenphysiciansbutitalsooffersmany others benefits (e.g. costsavings, improved care,improved
∗Correspondingauthor.Tel.:+33624302337/614556164;fax:+33562442708.
E-mailaddresses:[email protected](A.Sene),[email protected](B.Kamsu-Foguem),[email protected] (P.Rumeau).
accessand real-timeresponses).Likeany medicalpractice, telemedicineaimedatestablishingadiagnosis,providinga preventiveorpost-therapeuticmedicalmonitoring, perform-ingmedicalacts,prescribingdrugsandservices.
The largeamount ofhealth knowledgeavailable tothe medicalpersonnelishardlyembraced.Medicalinformation isdoublingevery5years[1]and81%ofthephysiciansspend
lessthan5hpermonthreadingmedicaljournals.Only20% oftheknowledgeusedbycliniciansreliesonevidence-based resources. IntheUnitedStatesofAmerica(USA),thereare anestimated1.5millionprescriptionsandmedicationerrors amountingforanextracostofcloseto50%.Theanalysisof structured medicaldata could help retrieveformer similar casesandhelpinchoosingthebestdiagnosisandtreatment strategy, as well as ease the extraction of epidemiological information[2].
Telemedicineisanewmedicalapproachcontributingto theimprovementofhealthcareaccessandprovision(e.g. pen-itentiary institutions,nursing homes,mountainous regions or less-favored areas). It canprovide additional healthcare opportunities particularly in the fields of aviation, space and maritime transport; where proper remote diagnosis andtreatmentcanavoidcostlymedicalevacuationservices (MEDEVAC).
Telemedicine is scarcely written in law, but national governmentsandhealthcareauthoritiesinfluencethe orga-nizationofhealthcareservicesatadistance,likeinFrance where we will test our research method. The French Law hasdefinedfiveactsoftelemedicineindecreen◦2010-1229
(October19,2010)[3]:
- Teleconsultation:aphysicianperformsaremoteconsultation toapatientwhocanbeassistedbyhealthprofessional. - Teleexpertise:aphysiciansolicitsremotelyotherphysicians
todiscussandtreatacase.
- Medicaltelemonitoring: acaregiver observes and interprets medicalsigns ofpatient. Thiscan be doneeither inthe manualorautomaticmode.
- Medicalteleassistance:aphysicianassistsremotelyanother medicalprofessionaltoperformamedicalact.
- Medicalcoordinationofemergency.
Telemedicinebenefitsfromalargebibliographybut prac-ticalchallenges remain:organizingthemanagement ofthe knowledgewealth,improvingsecurityengineeringand risk managementinthecontextofacontinuousimprovementof healthcareservices.Inthiscontext,informationmodelingcan betracedaccording tomedicalpatternsthroughstructured datathatarelinkedtopracticesviatelecommunication tech-nologies.
Thereafter,weproposetoenrichthecase-basedreasoning (CBR)process witha conceptualinformationsystem archi-tecture thatseeks toreflectboththe conventional medical reasoningand the CBR. Thisarchitecture isbased on con-ventionalmedicinestepbystepprocess.Thefirstfourstages reflectthemedicalconsultationprocess:
• Establishmentofthediagnosisofmedicalproblems. • Researchoftherighttreatment.
• Verificationofeffectivenessofthetreatment. • Adjustmentofthetreatmentifrequired.
Thefifthstageisthecontinuousupdatingoftheknowledge basetoensureitspermanentconsistencyandsustainability. Themorecasesinknowledgebasewehavethemoreefficient isthecase-basedreasoningmethod.Weareillustratingthe
approachthatweareproposingwiththestudyofanoncology case.
Theremainderofthispaperisorganizedinfoursections. Section 2providesthetheoreticalbackgroundand motivat-ing issuesabouttelemedicineandcase-basedreasoning.In the first partofSection 3, wedescribethe proposed archi-tecture withits detailedstepsforpurposesofdevelopment inthesuggestedmethodology.InthesecondpartofSection 3,itisprovidedarealcasestudyfromtheoncologydomain. Section4presentsadiscussionoftheachievedandexpected results.Section5givestheconclusionwithoutline descrip-tionsofprovidedcontributionintheresearchworkpresented inthispaper.
2.
Telemedicine
and
case-based
reasoning
Inthissectionaftershowingtheinterestofusingcase-based reasoning(CBR)intelemedicinewewillmentionafewrecent worksaddressingCBRandtelemedicine.Andattheendwe willalsoshowtheinnovativeaspectsoftheproposedresearch approach.
2.1. Thecase-basedreasoningparadigm
The case-based reasoning copies the human behavior. It resolvesproblemsseekingsimilarcasesandadaptingthem. CBRisareasoningparadigmthatinsteadofrelyingon gen-eralrulesormodelschoosesthespecificknowledgecontained intoalreadysolvedinstancesofproblems[2].Itisformalized asfour-stepprocess:
• Retrieve:findsimilarcases.
• Reuse:adaptandusesimilarcasetoresolveanewproblem. • Revise:adjustthenewsolution.
• Retain:storetheresultingexperience.
Thequalityofcase-basedreasoningmethoddepends pri-marilyonagoodrepresentationofcasesintheretrievestep(it meanstounderstandcurrentcaseinrelationtooldcasesin knowledgebase)andtherichnessofknowledgebase.Inother words,thedevelopmentofthecase-basedreasoningprocess isdrivenbythefollowingactivities[4]:
- Adaptingoldsolutionstomeetnewdemands. - Usingoldcasestoexplainnewsituations. - Usingoldcasestocritiquenewsolutions.
- Reasoningfromprecedentstointerpretanewsituation. Therationaleforusingthecase-basedreasoningprocess istosupporttheformalizationofreasoningproceduresfor collaborativemedicalactsintelemedicine.
Infact,thisparadigmissimilartothephysician’s reason-ing regardingtheassessmentofnewscasesincomparison with reportedcases andeventually adaptationof retrieved solutions(ifthisisnecessary).
Furthermore, CBR has methodological variations and systemic approaches allowing theuse of appropriate tech-nologies,withaconsistencyofsystemapplicationguidance andflexibilityofservices.
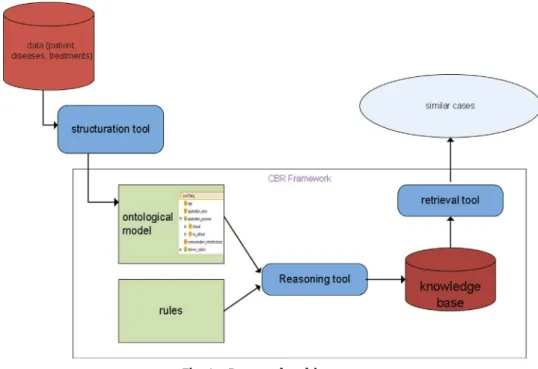
Fig.1–Proposedarchitecture.
Intermsofimplementationpracticeswecandescribefour maintypesofcase-basedreasoning[5]:
• Case-basedreasoningusingnearestneighbor:thisisthemost widelyusedtechnologyinCBR.Thesimilaritybetween tar-getcaseandeachcaseintheknowledgebaseisdetermined inordertorankthem.
• Case-basedreasoningusinginduction:thismethodpartitions casesinclusters.Casesineachclusteraresimilar,andas it is assumed (usually correctly) that caseswith similar descriptionsofproblems (where possibleits key compo-nents) will refer to similar problems and hence similar solutions.
• Case-basedreasoningusingfuzzylogic:fuzzylogicdealswith approximate reasoning with variables possibly having a truthvaluethatrangesindegreebetween0and1. Further-more,theattributesofcasescanberepresentedbylinguistic variablesassociatedwithspecificfunctions.
• Case-basedreasoningusingdatabasetechnology:database tech-nologycanbeusedtoimplementcase-basedreasoning.The problemisthat the databases use onlystructured infor-mationandusuallyemployanumberofexactmatchesto answerqueries.
2.2. Stateoftheart
Many works have already addressed telemedicine. These worksdifferintermsoftelemedicineactscoveredand meth-odsusedtopracticetelemedicine.
Authors in [6] suggest a different method (conceptual graphsandargumentativelogic)andfocusontele-expertise act.Theyproposeaframeworkforthedecisionmaking pro-cess to ensure traceability in teleexpertise. They visualize reasoningby CoGui [7] softwarethat includesfunctions to editconstraintsandrulesfortheassistanceinthereasoning process.Intelemonitoringact,the purposeofMeenuSingh
et al.’s works in [8] is to use a tool (handheld tele-electrocardiogram) to identify heart condition in a rural underservedpopulation.Theobjectiveofthisstudywas clini-calvalidationofthiselectrocardiogramasascreeningtoolfor evaluationofcardiacdiseasesintheruralpopulation.Some activitiesofteleconsultationarealready doneinthe region of Midi-Pyrénées inFrance as part of a health project led by GCS (health carecooperation consortium) [9] Télésanté Midi-Pyrénées.Ahealthinformationsystemisavailablefor physicians in order to deliver remote healthcare services. Inteleassistance,Giorgio[10]proposesamedicaldevicefor healthmonitoringandteleassistanceapplications.This sys-temallowsreal-timerescueofpatientshavingheartfailure andhighriskoflife.
SomeworksarerelateddirectlytotheapplicationofCBR inmedicaldomain.Montaniet al.[2] proposeacase-based decisiontool.Theiraimistohelpdoctorsindiabetestherapy revisionthroughanintelligentretrievalofdatarelatedtopast casessimilartothetargetone.Inourapproachwepropose case-basedreasoningarchitecture.
Thenon-exhaustivereadingofworksrelatedtothe med-icalapplicationsofcase-basedreasoning[2,4,8]shows that they mainlyuse the basicCBR process with four steps. In ourreasoningapproach,duetothesensitivityaboutthe com-plexissuesofthemedicalfield,weaddanotherstepinthe CBRprocessinordertoincreasethereliabilityofthemedical reasoningprocesses.
Inwhatfollows,wewillpresentindetailourarchitecture enrichingtheCBRprocessandthenanillustrativeapplication oftheproposedapproachinoncology.
3.
Research
methods
Inthissectionwewillfirstlistandexplaintheconstitutive elementsofourarchitecture.Thenwewillstudytherelation
Fig.2–CBRprocess.
betweentheelementsandhowtocombinethemtobuildan efficientreasoningsystemabletoprovideeffectivesupportin telemedicine.
3.1. Proposedarchitecture
Fig. 1shows the proposed architecture that isintended to beeasilyexpandable.Thestageofstructuringand concep-tualizationisnotpresentlyfullyautomatedbutitismadein collaborationwithexpertsofthemedicalfield (particularly inoncologyandgeriatrics).Thecompleteautomationofthis architecturewillbetheobjectoffuturestudies[11].
Theproposedarchitecture(Fig.1)combinesontologiesand rulesinreasoningtoolthatformalizesknowledgemodeling forthedescriptionofcollaborativepracticesandinformation retrieval.
Anontologicalmodelisobtainedfrompatients,diseases, andtreatmentdatabythestructuringtool.Thena reason-ing tool (takinginto accountthe specifiedconstraints and rules)canchecktheconsistenceofontologyandmake infer-ences.Theresultwillbeaknowledgebasewhichwillbein communicationwiththeretrievaltoolaimingtofindsimilar cases.
WehaveinFig.2theCBRframework(withfivesteps)based ontheproposedarchitecture.Eachstepwouldbeperformed usingsuitabletoolsfornaturallanguageprocessing,data rep-resentation,ontologymodeling,indexationandinformation retrieval.
Duringresearchoftreatment(firststageofreasoning),we willapplysuccessivelytwotechniquesoftenusedseparately: case-basedreasoningusing inductionthencase-based rea-soningusingnearestneighbor.Thepurposeistomakecase retrievalfasterbutalsoefficient.Infactapartitionofthecases baseindifferentclustersallowstoreducetheresearchspace andtomakesimilaritycalculationsonasmallgrouponwhich thereasoningprocedureswillhavetofocusforthe determi-nationofthemoresuitablecases.
Fig.3–Medicaltaxonomy.
• Ontology
In thecontext ofcomputerscience, ontology isusedfor information organization and knowledgerepresentation. Defined originallyin 1993 by Thomas Gruber [12] as an
explicitspecificationofaconceptualization,ontologyisdesigned for knowledge sharing.Ontology contains a hierarchical description of concepts and relationships that can for-mallyexistforanentityoracommunityofentities.The developmentofontologiesisessentialtoformalizea com-monvocabularyfordistributedcollaborationinaparticular domain.Fourcategoriesofontologycanbedistinguished dependingonsubjectoftheconceptualization[13]. - Applicationontologies:statementsofthemeaningofterms
tomodelknowledgeneededforaspecificapplication. - Domain ontologies: conceptualization of a particular
domain(e.g.medicine,automobileindustry,oenology). - Generic ontologies: upper conceptualization applicable
acrossavariedrangeofdomainsets.
- Representation ontologies: explanation of the concep-tualizations that underpin knowledge representation formalisms.
• Naturallanguageprocessing(NLP)
NLP operates as a practical tool within the human–computer interaction framework and encom-passes language understanding or language generation tocover taskssuchasinformationretrieval,information extraction and speech processing. Natural processing language may increase the feasibility and effectiveness ofmoreapplicationsinthemedicaldomainbymakingit easiertostructureinformationfromdifferentsources[11]. Infactitcanincreasetheeffectivenessofcommunication means (e.g. proper use of the medical devices) tomake them more user-friendly for collaborative teams. NLP willalsofacilitatethe conversionofmedicalinformation from computer databases into understandable human language.
Beforethedescriptionofthe5stages,wewillfocusona mostimportantnotionincase-basedreasoning:the“case”.It isgenerallydefinedasasetoffeaturesrepresentinga prob-lem,itssolution,and indicationsabouthowthesolutionis generated.Casewillbeconsideredlikeavectorofconcepts characterizingasituationwithanontologymodeling.
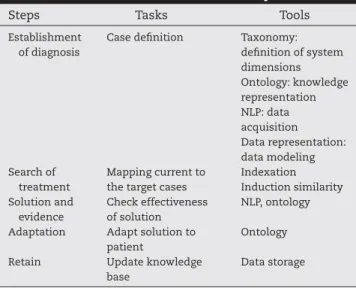
InTable1,foreachstepofourarchitecture,wedescribethe associatedtasksandtoolsusedfortheimplementationofthe CBRprocess.
Fig.4–Medicalontology.
3.1.1. Taxonomy
Taxonomyisaclassificationofconcepts,withtheprinciples underlyingsuchanarrangement.Taxonomyisoftenseenas theminimalstructureofontologyincomputerscience.
Table1–TasksandtoolsusedfortheCBRprocess.
Steps Tasks Tools
Establishment ofdiagnosis
Casedefinition Taxonomy: definitionofsystem dimensions Ontology:knowledge representation NLP:data acquisition Datarepresentation: datamodeling Searchof treatment Mappingcurrentto thetargetcases
Indexation Inductionsimilarity Solutionand evidence Checkeffectiveness ofsolution NLP,ontology Adaptation Adaptsolutionto
patient
Ontology Retain Updateknowledge
base
Datastorage
Asdescribedearlierthedomainontologycontainsa hier-archical description of concepts, which corresponds to a taxonomicstructurationofclasseswithrespecttotheir spe-cializationrelation.
In [14] Tulu et al. proposed a taxonomy structuring telemedicinedomain.Theyidentifiedfivedimensions(Fig.3): (1)applicationpurpose,(2)applicationarea,(3) environmen-talsetting,(4)communicationinfrastructure,and(5)delivery option. Applicationpurposeand applicationarea represent themedicalpartandthelastthreedimensionsaretoolsand placestodotelemedicine.
Table2providessomeexamplesofmedicaltaxonomy con-tentthatisapplicableineachdimension.
Taking into account the taxonomy presentedabove, we builtdomainontologyofmedicalfieldwiththeopen-source ontologyeditorcalledProtégé®
[15].Fig.4showsasegmentof ourontologywithtreatment’sassertions.
Themostimportantconceptsarepatientandtreatment. The case representation describes the treatment and the patientisthemaincomponentofthisdescription.
Patientconcept
Thisconceptsummarizesallconsideredattributesinthe characterizationofapatientcondition.Itistheinformation requiredfortherecognitionofsymptoms,theestablishment
Table2–taxonomydimensions.
Dimension Contain
Applicationarea Cardiology Dermatology Neurology Oncology Infectiousdiseases Applicationpurpose Nonclinical:
Research Patienteducation Evaluationresearch Clinical: Teleconsultation Telemonitoring Teleexpertise Teleassistance Drugstrials Rehabilitation Patientcasereview Deliveryoption Devices:
Electrocardiogram A-rayscanner Camera
Application:
Naturallanguageprocessing Interactivevideo
Interactiveaudio Realtimecommunication Environmentsittings Hospital
Patient’shome Medicalcenter Communication infrastructure Opticalfiber ADSL GSM Satellite ATM
ofthediagnosiswiththemeansavailabletothehealth pro-fessionals.
Fig. 5showshow are organizedthe additionalconcepts requiredtocharacterizethecomponent“patient”.
Treatmentconcept
Inthetreestructureoftreatmentconcept,wefindall fea-turesofmedicalsystem(Fig.6):
• Thepatient:apersonwhoisarecipientofhealthcareand associatedtreatments.
• The disease:anabnormalcondition thataffects apatient withcertainsymptomsandsigns.
• Thephysician:amedicalprofessionalwhoprovidesthe diag-nosisandtreatmentofdiseases.
• Environment:hospital,patienthome,etc. • Meansandoptions:devicesandapplications;
• Prescriptions:amedicalinstructionsofcare(e.g.bydrugs)or complementaryinvestigationstranscribedbyaphysician. • Evidences: scientific proofs that serve to support clinical
decision-making.
• Palliativecare:therapiesthatrelievesymptomsofdiseases withoutcurativeintent.
Fig.5–Patientconceptdefinition.
• Alternativemedicine:naturopathicandtraditionalmedicine practices(e.g.homeopathy,AfricanandChinesemedicine). • Chemotherapy: treatment of cancer with chemical
sub-stances(chemotherapeuticagents).
Table3–casefeatures.
Concepts Abbreviation fortable
Type Values
Patienttreated
Name pin String
Firstname pifn String
Age pia Integer
Symptoms ps Vectorof string Behavior phbs,phbd, phbsp String [Smoker, drinker, sportsman] Heritabledisease phfhd String
Medicalstate phm Vectorof string Physician Name String Specialty String Type Integer Disease Disease pd Vectorof string Alternative medicine
String [Yes,no] Palliativecare String [Yes,no] Chemotherapy String [Yes,no]
Evidences
Confidence Float
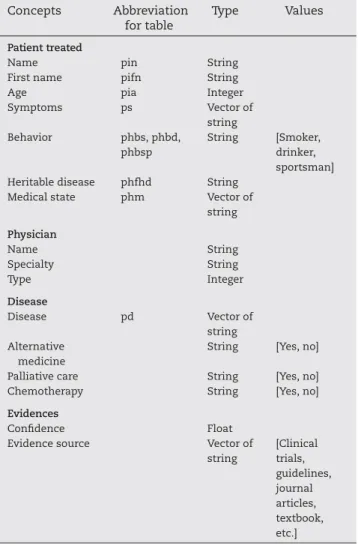
Evidencesource Vectorof string [Clinical trials, guidelines, journal articles, textbook, etc.] 3.1.2. Casedefinition
Table3showsfeaturesdefiningacase.Foreachattributewe havethepossiblevaluesandtheirtype.
3.1.3. Case-basedreasoningprocess
InTable4wesummarizeeachstepwiththemainattributes.
3.1.3.1. Establishmentofdiagnosis. Atthislevel,theaimisto identifythepatient’sdiseaseorhealthproblemandclinical condition.Theestablishmentofadiagnosiscorrespondstothe firststageofourcase-basedreasoning.Thestudyofmedical signsandsymptoms(forexamplecomparisonwithsymptoms inInternationalClassificationofDiseases(ICD)givesasetof diseases).Aninvestigationofkeypatientparameters(namely: age,medicalhistory(lifestyleandfamily)),clinicaltrialsand booksprovidesuswiththeinitialmeansforachievinga rele-vantdiagnosisandtreatmentoftheconsidereddisease.The taxonomiccomponentofdomainontologyandthedata rep-resentationare themodeling elementsusedfortheformal representationofmedicalcases(Fig.3).Theconceptsusedfor thisstagearepresentedinFig.7.
Intheprocessforestablishingthediagnosisofadisease, wewillfirstcomparesymptomsbetweenthecurrentcaseand previousmedicalcasesrecordedintheknowledgebase.This comparisonwillbedonewithadiagnosisalgorithm(Fig.8) oralocalsimilarityfunctionoftoolslikeProtégé®
.Ifthisis
Fig.7–Patientconcept.
enoughtoconfirmadiseasewecanstartthesearchfora treat-mentorelseweuseothersourceslikeInternationalStatistical ClassificationofDiseasesandRelatedHealthProblems, usu-allycalledbytheshort-formnameInternationalClassification ofDiseases(ICD).
3.1.3.2. Research oftreatment. After theestablishment ofa diagnosis,asetofpossibletreatmentscanbeidentifiedand theirprioritizationsbasedonthepatient’sneeds.Thechoice oftreatmentdependsonthecomparisonofcurrentpatient factors(e.g.ageandmedicalcondition)withtheentire candi-datetreatmentscorrespondingtothediagnosisestablished. Inordertodothis,wewillcalculatesimilaritieswiththe fol-lowingequation:
s=
n
X
i=1
f(Ti,Si)ײi
s: similarity between the current case of the patient involvedandtherecordedmedicalcasesofpastpatients;T:
attributeoftargetcase;S:attributeofsourcecase;i:current attribute;n:numberofattribute;˛:theweightingofattributes inordertorankthemaccordingtotheirimportanceand pri-orityscalesofthemedicalcontext.Forexample,thelifestyle ofapatientcanbeconsideredmostimportancethathisage, forfallspreventionintheelderly.
Thisstageprovidesapre-treatmentassessment,asetof treatmentsthatwewillweightinstage3(solutionand evi-dence).
3.1.3.3. Solution and evidence. This is acritical step ofthe executionoftheproposedmethod,inparticularregardingits effectiveness.Themostcredibleandreliabletypeoftreatment isthatwhichprovidesananalysisofthesourcesofevidence andexperts’opinions[16].
Sourcesofevidence:
Eachtreatment(case)isregisteredasfollows(Fig.9). Effective treatmentsandtheir associatedreferences can beidentifiedusingontologyalignmenttechniquesindigital technologiesforhealthcare[17].Ifproposedreferencesallow choosingonetreatmentthenweproceedtothenextstageor elsewewilltakeaccountoftheexperts’opinions.References canbe:
• Areviewarticle:presentingresearchresults.Articlemustbe reviewed byexpertswithin thesame subjectarea before publication.
Table4–Conceptsandstepsmapping.
Step Attribute Use
Establishmentofdiagnosis Patient Thestudyofmedicalsigns,symptomsand patient’shistoryprovidesdiagnosis Researchoftreatment Disease Case-basedreasoningusinginductionto
partitiondiseasescase-basedreasoningusing nearestneighborstofindmostsimilarcases Solutionandevidence Patient
Disease Evidence
Studyofsolutionandevidenceisdonetaking intoaccountdiseasesandpatientfeatures
Adaptation Patient
Disease Environment Evidence Delivery
Thetreatmentwillbecustomizedtopatientand environment
Retain Treatment Storageoftheresultingexperience(casewith
diagnosisandtreatment)intheknowledgebase
Fig.8–Diagnosisalgorithm.
Fig.9–referenceconcept.
• Guidelines:showingacourseofaction.Guidelinesmaybe issuedandusedbygovernmentalorprivateorganization andfollowingthemisnotmandatory.
• Aclinicaltrialisascientificresearchstudyonhuman sub-jectsintendingtoassesseffectivenessandtoleranceofa prospectivediagnosticortherapeuticintervention.
3.1.3.4. Adaptation. Generally,itisdifficulttoobtainafully similarcasetopreviousones.Wearerequiredtomake reason-ableadaptationstomatchthecurrentmedicalenvironment andthemedicalneedsofthepatientconcerned.Thereisa widevarietyofmedicaloptionstomeetthedifferent anatomi-calandphysiologicalcharacteristicsofpatientssufferingfrom thesamedisease.Thetreatmentapproachtypicallydepends onthecategoryandcriticalnatureofthepatient’s parame-ters.Forexample,onamedicalprescriptiontheindications
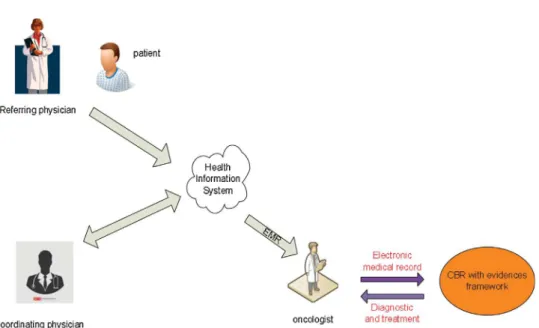
Fig.10–Collaborativemodeloftelemedicinedelivery.
Fig.11–Casesimportintheknowledgebase.
anddosagerecommendations dependonvariables suchas theseverityandchronicityofthediseaseortheageand gen-derofpatient.Thechoiceofthebesttreatmentisdetermined byaconsiderablesimilarityamongcasesintheirattributes andtheadaptationofthetreatmentshouldbebasedonthe patient’scondition,theclinicalresponseandthepossibleor occurringsideeffects.
3.1.3.5. Retain.Itmarks asignificantstage inthe informa-tion management cycle of case-based reasoning. This is contributing to support the reuse of the recorded cases withtheirassociatedreasoning(establishmentofdiagnosis or search for treatment) for information retrieval, knowl-edge and information sharing and decision making. The structuration of cases base isdetermined by the indexing functionsand the models ofmemory organization (simple model, model with dynamic memory or model based on categories)ofthecase-basedreasoningsystem. This struc-turation,forexample, canuse anetworkofcategories and cases to explain organizational patterns according to the characteristics describedbya name,a valueandalevel of importanceregardingthemembershipofacaseinacategory (Table5).
Theeffectivestepofretainingdependsonthe obtainabil-ity ofthe essential bibliography, procedures,methods and services toachieve theefficient datastructuration andthe availabilityofsignificantinformation.
3.2. Casestudy:oncologycase
Telemedicine ispredominantly used formanaging chronic diseasesorcriticalmedicaldomains,suchascardiology, radi-ology,ophthalmologyoroncology[18].
In ourcase study,and inthe context ofsupportingthe developmentofremotecollaborationbetweenhealth profes-sionals, we use the model of teleexpertisedefined bythe GCS TélésantéMidi-Pyrénées (Fig. 10). Thereferring physi-cian needs a certain expertise regardingcomplex medical
Table5–Caseorganization.
Typea Typeb Typec Typen
Treatmenta1 Treatmentb1 Treatmentc1 Treatmentn1 Treatmenta2 Treatmentb2 Treatmentc2 Treatmentn2 Treatmenta3 Treatmentb3 Treatmentc3 Treatmentnq
Fig.12–Symptomsandhistoriesofpatients.
Fig.13–Establishmentofdiagnosis.
problems and he made the request (in a synchronous or asynchronous manner) on the health information system (SIS) of the GCS. The coordinating physician contacts the requiredphysiciantoobtain an expertmedicaladviceand organizesthecollaborativemedicalsessionaccordingtothe contextualcharacteristics ofthetargetcase.Inthemedical situationdescribedinthiscasestudy;therequiredphysician isanoncologistwhointeractswiththecase-basedreasoning
system.However,theoncologistneedstotakeintoaccount theopinionsoftherequiringphysician;thepatientsandtheir families.Theprimarysourcesofdataforuseinthisstudyare realanonymizedmedicalrecords.Alistofprospectrecordsof datafromobservationaldatabaseswasaskedfromanexpert physicianworkinginageriatriconcologyunitofauniversity hospitalinToulouse.Itwasrequiredthattherecordswould includetheestablishmentofthediagnosisandthetreatment
Fig.15–Researchoftreatmentwithdetailsandquery.
Fig.16–Casewithverifiableevidences.
ofthecondition.Thephysicianprovidedalistof10names,a physicianinvolvedinthestudycheckedtherecordsfor com-prehensiveness,andthenfromthe8remaininganonymized records four were randomly selected. Three cases were integratedinthetargetknowledgebaseandtheforthonewas usedasthetestcaseprovidedfortheexecutionofcase-based reasoningwithevidences.
Even if our study is in oncology, this framework can be applied on any branch of medicine. In Fig. 11 we have 3cases(treatments) incomma-separated value(CSV) files used to import the attributes of the cases. CVS is a shared file format that is commonly supported by scientific applications to represent sets or sequences of records.
Infactforthecasestudy,weuseProtégé3.5®
tocheckthe consistenceoftheontologyandMyCBR®
plug-intocompute thecasebasedreasoningprocess.
3.2.1. Oncologycase:establishmentofdiagnosis
According to the first stage in the case-based reasoning process,theestablishmentofdiagnosisisperformedby com-paringsymptomscharacteristicofthepatient’sdisease.This isachievedmainlythroughananalysisofsimilarities symp-tomsofpatientsinthedatastructures.Thepatienthistory canbeusedtoenablepromptandreliablediagnosis(Fig.12).
Activatingonlytheattributesymptom,wegetapercentage ofsymptomsfoundinthepatientincomparisontothecases intheknowledgebase.Thediseaseofthematchingcaseis lymphoma(asdiagnosedbytheexperts)(Fig.13).
3.2.2. Oncologycase:researchoftreatment
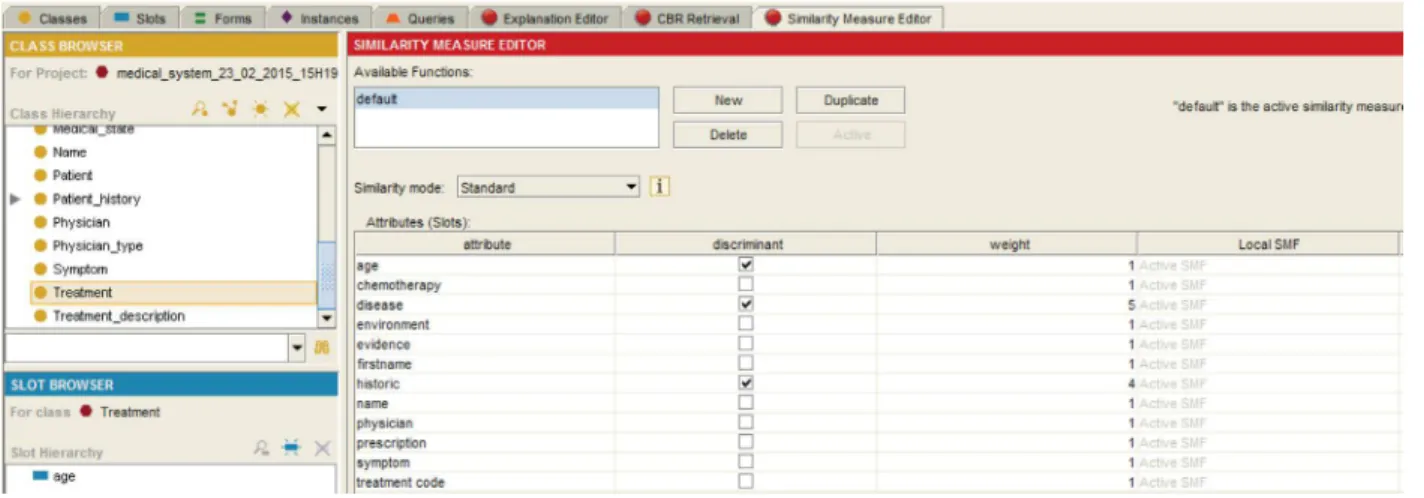
Thefollowingfigureshowsour approachtosearch a treat-ment.Eachfielddescribingtheconcepttreatmenthasaweight dependingonitsimportance(Fig.14).
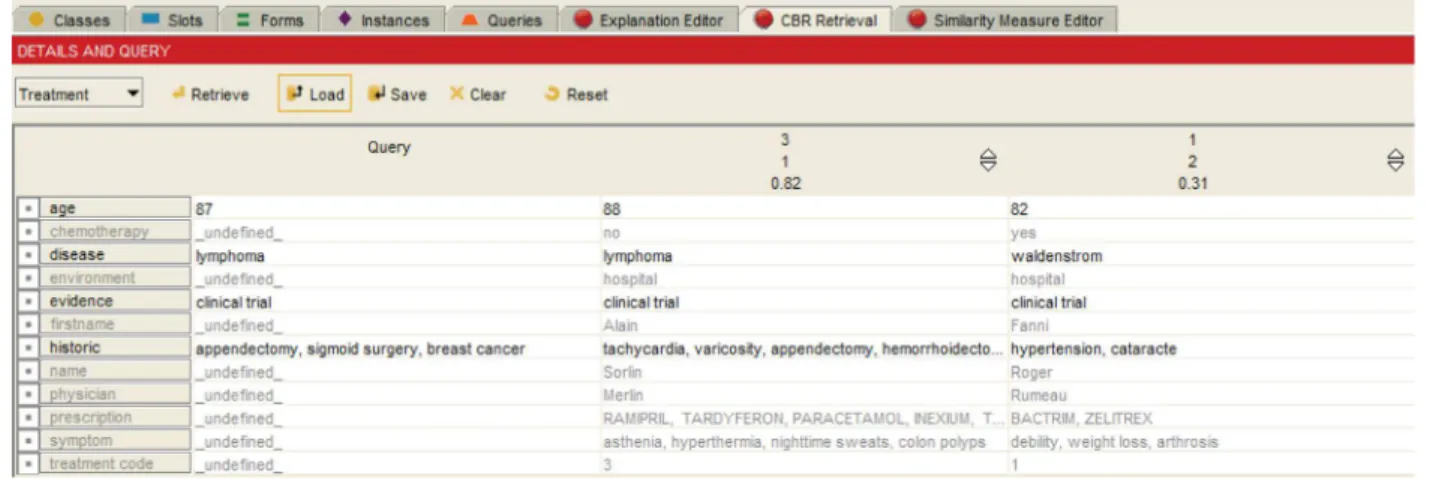
Wecan start retrieval afterediting patient information. ThisgivestheresultpresentedinFig.15.Particularly,the treat-ment1correspondswith80%intheconsideredcase.
3.2.3. Oncologycase:solutionandevidence
Wehaveanobjectiveclinicaltrialcertifyingtheeffectiveness oftreatment1andtheexperts’opinionscanconfirmthispoint (Fig.16).Inshort,theapplicationoftheadoptedapproachis illustratedbythetwofollowingsteps:
(1) Step1:simplematching:Treatment1=80%andTreatment 2=5%.
(2) Step2:matchingwithevidences:Treatment1=82%and Treatment2=31%.
3.2.4. Oncologycase:adaptation
Eachstageorfeatureofmedicationdependsononeormore attributes.Forexampledoseofmedicinesdependsontheage ofpatient,potentialdruginteractionsorallergies(Fig.17).
3.2.5. Oncologycase:retain
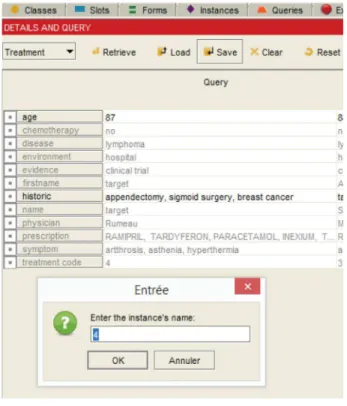
Thecurrentcaseisregisteredaccordingtothetypeofdisease (Figs.18and19).
4.
Discussion
Inthepaperwepresentedacase-basedreasoningframework appliedtomedicaldomain.
Asit is described above ourapproachbased on ontolo-giesfocusesonthemainactivitiesofmedicalprofessionals intelemedicine.Domainontologieshavealreadybeen pro-posedondiseases,drugsbuttherearefewresearchworksin telemedicineandEHealthattemptingtodefinethetreatment andbindittothepatientwithhissymptoms.
Our work istrying to embrace asa whole the medical decision system in its ecosystem (patients, treatment and diagnosistoolsavailability,availableknowledge).Themodular aspectoftheproposedframeworkallowsaneasyincremental applicationortheincorporationofnewmodulessuchasother
Fig.18–Caseedition.
typesofreasoningsystem(e.g.constraintsolversordeductive classifier)andinformationprocessing(e.g.naturallanguage processing).
In our paper, both the source and the target casesare originating fromthesame team,withcommonuses inthe namingofthesymptoms,diseasesandtreatments.Moreover oncology is a medical specialty where care is highly nor-malized trough diagnosis and treatment protocols (e.g. Tumor-Nodes-Metastasis(TNM)CancerStagingsystem[19]). Whenwewilltrythemedicalpotentialofourapproachwewill needsourceandtargetmedicalrecordsfromdifferentteams. Thenextstepwillbetoconsideramedicalspecialtywithmore heterogeneousprocesses.
Theestablishmentofthediagnosisandtreatmentisonly based on the presenceofthe symptoms and theirhistory. Thechronologyorthedynamicsofthesymptomsshouldalso betaken into account,notonlyinthepastbut asthe dis-easeprogressesandthemanagementofpatientcareshould adapt.Furthermoreitmustbearealstructurationof symp-tomsthatdonotalwayshavethesameimportance.Thiswill allowtakingintoaccountforexamplepathognomonic char-acter ofsomesymptomsandtheinterestoftheabsenceof somediscriminatingsignsforthediagnosis.
Presently, medical research is mostly based on “evi-dencebasedmedicine”[20]thatemphasizestheintegration of evidencefrom well considered and conducted research. Evidence-based practice uses guidelines and policies that incorporate evidence from scientific research in medical strategiesanddecisions.Itcanbeappliedinpopulation-level decisionsresultingfrommeta-analysiscomparingthe aver-ageeffectontwosimilarnormalpopulations,onereceiving theprocedure,theotherusedasacontrol.Thesimilarityof thepopulationsisrequiringascreeningwithinclusionand
Fig.19–Caseregistration.
exclusioncriteria.Thedifficultyisthataphysicianiscaring foranindividual withadegree ofvariationfrom the aver-age.Moreover,someoftherealpatientswouldnothavemet theinclusioncriteriaorwouldhavehadtobeexcluded.Our methodcouldprovideawaytoassessthepositiveor detrimen-taleffectsonthosepatientsoftheprocesswhileidentifying thedeviationsandprovidingrelevanthypothesesonan expla-nationofthoseeffects.
5.
Conclusion
Thisstudyprovedthepreliminaryfeasibilityofatelemedicine frameworkusingcasebasedreasoningwithevidences.This frameworkiscomplementarytothepreviousones[21–35]in termsofevidences,consideringthesensitivityandspecificity ofevidence-basedpractices.Thetechnicalarchitectureis pro-posedwithanapplicationoftheconceptualmethodinthe fieldofgeriatriconcology.
Thisarchitecture with five-step process instead offour, pointsupparticularlyevidencesandspecialist’sopinionsfor effectivenessandsafetyofthecares.Eachstepisperformed using tools from knowledge engineering and information processing(e.g. data structuration,ontology modeling,and similaritymeasure).
On the basisof four real cases (threesources and one target),wehaveimplementedeachstepofthecase-based rea-soningenrichedwithevidences.Evenifthecasesusedarereal, thefunctionalityofthistoolwillbecertifiedafterthegood gen-eralcorrelationbetweentheresultsobtainedandtheexpert’s analysis.Thiswillbedoneinfurtherworks.
Inamedium-termperspective,wewillalsoimproveand automateeachmoduleoftheproposedsystem,ouraimbeing tobuildaframeworkacceptedbyallstakeholders(e.g.patient, medicalprofessionalsandhealthcareauthorities)
Conflict
of
interest
Nonedeclared.
r
e
f
e
r
e
n
c
e
s
[1] M.Quirk,IntuitionandMetacognitioninMedicalEducation: KeystoDevelopingExpertise,SpringerPublishingCompany, Inc.,NewYork,2006.
[2] S.Montani,etal.,Diabeticpatientsmanagementexploiting case-basedreasoningtechniques,Comput.MethodsProgr. Biomed.62(3)(2000)205–218.
[3] P.Simon,W.Pellitteri,Ledécretfranc¸aisdetélémédecine: unegarantiepourlesmédecins,Eur.Res.Telemed.1(2) (2012)70–75.
[4] J.L.Kolodner,Anintroductiontocase-basedreasoning,Artif. Intell.Rev.6(1)(1992)3–34.
[5] I.Watson,Case-basedreasoningisamethodologynota technology,Knowl.BasedSyst.12(1999)303–308.
[6] M.B.Doumbouya,B.Kamsu-Foguem,H.Kenfack,C.Foguem, Aframeworkfordecisionmakingonteleexpertisewith traceabilityofthereasoning,IRBM36(1)(2014)40–51. [7] Lirmm.CoGui.http://www.lirmm.fr/cogui(lastaccessedon
10May2015).
[8] M.Singh,etal.,Applicationofhandheldtele-ECGforhealth caredeliveryinruralIndia,Int.J.Telemed.Appl.2014(2014),
http://dx.doi.org/10.1155/2014/981806,ArticleID981806,6 pages, http://www.hindawi.com/journals/ijta/2014/981806/cta/ [9] GCSTélésantéMidi-Pyrénées. https://www.telesante-midipyrenees.fr/portail/(last accessedon10May2015).
[10] A.Giorgio,Aminiaturizedmedicaldeviceforhealth monitoringandteleassistanceapplications,Int.J.Bioinform. Res.4(1)(2012)258–262.
[11] K.Dramé,G.Diallo,F.Delva,J.F.Dartigues,E.Mouillet,R. Salamon,F.Mougin,Reuseoftermino-ontologicalresources andtextcorporaforbuildingamultilingualdomain ontology:anapplicationtoAlzheimer’sdisease,J.Biomed. Inf.48(2014)171–182.
[12] T.R.Gruber,Atranslationapproachtoportableontology specifications,Knowl.Acquis.5(2)(1993)199–220. [13] G.vanHeijst,A.Th.Schreiber,B.J.Wielinga,Usingexplicit
ontologiesinKBSdevelopment,Int.J.Hum.Comput.Stud. 46(2–3)(1997)183–292.
[14] B.Tulu,S.Chatterjee,M.Maheshwari,Telemedicine taxonomy:aclassificationtool,Telemed.E-Health13(3) (2007)349–358.
[15] StanfordUniversity.Protégé.protege.stanford.edu(last accessedon10May2015).
[16] P.A.PotesRuiz,B.Kamsu-Foguem,D.Noyes,Knowledge reuseintegratingthecollaborationfromexpertsin
industrialmaintenancemanagement,Knowl.BasedSyst.50 (2013)171–186.
[17] M.Ba,G.Diallo,Large-scalebiomedicalontologymatching withServOMap,IRBM34(1)(2013)56–59.
[18] B.A.Muellera,C.Obcemea,J.Lee,S.Sim,Pilotstudyofa radiationoncologytelemedicineplatform,Radiat.Oncol.Inf. 2(1)(2010)20–30.
[19] L.H.Sobin,M.K.Gospodarowicz,C.Wittekind(Eds.),TNM ClassificationofMalignantTumors,Wiley-Blackwell,Oxford, 2009,ISBN978-1-4443-3241-4.
[20] L.A.Winters-Miner,P.S.Bolding,J.M.Hilbe,M.Goldstein,T. Hill,R.Nisbet,N.Walton,G.D.Miner,Evidence-Based Medicine,in:PracticalPredictiveAnalyticsandDecisioning SystemsforMedicine:InformaticsAccuracyand
Cost-EffectivenessforHealthcareAdministrationand DeliveryIncludingMedicalResearch,ElsevierInc.,2015,pp. 96–105(Chapter7).
[21] B.Kamsu-Foguem,P.F.Tiako,E.Mutafungwa,C.Foguem, Knowledge-basedmodellingappliedtosynucleinopathies, Eur.Geriatr.Med.(2015),
http://dx.doi.org/10.1016/j.eurger.2015.02.011.
[22] B.Kamsu-Foguem,G.Tchuenté-Foguem,C.Foguem,Using conceptualgraphsforclinicalguidelinesrepresentationand knowledgevisualization,Inform.Syst.Front.16(4)(2014) 571–589.
[23] B.Kamsu-Foguem,G.Tchuenté-Foguem,C.Foguem, Conceptualgraphoperationsforformalvisualreasoningin themedicaldomain,IRBM35(5)(2014)262–270.
[24] B.Kamsu-Foguem,G.Tchuenté-Foguem,C.Foguem, Verifyingamedicalprotocolwithtemporalgraphs:thecase ofanosocomialdisease,J.Crit.Care29(4)(2014)
690.e1–690.e9.
[25] B.Kamsu-Foguem,C.Foguem,Adversedrugreactionsin someAfricanherbalmedicine:literaturereviewand stakeholders’interview,Integr.Med.Res.3(3)(2014)126–132. [26] B.Kamsu-Foguem,G.Diallo,C.Foguem,Conceptual
graph-basedknowledgerepresentationforsupporting reasoninginAfricanTraditionalMedicine,Eng.Appl.Artif. Intell.26(4)(2013)1348–1365.
[27] K.Tafin-Kampé,B.Kamsu-Foguem,Acuteosteomyelitisdue toStaphylococcusaureusinchildren:whatisthestatusof treatmenttoday?Pediatr.Infect.Dis.5(3)(2013)122–126.
[28] B.Kamsu-Foguem,G.Tchuenté-Foguem,L.Allart,Y.Zennir, C.Vilhelm,H.Mehdaoui,D.Zitouni,H.Hubert,M.Lemdani, P.Ravaux,User-centeredvisualanalysisusingahybrid reasoningarchitectureforintensivecareunits,Decis. SupportSyst.54(1)(2012)496–509.
[29] B.Kamsu-Foguem,P.F.Tiako,L.P.Fotso,C.Foguem,Modeling foreffectivecollaborationintelemedicine,Telemat.Inform. 32(4)(2015)776–786.
[30] M.B.Doumbouya,B.Kamsu-Foguem,H.Kenfack,C.Foguem, Telemedicineusingmobiletelecommunication:towards syntacticinteroperabilityinteleexpertise,Telemat.Inform. 31(4)(2014)648–659.
[31] B.Kamsu-Foguem,Systemicmodelingintelemedicine,Eur. Res.Telemed.3(2)(2014)57–65.
[32] B.Kamsu-Foguem,Ontologicalviewintelemedicine,Eur. Res.Telemed.3(2)(2014)67–76.
[33] B.Kamsu-Foguem,C.Foguem,Couldtelemedicineenhance traditionalmedicinepractices?Eur.Res.Telemed.3(3) (2014)117–123.
[34] B.Kamsu-Foguem,C.Foguem,Telemedicineandmobile healthwithintegrativemedicineindevelopingcountries, HealthPolicyTechnol.3(4)(2014)264–271.
[35] G.Paré,M.Jaana,C.Sicotte,Systematicreviewofhome telemonitoringforchronicdiseases:theevidencebase,J. Am.Med.Inform.Assoc.14(May–Jun(3))(2007)269–277.
AlsaneSeneisaPhDstudentintheUniversityofToulouseand isregisteredattheDoctoralSchoolofAeronautics Astronau-tics(EDAA)associatedtotheISAE-SUPAERO.Hisresearcharea concernsinformationprocessingandknowledgemodellingin healthinformationtechnologywithparticularfocuson the telemedicine.HeholdsaMasterofScienceinComputer Sci-encesandTelecommunicationsattheUniversityofToulouse and also earned a professional Master degree in embed-dedandreal-timesystemsattheUniversityofToulouse.He hassomeskillsandcompetenciesinmodelingandanalysis forthedevelopmentofsoftwareapplicationsandembedded networks.
BernardKamsuFoguemiscurrentlyatenuredAssociate Pro-fessorattheNationalEngineeringSchoolofTarbes(ENIT)of NationalPolytechnicInstituteofToulouse(INPT)and under-takesresearchintheProductionEngineeringLaboratory(LGP) ofENIT-INPT,aresearchentity(EA1905)oftheUniversityof Toulouse.Heisavisitingscholarinsomerenowned universi-ties:UnitedKingdom(e.g.OxfordBrookesUniversity,Oxford), Finland(e.g.AaltoUniversity,HelsinkiUniversityof Technol-ogy,VTTTechnicalResearchCentreofTampere,Universityof Oulu,ÅboakademiofTurkuUniversity).Heisalsoinvolved in the thematic group: e-Health of InterOP-VLab (Interna-tional VirtualLaboratoryforEnterprise Interoperability).He isamemberofInternationalEditorialReviewerBoardof Arti-ficialIntelligenceResearchandareviewerforalargenumber ofinternationalscientificjournalssuchasKnowledge-Based Systems, Engineering Applications ofArtificial Intelligence, InternationalJournalofProductionResearch,Journalof Intel-ligent Manufacturing, Computer Methods and Programs in Biomedicine, Computers in Biology and Medicine, Interac-tingwithComputers,Sensorsand KnowledgeManagement Research& Practice. Hegot the “accreditationto supervise research”, abbreviated HDR from University of Toulousein 2013. He has a Master’s in Operational Research, Combi-natoricsand Optimization(2000)from National Polytechnic Institute ofGrenoble,and a PhDin ComputerScience and Automation(2004)fromtheUniversityofMontpellier2.His currentinterestsareinKnowledgeDiscoveryandData Min-ing, Knowledge Representation, Formal Visual Reasoning, Ontology-based Semantic Analysis,Knowledge Exploitation for remote Collaboration, Decision Support Systems and
IntelligentSystems.Theapplicationrangeisextensiveand includesContinuousImprovementProcesses,Reliability cen-teredMaintenance,BuildingInformationModelingandHealth InformationSystems.
Dr. Pierre Rumeau MD PhD is a consulting geriatrician at University Hospital Toulouse and is the head of La Grave Gerontechnology Laboratory, Gerontopole/UMR1027 Inserm-Toulouse University. He is asenior lecturer inrisk
managementfortheinternationalmasterofmechatronic sys-temsforrehabilitation(Paris6-Brescia).HehasaPhDinModel, MethodsandAlgorythmsinbiology,healthandenvironment (2010)fromtheUniversityofGrenoble.Hehasbeeninvolved inseveralscientificprojectsrelatingtohealth,telemedicine, compensationandtechnology(e.g.AILISA,DOMEO, Health-ware,Homecare,PréDICA,MIRAS,Monimad,RESATER,Riddle, TANDEM,UR-Safe).