DOYEN 1962 – 1 1969 – 1 1974 – 1 1981 – 1 1989 – 1 1997 – 2 2003 - 2 ADMIN Doyen Vice-Do Vice-Doy Vice-Doy Secrétai NS HONORA 1969 : 1974 : 1981 : 1989 : 1997 : 2003 : 2013 : NISTRATIO Professeur oyen chargé Professeur oyen chargé d Professeur oyen chargé d Professeur ire Général Mr. Moham U FACULT AIRES : Professeur A Professeur A Professeur B Professeur T Professeur M Professeur A Professeur N ON : Mohamed A des Affaires Brahim LE de la Recher Toufiq DAK des Affaires Jamal TAO med KARRA UNIVERSITE M TE DE MEDEC Abdelmalek Abdellatif BE Bachir LAZR Taieb CHKIL Mohamed Ta Abdelmajid B Najia HAJJA ADNAOUI Académiqu EKEHAL rche et de la KKA Spécifiques OUFIK A MOHAMME CINE ET DE P FARAJ ERBICH RAK LI ahar ALAOU BELMAHI AJ – HASSOU ues et estudia Coopération s à la Pharm D V DE RABA PHARMACIE UI UNI antines n acie AT ‐ RABAT
1 - ENSEIGNANTS-CHERCHEURS MEDECINS ET PHARMACIENS
PROFESSEURS :
Décembre 1984
Pr. MAAOUNI Abdelaziz Médecine Interne – Clinique Royale
Pr. MAAZOUZI Ahmed Wajdi Anesthésie -Réanimation Pr. SETTAF Abdellatif Pathologie Chirurgicale
Novembre et Décembre 1985
Pr. BENSAID Younes Pathologie Chirurgicale
Janvier, Février et Décembre 1987
Pr. LACHKAR Hassan Médecine Interne
Pr. YAHYAOUI Mohamed Neurologie
Décembre 1989
Pr. ADNAOUI Mohamed Médecine Interne –Doyen de la FMPR
Pr. OUAZZANI Taïbi Mohamed Réda Neurologie
Janvier et Novembre 1990
Pr. HACHIM Mohammed* Médecine-Interne
Pr. KHARBACH Aîcha Gynécologie -Obstétrique
Pr. TAZI Saoud Anas Anesthésie Réanimation
Février Avril Juillet et Décembre 1991
Pr. AZZOUZI Abderrahim Anesthésie Réanimation- Doyen de FMPO
Pr. BAYAHIA Rabéa Néphrologie
Pr. BELKOUCHI Abdelkader Chirurgie Générale
Pr. BENCHEKROUN Belabbes Abdellatif Chirurgie Générale
Pr. BENSOUDA Yahia Pharmacie galénique
Pr. BERRAHO Amina Ophtalmologie
Pr. BEZAD Rachid
Gynécologie Obstétrique Méd. Chef Maternité des Orangers
Pr. CHERRAH Yahia Pharmacologie
Pr. CHOKAIRI Omar Histologie Embryologie
Pr. KHATTAB Mohamed Pédiatrie
Pr. SOULAYMANI Rachida Pharmacologie- Dir. du Centre National PV Rabat
Pr. TAOUFIK Jamal Chimie thérapeutique V.D à la pharmacie+Dir. du CEDOC +
Directeur du Médicament
Décembre 1992
Pr. AHALLAT Mohamed Chirurgie Générale Doyen de FMPT
Pr. BENSOUDA Adil Anesthésie Réanimation
Pr. CHAHED OUAZZANI Laaziza Gastro-Entérologie
Pr. CHRAIBI Chafiq Gynécologie Obstétrique
Pr. EL OUAHABI Abdessamad Neurochirurgie
Pr. FELLAT Rokaya Cardiologie
Pr. GHAFIR Driss* Médecine Interne
Pr. JIDDANE Mohamed Anatomie
Pr. TAGHY Ahmed Chirurgie Générale
Pr. ZOUHDI Mimoun Microbiologie
Mars 1994
Pr. BENJAAFAR Noureddine Radiothérapie
Pr. BEN RAIS Nozha Biophysique
Pr. CAOUI Malika Biophysique
Pr. CHRAIBI Abdelmjid
Endocrinologie et Maladies Métaboliques Doyen de la FMPA
Pr. EL AMRANI Sabah Gynécologie Obstétrique Pr. EL BARDOUNI Ahmed Traumato-Orthopédie Pr. EL HASSANI My Rachid Radiologie
Pr. ERROUGANI Abdelkader Chirurgie Générale – Directeur du CHIS-Rabat
Pr. ESSAKALI Malika Immunologie
Pr. ETTAYEBI Fouad Chirurgie Pédiatrique
Pr. HASSAM Badredine Dermatologie
Pr. IFRINE Lahssan Chirurgie Générale
Pr. MAHFOUD Mustapha Traumatologie – Orthopédie
Pr. RHRAB Brahim Gynécologie –Obstétrique
Pr. SENOUCI Karima Dermatologie
Mars 1994
Pr. ABBAR Mohamed* Urologie Directeur Hôpital My Ismail Meknès Pr. ABDELHAK M’barek Chirurgie – Pédiatrique
Pr. BENTAHILA Abdelali Pédiatrie
Pr. BENYAHIA Mohammed Ali Gynécologie – Obstétrique Pr. BERRADA Mohamed Saleh Traumatologie – Orthopédie Pr. CHERKAOUI Lalla Ouafae Ophtalmologie
Pr. LAKHDAR Amina Gynécologie Obstétrique
Mars 1995
Pr. ABOUQUAL Redouane Réanimation Médicale
Pr. AMRAOUI Mohamed Chirurgie Générale
Pr. BAIDADA Abdelaziz Gynécologie Obstétrique
Pr. BARGACH Samir Gynécologie Obstétrique
Pr. DRISSI KAMILI Med Nordine* Anesthésie Réanimation Pr. EL MESNAOUI Abbes Chirurgie Générale Pr. ESSAKALI HOUSSYNI Leila Oto-Rhino-Laryngologie
Pr. HDA Abdelhamid* Cardiologie Inspecteur du Service de Santé des FAR Pr. IBEN ATTYA ANDALOUSSI Ahmed Urologie
Pr. OUAZZANI CHAHDI Bahia Ophtalmologie
Pr. SEFIANI Abdelaziz Génétique
Pr. ZEGGWAGH Amine Ali Réanimation Médicale
Décembre 1996
Pr. AMIL Touriya* Radiologie
Pr. BELKACEM Rachid Chirurgie Pédiatrie Pr. BOULANOUAR Abdelkrim Ophtalmologie Pr. EL ALAMI EL FARICHA EL Hassan Chirurgie Générale
Pr. GAOUZI Ahmed Pédiatrie
Pr. MAHFOUDI M’barek* Radiologie
Pr. OUZEDDOUN Naima Néphrologie
Pr. ZBIR EL Mehdi* Cardiologie DirecteurHôp.Mil. d’Instruction Med V Rabat
Novembre 1997
Pr. ALAMI Mohamed Hassan Gynécologie-Obstétrique
Pr. BEN SLIMANE Lounis Urologie
Pr. BIROUK Nazha Neurologie
Pr. ERREIMI Naima Pédiatrie
Pr. FELLAT Nadia Cardiologie
Pr. KADDOURI Noureddine Chirurgie Pédiatrique
Pr. KOUTANI Abdellatif Urologie
Pr. LAHLOU Mohamed Khalid Chirurgie Générale
Pr. MAHRAOUI CHAFIQ Pédiatrie
Pr. TOUFIQ Jallal Psychiatrie Directeur Hôp.Ar-razi Salé
Pr. YOUSFI MALKI Mounia Gynécologie Obstétrique
Novembre 1998
Pr. BENOMAR ALI Neurologie Doyen de la FMP Abulcassis
Pr. BOUGTAB Abdesslam Chirurgie Générale Pr. ER RIHANI Hassan Oncologie Médicale
Pr. BENKIRANE Majid* Hématologie
Janvier 2000
Pr. ABID Ahmed* Pneumo-phtisiologie
Pr. AIT OUAMAR Hassan Pédiatrie
Pr. BENJELLOUN Dakhama Badr.Sououd Pédiatrie
Pr. BOURKADI Jamal-Eddine Pneumo-phtisiologie Directeur Hôp. My Youssef Pr. CHARIF CHEFCHAOUNI Al Montacer Chirurgie Générale
Pr. ECHARRAB El Mahjoub Chirurgie Générale Pr. EL FTOUH Mustapha Pneumo-phtisiologie
Pr. EL MOSTARCHID Brahim* Neurochirurgie
Pr. MAHMOUDI Abdelkrim* Anesthésie-Réanimation Pr. TACHINANTE Rajae Anesthésie-Réanimation Pr. TAZI MEZALEK Zoubida Médecine Interne
Novembre 2000
Pr. AIDI Saadia Neurologie
Pr. AJANA Fatima Zohra Gastro-Entérologie
Pr. BENAMR Said Chirurgie Générale
Pr. CHERTI Mohammed Cardiologie
Pr. ECH-CHERIF EL KETTANI Selma Anesthésie-Réanimation Pr. EL HASSANI Amine Pédiatrie - Directeur Hôp.Cheikh Zaid
Pr. EL KHADER Khalid Urologie
Pr. EL MAGHRAOUI Abdellah* Rhumatologie
Pr. GHARBI Mohamed El Hassan Endocrinologie et Maladies Métaboliques
Pr. MDAGHRI ALAOUI Asmae Pédiatrie
Pr. ROUIMI Abdelhadi* Neurologie
Décembre 2000
Pr.ZOHAIR ABDELLAH * ORL
Pr. BALKHI Hicham* Anesthésie-Réanimation
Pr. BENABDELJLIL Maria Neurologie
Pr. BENAMAR Loubna Néphrologie
Pr. BENAMOR Jouda Pneumo-phtisiologie
Pr. BENELBARHDADI Imane Gastro-Entérologie
Pr. BENNANI Rajae Cardiologie
Pr. BENOUACHANE Thami Pédiatrie
Pr. BEZZA Ahmed* Rhumatologie
Pr. BOUCHIKHI IDRISSI Med Larbi Anatomie Pr. BOUMDIN El Hassane* Radiologie
Pr. CHAT Latifa Radiologie
Pr. DRISSI Sidi Mourad* Radiologie
Pr. EL HIJRI Ahmed Anesthésie-Réanimation
Pr. EL MAAQILI Moulay Rachid Neuro-Chirurgie
Pr. EL MADHI Tarik Chirurgie-Pédiatrique
Pr. EL OUNANI Mohamed Chirurgie Générale
Pr. ETTAIR Said Pédiatrie - Directeur Hôp. d’EnfantsRabat
Pr. GAZZAZ Miloudi* Neuro-Chirurgie
Pr. HRORA Abdelmalek Chirurgie Générale
Pr. KABBAJ Saad Anesthésie-Réanimation
Pr. KABIRI EL Hassane* Chirurgie Thoracique Pr. LAMRANI Moulay Omar Traumatologie Orthopédie
Pr. LEKEHAL Brahim Chirurgie Vasculaire Périphérique Pr. MAHASSIN Fattouma* Médecine Interne
Pr. MEDARHRI Jalil Chirurgie Générale
Pr. MIKDAME Mohammed* Hématologie Clinique
Pr. MOHSINE Raouf Chirurgie Générale
Pr. NOUINI Yassine Urologie - Directeur Hôpital Ibn Sina
Pr. SABBAH Farid Chirurgie Générale
Pr. SEFIANI Yasser Chirurgie Vasculaire Périphérique Pr. TAOUFIQ BENCHEKROUN Soumia Pédiatrie
Décembre 2002
Pr. AL BOUZIDI Abderrahmane* Anatomie Pathologique
Pr. AMEUR Ahmed * Urologie
Pr. AMRI Rachida Cardiologie
Pr. AOURARH Aziz* Gastro-Entérologie
Pr. BAMOU Youssef * Biochimie-Chimie
Pr. BELMEJDOUB Ghizlene* Endocrinologie et Maladies Métaboliques
Pr. BENZEKRI Laila Dermatologie
Pr. BENZZOUBEIR Nadia Gastro-Entérologie Pr. BERNOUSSI Zakiya Anatomie Pathologique Pr. BICHRA Mohamed Zakariya* Psychiatrie
Pr. CHOHO Abdelkrim * Chirurgie Générale
Pr. CHKIRATE Bouchra Pédiatrie
Pr. EL ALAMI EL Fellous Sidi Zouhair Chirurgie Pédiatrique Pr. EL HAOURI Mohamed * Dermatologie
Pr. FILALI ADIB Abdelhai Gynécologie Obstétrique
Pr. HAJJI Zakia Ophtalmologie
Pr. IKEN Ali Urologie
Pr. KRIOUILE Yamina Pédiatrie
Pr. MABROUK Hfid* Traumatologie Orthopédie
Pr. MOUSSAOUI RAHALI Driss* Gynécologie Obstétrique Pr. OUJILAL Abdelilah Oto-Rhino-Laryngologie Pr. RACHID Khalid * Traumatologie Orthopédie
Pr. RAISS Mohamed Chirurgie Générale
Pr. RGUIBI IDRISSI Sidi Mustapha* Pneumo-phtisiologie
Pr. RHOU Hakima Néphrologie
Pr. SIAH Samir * Anesthésie Réanimation
Pr. THIMOU Amal Pédiatrie
Pr. ZENTAR Aziz* Chirurgie Générale
Janvier 2004
Pr. ABDELLAH El Hassan Ophtalmologie
Pr. AMRANI Mariam Anatomie Pathologique
Pr. BENBOUZID Mohammed Anas Oto-Rhino-Laryngologie Pr. BENKIRANE Ahmed* Gastro-Entérologie
Pr. BOULAADAS Malik Stomatologie et Chirurgie Maxillo-faciale
Pr. BOURAZZA Ahmed* Neurologie
Pr. CHAGAR Belkacem* Traumatologie Orthopédie
Pr. CHERRADI Nadia Anatomie Pathologique
Pr. EL FENNI Jamal* Radiologie
Pr. EL HANCHI ZAKI Gynécologie Obstétrique Pr. EL KHORASSANI Mohamed Pédiatrie
Pr. EL YOUNASSI Badreddine* Cardiologie
Pr. HACHI Hafid Chirurgie Générale
Pr. JABOUIRIK Fatima Pédiatrie
Pr. KHARMAZ Mohamed Traumatologie Orthopédie Pr. MOUGHIL Said Chirurgie Cardio-Vasculaire Pr. OUBAAZ Abdelbarre * Ophtalmologie
Pr. TARIB Abdelilah* Pharmacie Clinique
Pr. TIJAMI Fouad Chirurgie Générale
Pr. ZARZUR Jamila Cardiologie
Janvier 2005
Pr. ABBASSI Abdellah Chirurgie Réparatrice et Plastique Pr. AL KANDRY Sif Eddine* Chirurgie Générale
Pr. ALLALI Fadoua Rhumatologie
Pr. AMAZOUZI Abdellah Ophtalmologie
Pr. AZIZ Noureddine* Radiologie
Pr. BARKAT Amina Pédiatrie
Pr. BENYASS Aatif Cardiologie
Pr. DOUDOUH Abderrahim* Biophysique
Pr. EL HAMZAOUI Sakina * Microbiologie
Pr. HAJJI Leila Cardiologie(mise en disponibilité)
Pr. HESSISSEN Leila Pédiatrie
Pr. JIDAL Mohamed* Radiologie
Pr. LAAROUSSI Mohamed Chirurgie Cardio-vasculaire
Pr. LYAGOUBI Mohammed Parasitologie
Pr. RAGALA Abdelhak Gynécologie Obstétrique
Pr. SBIHI Souad Histo-Embryologie Cytogénétique
Pr. ZERAIDI Najia Gynécologie Obstétrique
AVRIL 2006
Pr. ACHEMLAL Lahsen* Rhumatologie
Pr. AKJOUJ Said* Radiologie
Pr. BELMEKKI Abdelkader* Hématologie
Pr. BENCHEIKH Razika O.R.L
Pr. BIYI Abdelhamid* Biophysique
Pr. BOUHAFS Mohamed El Amine Chirurgie - Pédiatrique
Pr. BOULAHYA Abdellatif* Chirurgie Cardio – Vasculaire. Pr. CHENGUETI ANSARI Anas Gynécologie Obstétrique
Pr. DOGHMI Nawal Cardiologie
Pr. FELLAT Ibtissam Cardiologie
Pr. FAROUDY Mamoun Anesthésie Réanimation
Pr. HARMOUCHE Hicham Médecine Interne
Pr. HANAFI Sidi Mohamed* Anesthésie Réanimation Pr. IDRISS LAHLOU Amine* Microbiologie
Pr. JROUNDI Laila Radiologie
Pr. KARMOUNI Tariq Urologie
Pr. KILI Amina Pédiatrie
Pr. KISRA Hassan Psychiatrie
Pr. KISRA Mounir Chirurgie – Pédiatrique
Pr. LAATIRIS Abdelkader* Pharmacie Galénique Pr. LMIMOUNI Badreddine* Parasitologie
Pr. MANSOURI Hamid* Radiothérapie
Pr. OUANASS Abderrazzak Psychiatrie
Pr. SAFI Soumaya* Endocrinologie
Pr. SEKKAT Fatima Zahra Psychiatrie
Pr. SOUALHI Mouna Pneumo – Phtisiologie
Pr. TELLAL Saida* Biochimie
Décembre 2006
Pr SAIR Khalid Chirurgie générale Dir. Hôp.Av.Marrakech
Octobre 2007
Pr. ABIDI Khalid Réanimation médicale
Pr. ACHACHI Leila Pneumo phtisiologie
Pr. ACHOUR Abdessamad* Chirurgie générale
Pr. AIT HOUSSA Mahdi * Chirurgie cardio vasculaire Pr. AMHAJJI Larbi * Traumatologie orthopédie
Pr. AOUFI Sarra Parasitologie
Pr. BAITE Abdelouahed * Anesthésie réanimation Directeur ERSSM Pr. BALOUCH Lhousaine * Biochimie-chimie
Pr. BENZIANE Hamid * Pharmacie clinique Pr. BOUTIMZINE Nourdine Ophtalmologie Pr. CHERKAOUI Naoual * Pharmacie galénique Pr. EHIRCHIOU Abdelkader * Chirurgie générale
Pr. EL BEKKALI Youssef * Chirurgie cardio-vasculaire
Pr. EL ABSI Mohamed Chirurgie générale
Pr. EL MOUSSAOUI Rachid Anesthésie réanimation
Pr. EL OMARI Fatima Psychiatrie
Pr. GHARIB Noureddine Chirurgie plastique et réparatrice
Pr. HADADI Khalid * Radiothérapie
Pr. ICHOU Mohamed * Oncologie médicale
Pr. ISMAILI Nadia Dermatologie
Pr. KEBDANI Tayeb Radiothérapie
Pr. LALAOUI SALIM Jaafar * Anesthésie réanimation
Pr. LOUZI Lhoussain * Microbiologie
Pr. MADANI Naoufel Réanimation médicale
Pr. MAHI Mohamed * Radiologie
Pr. MARC Karima Pneumo phtisiologie
Pr. MASRAR Azlarab Hématologie biologique
Pr. MRANI Saad * Virologie
Pr. OUZZIF Ez zohra * Biochimie-chimie
Pr. RABHI Monsef * Médecine interne
Pr. RADOUANE Bouchaib* Radiologie
Pr. SEFFAR Myriame Microbiologie
Pr. SEKHSOKH Yessine * Microbiologie
Pr. SIFAT Hassan * Radiothérapie
Pr. TABERKANET Mustafa * Chirurgie vasculaire périphérique
Pr. TACHFOUTI Samira Ophtalmologie
Pr. TAJDINE Mohammed Tariq* Chirurgie générale Pr. TANANE Mansour * Traumatologie-orthopédie
Pr. TOUATI Zakia Cardiologie
Décembre 2008
Pr TAHIRI My El Hassan* Chirurgie Générale
Mars 2009
Pr. ABOUZAHIR Ali * Médecine interne
Pr. AGADR Aomar * Pédiatrie
Pr. AIT ALI Abdelmounaim * Chirurgie Générale Pr. AIT BENHADDOU El Hachmia Neurologie
Pr. AKHADDAR Ali * Neuro-chirurgie
Pr. ALLALI Nazik Radiologie
Pr. AMINE Bouchra Rhumatologie
Pr. ARKHA Yassir Neuro-chirurgie Directeur Hôp.des Spécialités Pr. BELYAMANI Lahcen* Anesthésie Réanimation
Pr. BJIJOU Younes Anatomie
Pr. BOUHSAIN Sanae * Biochimie-chimie
Pr. BOUI Mohammed * Dermatologie
Pr. BOUNAIM Ahmed * Chirurgie Générale
Pr. BOUSSOUGA Mostapha * Traumatologie-orthopédie
Pr. CHTATA Hassan Toufik * Chirurgie Vasculaire Périphérique Pr. DOGHMI Kamal * Hématologie clinique
Pr. EL MALKI Hadj Omar Chirurgie Générale Pr. EL OUENNASS Mostapha* Microbiologie
Pr. ENNIBI Khalid * Médecine interne
Pr. FATHI Khalid Gynécologie obstétrique
Pr. HASSIKOU Hasna * Rhumatologie
Pr. KABBAJ Nawal Gastro-entérologie
Pr. KABIRI Meryem Pédiatrie
Pr. KARBOUBI Lamya Pédiatrie
Pr. LAMSAOURI Jamal * Chimie Thérapeutique Pr. MARMADE Lahcen Chirurgie Cardio-vasculaire
Pr. MESKINI Toufik Pédiatrie
Pr. MESSAOUDI Nezha * Hématologie biologique
Pr. MSSROURI Rahal Chirurgie Générale
Pr. NASSAR Ittimade Radiologie
Pr. OUKERRAJ Latifa Cardiologie
Pr. RHORFI Ismail Abderrahmani * Pneumo-Phtisiologie
Octobre 2010
Pr. AMEZIANE Taoufiq* Médecine Interne Pr. BELAGUID Abdelaziz Physiologie
Pr. CHADLI Mariama* Microbiologie
Pr. CHEMSI Mohamed* Médecine Aéronautique
Pr. DAMI Abdellah* Biochimie- Chimie
Pr. DARBI Abdellatif* Radiologie
Pr. DENDANE Mohammed Anouar Chirurgie Pédiatrique
Pr. EL HAFIDI Naima Pédiatrie
Pr. EL KHARRAS Abdennasser* Radiologie
Pr. EL MAZOUZ Samir Chirurgie Plastique et Réparatrice
Pr. EL SAYEGH Hachem Urologie
Pr. ERRABIH Ikram Gastro-Entérologie
Pr. LAMALMI Najat Anatomie Pathologique
Pr. MOSADIK Ahlam Anesthésie Réanimation
Pr. MOUJAHID Mountassir* Chirurgie Générale
Pr. NAZIH Mouna* Hématologie
Pr. ZOUAIDIA Fouad Anatomie Pathologique
Décembre 2010
Pr.ZNATI Kaoutar Anatomie Pathologique
Mai 2012
Pr. AMRANI Abdelouahed Chirurgie pédiatrique Pr. ABOUELALAA Khalil * Anesthésie Réanimation Pr. BENCHEBBA Driss * Traumatologie-orthopédie Pr. DRISSI Mohamed * Anesthésie Réanimation Pr. EL ALAOUI MHAMDI Mouna Chirurgie Générale Pr. EL KHATTABI Abdessadek * Médecine Interne Pr. EL OUAZZANI Hanane * Pneumophtisiologie
Pr. ER-RAJI Mounir Chirurgie Pédiatrique
Pr. JAHID Ahmed Anatomie Pathologique
Pr. MEHSSANI Jamal * Psychiatrie
Pr. RAISSOUNI Maha * Cardiologie
* Enseignants Militaires Février 2013
Pr.AHID Samir Pharmacologie
Pr.AIT EL CADI Mina Toxicologie
Pr.AMRANI HANCHI Laila Gastro-Entérologie
Pr.AMOR Mourad Anesthésie Réanimation
Pr.AWAB Almahdi Anesthésie Réanimation
Pr.BELAYACHI Jihane Réanimation Médicale
Pr.BENCHEKROUN Laila Biochimie-Chimie
Pr.BENKIRANE Souad Hématologie
Pr.BENNANA Ahmed* Informatique Pharmaceutique Pr.BENSGHIR Mustapha * Anesthésie Réanimation
Pr.BENYAHIA Mohammed * Néphrologie
Pr.BOUATIA Mustapha Chimie Analytique et Bromatologie Pr.BOUABID Ahmed Salim* Traumatologie orthopédie
Pr BOUTARBOUCH Mahjouba Anatomie
Pr.CHAIB Ali * Cardiologie
Pr.DENDANE Tarek Réanimation Médicale
Pr.DINI Nouzha * Pédiatrie
Pr.ECH-CHERIF EL KETTANI Mohamed Ali Anesthésie Réanimation Pr.ECH-CHERIF EL KETTANI Najwa Radiologie
Pr.EL FATEMI NIZARE Neuro-chirurgie
Pr.EL GUERROUJ Hasnae Médecine Nucléaire
Pr.EL HARTI Jaouad Chimie Thérapeutique
Pr.EL JAOUDI Rachid * Toxicologie
Pr.EL KABABRI Maria Pédiatrie
Pr.EL KHANNOUSSI Basma Anatomie Pathologique
Pr.EL KHLOUFI Samir Anatomie
Pr.EL KORAICHI Alae Anesthésie Réanimation
Pr.EN-NOUALI Hassane * Radiologie
Pr.ERRGUIG Laila Physiologie
Pr.FIKRI Meryem Radiologie
Pr.GHFIR Imade Médecine Nucléaire
Pr.IMANE Zineb Pédiatrie
Pr.IRAQI Hind Endocrinologie et maladies métaboliques
Pr.KABBAJ Hakima Microbiologie
Pr.KADIRI Mohamed * Psychiatrie
Pr.MAAMAR Mouna Fatima Zahra Médecine Interne
Pr.MEDDAH Bouchra Pharmacologie
Pr.MELHAOUI Adyl Neuro-chirurgie
Pr.MRABTI Hind Oncologie Médicale
Pr.NEJJARI Rachid Pharmacognosie
Pr.OUBEJJA Houda Chirugie Pédiatrique
Pr.OUKABLI Mohamed * Anatomie Pathologique
Pr.RAHALI Younes Pharmacie Galénique
Pr.RATBI Ilham Génétique
Pr.RAHMANI Mounia Neurologie
Pr.REDA Karim * Ophtalmologie
Pr.REGRAGUI Wafa Neurologie
Pr.RKAIN Hanan Physiologie
PROFESSEURS AGREGES :
DECEMBRE 2014
Pr. ABILKASSEM Rachid* Pédiatrie
Pr. AIT BOUGHIMA Fadila Médecine Légale
Pr. BEKKALI Hicham * Anesthésie-Réanimation
Pr. BENAZZOU Salma Chirurgie Maxillo-Faciale
Pr. BOUABDELLAH Mounya Biochimie-Chimie
Pr.ROUAS Lamiaa Anatomie Pathologique
Pr.ROUIBAA Fedoua * Gastro-Entérologie
Pr SALIHOUN Mouna Gastro-Entérologie
Pr.SAYAH Rochde Chirurgie Cardio-Vasculaire
Pr.SEDDIK Hassan * Gastro-Entérologie
Pr.ZERHOUNI Hicham Chirurgie Pédiatrique
Pr.ZINE Ali* Traumatologie Orthopédie
AVRIL 2013
Pr.EL KHATIB MOHAMED KARIM * Stomatologie et Chirurgie Maxillo-faciale
MAI 2013
Pr.BOUSLIMAN Yassir Toxicologie
MARS 2014
Pr. ACHIR Abdellah Chirurgie Thoracique
Pr.BENCHAKROUN Mohammed * Traumatologie- Orthopédie
Pr.BOUCHIKH Mohammed Chirurgie Thoracique
Pr. EL KABBAJ Driss * Néphrologie
Pr. EL MACHTANI IDRISSI Samira * Biochimie-Chimie
Pr. HARDIZI Houyam Histologie- Embryologie-Cytogénétique
Pr. HASSANI Amale * Pédiatrie
Pr. HERRAK Laila Pneumologie
Pr. JANANE Abdellah * Urologie
Pr. JEAIDI Anass * Hématologie Biologique
Pr. KOUACH Jaouad* Génycologie-Obstétrique
Pr. LEMNOUER Abdelhay* Microbiologie
Pr. MAKRAM Sanaa * Pharmacologie
Pr. OULAHYANE Rachid* Chirurgie Pédiatrique
Pr. RHISSASSI Mohamed Jaafar CCV
Pr. SABRY Mohamed* Cardiologie
Pr. SEKKACH Youssef* Médecine Interne
Pr. TAZI MOUKHA Zakia Génécologie-Obstétrique
AVRIL 2014
Pr. BOUCHRIK Mourad* Parasitologie
Pr. DERRAJI Soufiane* Pharmacie Clinique
Pr. DOBLALI Taoufik* Microbiologie
Pr. EL AYOUBI EL IDRISSI Ali Anatomie
Pr. EL GHADBANE Abdedaim Hatim* Anesthésie-Réanimation
Pr. EL MARJANY Mohammed* Radiothérapie
Pr. FEJJAL Nawfal Chirurgie Réparatrice et Plastique
Pr. JAHIDI Mohamed* O.R.L
Pr. LAKHAL Zouhair* Cardiologie
Pr. OUDGHIRI NEZHA Anesthésie-Réanimation
Pr. RAMI Mohamed Chirurgie Pédiatrique
Pr. SABIR Maria Psychiatrie
Pr. SBAI IDRISSI Karim* Médecine préventive, santé publique et Hyg.
AOUT 2015
Pr. MEZIANE Meryem Dermatologie
Pr. TAHRI Latifa Rhumatologie
JANVIER 2016
Pr. BENKABBOU Amine Chirurgie Générale
Pr. EL ASRI Fouad* Ophtalmologie
Pr. ERRAMI Noureddine* O.R.L
Pr. NITASSI Sophia O.R.L
JUIN 2017
Pr. ABI Rachid* Microbiologie
Pr. ASFALOU Ilyasse* Cardiologie
Pr. BOUAYTI El Arbi* Médecine préventive, santé publique et Hyg.
Pr. BOUTAYEB Saber Oncologie Médicale
Pr. EL GHISSASSI Ibrahim Oncologie Médicale
Pr. OURAINI Saloua* O.R.L
Pr. RAZINE Rachid Médecine préventive, santé publique et Hyg.
Pr. ZRARA Abdelhamid* Immunologie
2 - ENSEIGNANTS-CHERCHEURS SCIENTIFIQUES
PROFESSEURS/Prs. HABILITES
Pr. ABOUDRAR Saadia Physiologie
Pr. ALAMI OUHABI Naima Biochimie-chimie
Pr. ALAOUI KATIM Pharmacologie
Pr. ALAOUI SLIMANI Lalla Naïma Histologie-Embryologie
Pr. ANSAR M’hammed Chimie Organique et Pharmacie Chimique
Pr .BARKIYOU Malika Histologie-Embryologie
Pr. BOUHOUCHE Ahmed Génétique Humaine
Pr. BOUKLOUZE Abdelaziz Applications Pharmaceutiques Pr. CHAHED OUAZZANI Lalla Chadia Biochimie-chimie
Pr. DAKKA Taoufiq Physiologie
Pr. FAOUZI Moulay El Abbes Pharmacologie
Pr. IBRAHIMI Azeddine Biologie moléculaire/Biotechnologie
Pr. KHANFRI Jamal Eddine Biologie
Pr. OULAD BOUYAHYA IDRISSI Med Chimie Organique
Pr. REDHA Ahlam Chimie
Pr. TOUATI Driss Pharmacognosie
Pr. ZAHIDI Ahmed Pharmacologie
Mise à jour le 10/10/2018 Khaled Abdellah
D
To my father El Hassan Katir;
My role model, my rock, my inspiration, my pride, and joy. Your heart is THE purest one I know in this life as well as THE smartest. I can never thank you enough for all the hard work and sacrifices you have done for our family, for me. For the nights you spend
awake so we can lie down at peace sleeping, for the cloth you take off your back so we can be at warm, for the smile you put on your face so we can’t see the worries of the
world. I thank you from the bottom of my heart. You thought me to be kind to my enemies, to always have faith and see the good side of things, to care from far and never
expect something in return because this is the true meaning of generosity. You are kind enough to let me be myself on any occasion, to speak my truth, to explore the world while
always keeping in mind that facts and science are our best allay. I pray to come close to repay you all the love and sweetness you aspired to create in our home. May God protect
you! I don’t know what I would have become if I never had the amazing father and mentor that you are.
To my mother Fatima Bentaher;
Boy, we had our differences! But that what made me strong and independent with a sense of self-awareness, and for that, I will forever be grateful. Mum, you are the strongest person
I know. You are also so resourceful and smart I wonder sometimes “How did she come up with that idea?!” I see in you the woman I aspire to become. You’ve always pouched us to achieve the best, to be perfectionists, to never settle for less what we deserve. When I see in your courage and determination a great motivation to try changing the world to be better, I
want to do the same, even on a small scale, and especially do that with a great sense of humour along the way. Thank you a million times for putting your work on the side in moments when I needed you. And thank you for making me feel that there is always
For my sister Kawtar Katir;
Kouka, my sister, my friend, and my partner in crime always and forever. Whenever life gets tough, you are my go-to person, because you can be more rational and strategic in moments
of distress than I am. I love you beyond words can describe and beyond distances. You are always on my mind. Thank you for everything you have done for me.
For my little sister Doha Katir;
You are a WONDERFUL spirit. At last, I thank my parents for having you! You cannot imagine how much I love you and adore you. You are so kind I am amazed sometimes how people like you could even still exist. You are extremely smart and generous and boy you are courageous! We will always have each others’ backs and that is not something you see very
To my grandpa the artist Idriss Bentaher and my grandma
Aphrodite Lalla Aicha Derraz;
The ones I consider as my second parents. I am thankful everyday for having alive still. You raised me like your own surrounded with unconditional love and warm. You’ve always cared for me, asked about me and worried about me. You are my BIGGEST cheerleads, more
than my parents are. You make me sense so beautiful and intelligent and that I can take over the universe. I feel extremely proud having such avant-garde grandparents.
To my latest grandparents and especially my grandfather Fire
Katir Mohammed;
He was a great man. A writer, a judge, a warrior and a peace advocate. Thank you for your sacrifice for this country. Thank you for raising such conscientious men and women. The
To my uncle Said Bentaher and his family;
Said my brother and my friend. I love you beyond words can say. You have always being my confident, and I am never afraid to talk to you about anything and everything. Your words are wisdom, your hugs are sweetness and your generosity is everything. Aunty Maha I am
very happy you are part of our family. I love you and respect you a lot for the smart and gentle women you are. You make my bro so happy. Thank you.
As for Rim and Reda they are a JOY to be around. They are so smart and elegant they may restore my faith in children.
To my family in Spain
To my amazing friends and second family (with no order of
preference I swear, but women first)
Zineb El Hamdani
OMG where do I begin … Zineb you are one of my sisters, my best friends and my life companion. I can’t thank you enough for the things you have done for me. Since we were teenagers, it was the start of a great friendship that will last for eternity. You are the most
graceful and wise people I know. I am amazed how down to earth and logical you can be and at the same time you have a great sense of adventure and not afraid to get out your comfort zone. I thank you for all the moments you’ve hold my hand when times were rough. I thank you for the wonderful memories we made. I thank you for barring me at times when
I can’t even bare myself.
Basma Lahmer
One of the greatest friendships I made thank to IFMSA and later on thank to her light spirit and sweetness. Oh Basma..and to think I told you at the beginning I didn’t like you xD. I take that back a million times. We have grown to learn and understand each so much I can’t imagine experiencing or going through something without picking the phone and tell you everything. I love you so much. And I am forever grateful for your help and compassion.
Salma Naji
Salma (known also as Salmonella, Saji, Slims and others) Thank you a lot for stalking me in first year of med school, or else we wouldn’t have became such power couple. We have grown together and separately. We have experienced the good as well as the bad together. But whatever we do, whatever we say, whatever we go through, we always stand still and
fight. You are a beautiful human being; I wish you could see what I see in you.
Imane Melhaoui
I was never up for long-distance relationships in general until I came across this beauty. And I was hooked. My wifey, I love you above and beyond. You are the true meaning of unconditional love, because you always give and wish nothing in return. Thank you for listening to me, encouraging me, complimenting me, being kind and patient with me. You’ve helps me a lot and you do. Distance sucks, but it sucks less knowing that there is someone in
the other side of the country that will always have your back.
Maha Laouadi
Maha I thank you for being a great ear went I needed to venting. Thank you for the good times we had, the laughs, the memories and especially for your friendship. You are wonderful and I will always cherish the bond we have. We don’t talk every day, but when
Amine Hmaidouch
My longest relationship ever, 13 years now going 14! I love you so much for the person and friend you are. You have always been my confidant, my go-to person when I need encouraging words or a good laugh. Your sarcastic nature and your memes are unparalleled and a great source of help as well as the random sweet texts you send me from time to time.
I hope that WE never stop being. I can always count on you because you have never deceived me. So I will just say Thank you a billion times from the bottom of my heart.
Mehdi Farina
Funny, down to earth, wise sometimes yet others the contrary. But one thing that is constant is your kindness. The times you answered my calls in a heartbeat are countless, I can never thank you enough for that. You have a great and conscientious heart and it is one
the many things I like about you. I love you and may our friendship continue forever.
Saad Ait El Borj
You are an incredible friend. I always find you beside me when I need to. Thank you for sharing your vision of life with me because it is such an interesting one. Thank you for your advice and caring love even if you say that you don’t care but deep deep deep deep down you
do a little, and honestly that's all I need. P.S. Thank you for adopting Spiky because I am now an aunty to an amazing child.
Mehdi Ajji
You are so sweet and gentle. I always have a smile on my face when I say your name. Thank you for your kindness. Thank you for your time. I will always cherish our
memories together, and I hope our friendship continues. I love you a lot.
To my life partner Kamal Marzouki
I became a happier person with you. Thank you for all that you have done. For standing by me and encouraging me and compromising things for me. For doing all you can and beyond
so I can be comfortable and happy all the time. You spoiled me! I cannot imagine a day without you. You showed me it is possible to love and be loved unconditionally. Thank you
To my other friends and colleagues
My words of gratitude go to my friends who have always been a constant source of support when things would get a bit discouraging. May we continue this beautiful journey that is life together and I thank you for all the beautiful memories and the unforgettable moments.
Nora Ryadi, Yassine Gounni, Hala Saber, Abbas Guennoun, Mehdi Guedira, Mounia Benouachane, Rim Sadki, Mehdi Ilahiyane, Houda Bachri, Nouha Bennouna, Ilias Hmaidouch , Mohammed Reda Hassouni , Viktoria Petrova , Anastasio Garcia Garcia ,
Marouane Amzil, Omar Cherkaoui , Faouz Mansouri, Houria El Yazidi ...
To my Oujdi and Tunisian Friends
Amine Benyoussef , Amine El Hassani, Ossema Kallel, Ismail Chergui , Mehdi Samet, Khaoutar Sof , Amine Bensaid, And others
To my international and IFMSA friends
Mirona Predescu , Alex Oprita , Adeline Staicu , Chiara Premuda , Vero Moreno , Camelia Bigea , Robert Godeanu ,George Dub , Karim salah el Deene, Adrean Dulea , Giulia Beatrice, Utku Kuyusu , Iftitah Rahma , Larissa Peixoto , Andrea Podeanu , Alina Chirea ,
To my best Moroccan IFMSA delegation ever and best
MRT people
Rayane, Yassine, Baha, Meriem, Omar, Oumaima ,Zainab, Saad , Assaad , Ali chouchou , Basma, Marouane , Simo ,Mehdi and Maha.
To Pr. BELAYACHI Jihane
I would like to start by acknowledging the devoted help and guidance of my thesis advisor, Pr J. BELAYACHI. She was truly an inspiration through her patience and enthusiasm. Her insightful comments were a great source of constant motivation and
To Pr. ABOUQAL Redouane
I wish to thank my thesis president Pr. R. ABOUQAL, an honourable renowned professor whose expertise was essential to the completion of this work. His help and detailed explanations were necessary for taking this work to fruition. I will forever be
To Pr. MADANI Naoufel
I would like to thank Pr. N. MADANI for taking some time to discuss and enrich my work. Having him in my thesis committee is an honor and a pleasure and will be a great
To Pr. IRAQI Hind
I would like to thank Pr. H. IRAQI for accepting to be one of the members of my thesis committee. She graciously offered not only her time but also her goodwill, support and guidance to review this document; she is to be a source of valuable insight, remarks and
To Pr. DOGHMI Nawal
I would also like to thank Pr. N. DOGHMI for accepting to read and give input on my present work. Her advice during the writing of this work as well as expertise as a
A
WHO World Health Organization
HF Heart failure
ADCHF Acutely decompensated chronic heart failure
AHF Acute heart failure
EF Ejection fraction
HFpEF Heart failure with preserved ejection fraction
HFrEF Heart failure with reduced ejection fraction
AHF Acute heart failure
ESC European society of cardiology
ND No description
MIC Malnutrition, inflammation and cachexia
PN Parenteral nutrition
ATP Adenosine Triphosphate
FAO Fatty acid oxidation
PNI Prognostic Nutritional Index
NRI Nutritional Risk Index
CONUT Controlling Nutritional Status
MNA Mini Nutritional Assessment
TTR Serum transthyretin
BMI Body Mass Index
RAA Renin-angiotensin-aldosterone
REE Resting expending energy
E/é The ratio of transmitral flow velocity to mitral annulus motion velocity in early diastole
e.g. Exempli gratia
i.e Id est.
NOS Newcastle-Ottawa Assessment Scale
ORs Odd ratios
HRs Hazard ratios
COI Conflict of interest
RVSP Right ventricular systolic pressure
LVSD Left ventricular systolic dysfunction
PICO Population. Intervention. Comparison. Outcome(s)
NS No statement
VS Versus
ACM All-cause-mortality
NR Non reported
PUFA Polyunsaturated fatty acids
CRP ASPEN NRS GLIM TNF IL PRISMA-P C-Reactive protein
American society for parenteral and enteral nutrition Nutritional risk screening
Global leadership initiative in malnutrition Tumor necrosis factor
Interleukin
Preferred reporting items for systematic review and meta-analysis protocols
ILL
L
LUS
IST
STRA
T of
ATIO
ONS
List of figures
Figure 1 : The Global Leadership Initiative on Malnutrition diagnostic scheme
for screening, assessment, diagnosis and grading of malnutrition. ... 10
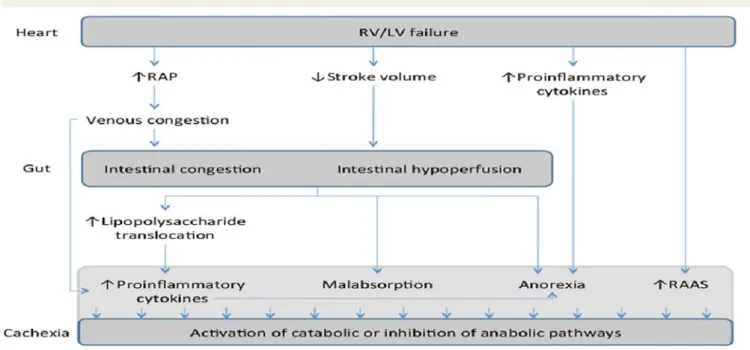
Figure 2 : Intestinal congestion and right ventricular dysfunction a link with
appetite loss, inflammation, and cachexia in heart failure ... 16
Figure 3 : Innate Immunity and the Failing Heart ... 18 Figure 4 : Malnutrition and Energy waist ... 20 Figure 5 : Cachexia and sarcopenia in heart failure. ... 23 Figure 6 : Malnutrition related to heart failure ... 24 Figure 7 : Obesity and survival in heart failure ... 26 Figure 8 : Body Composition and Heart Failure Prognosis ... 27 Figure 9 : Flow chart of study selection process ... 38 Figure 10 : Mortality rates in the review studies ... 50 Figure 11 : Forest plot for risk of ACM associated with risk of malnutrition in
patients with AHF ... 53
Figure 12 : Forest plot showing the nutritional screening tools in subgroups of
GNRI, PNI, CONUT and NRI ... 54
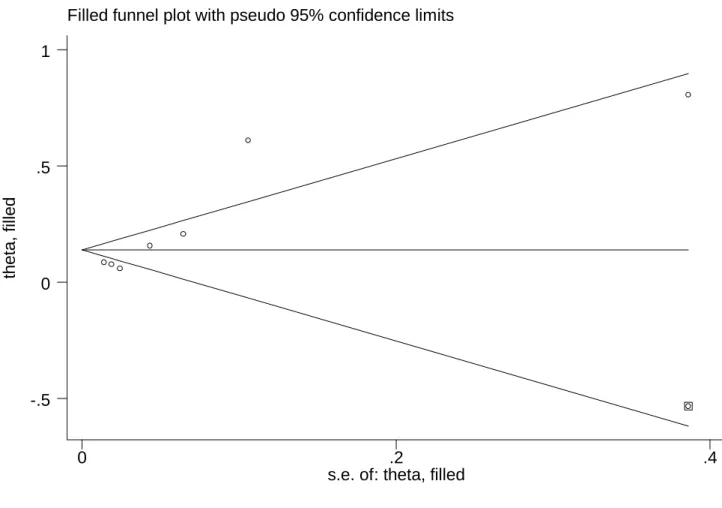
Figure 13 : Forest plot showing the mean follow-up duration ... 55 Figure 14 : Funnel plot showing publication bias ... 56 Figure 15 : Trim and fill figure. ... 57
List of table
Table 1 : Screening and assessment of malnutrition and cachexia. ... 9 Table 2 : Search strategy of the review ... 29 Table 3 : Newcastle-Ottawa quality assessment scale for cohort studies ... 33 Table 4 : study design of the review articles ... 40 Table 5 : Definition of AHF mentioned in the review studies ... 42 Table 6 : Nutrition screening instrument parameters used in review studies .... 44 Table 7 : Patients characteristics’ ... 46 Table 8 : Prevalence of malnutrition as assessed in studies (%) ... 48 Table 9 : ACM rates at follow-ups ... 49 Table 10 : Results of outcome ACM measurement ... 52 Table 11 : The Newcastle-Ottawa Scale used for quality assessment of the
twelve studies included in the systematic review. ... 65
I. INTRODUCTION ... 1
Acute heart failure related malnutrition ... 5
1. Phenotypic malnutrition criteria ... 6 2. Etiologic malnutrition criteria ... 7 3. Approach to malnutrition diagnosis, severity grading, and classification .. 7
Malnutrition in the acute heart failure ... 11
1. Definition of acute heart failure ... 12 2. Epidemiology of undernutrition and risk of undernutrition ... 13 3. Physiopathology of malnutrition in heart failure ... 14
3.1. Decreased Energy supply ... 14 3.2. Gastrointestinal and hepatic disorders ... 15 3.3. Cytokine production ... 17 3.4. Drug use ... 18 3.5. Electrolytes and micronutrients disorders’ ... 19 3.6. Increased nutritional requirements from increased resting energy
expenditure ... 20 3.7. Increased Energy demand: Hypercatabolism ... 20 3.8. Insulin resistance ... 21 3.9. Renal insufficiency ... 21
3.10. Cachexia and Sarcopenia ... 22 4. Physiopathology particularities of malnutrition in acute heart failure ... 25 5. The obesity paradox ... 26
Nutritional Status Screening particularly in AHF ... 28
II. METHODS AND MEASURES ... 29 1. Literature search ... 29 2. Selection of papers ... 30
2.1. Exclusion criteria ... 30 2.2. Inclusion criteria ... 31 3. Assessment of methodological quality ... 32 3.1. For the protocol ... 32 3.2. For the cohort studies ... 32 4. Data extraction ... 35 5. Data analysis ... 35 6. Protocol and registration ... 37 III. RESULTS ... 37
1. Search results ... 37 2. Characteristics of studies ... 39 3. Definition of AHF ... 41 4. Modalities of screening tools used in AHF patients ... 43
4.1. Instruments ... 43 4.2. Cut-off values ... 43 5. Quality assessment ... 45 6. Conflict of interest ... 46 7. Results of individual studies ... 46 7.1. Participants characteristics’ ... 46 7.2. Prevalence of malnutrition in patients with AHF ... 47 8. ACM Mortality rates ... 49 9. Results of out-come ACM associated with malnutrition in patients with AHF ... 50 10. Association of nutritional risk with ACM mortality... 52 10.1. Sources of heterogeneity ... 53 10.2. Publication Bias ... 55 IV. DISCUSSION ... 58 1. Summary of evidence ... 58 2. Limitations ... 61 CONCLUSION ... 62 APPENDIX ... 64 RESUMES ... 72 REFERENCES ... 76
1
I. INTRODUCTION
All countries worldwide are affected by one or more forms of malnutrition. To battle with malnutrition in all its forms is one of the biggest global health challenges. Women, elderly, infants, children, and adolescents are at particular risk of malnutrition (1).
Undernutrition is a state of energy, protein and/or micronutrient deficiency producing unwanted weight loss of more than 10% in 6 months as well as a measurable change in bodily functions (2).
Often perceived as a problem in developing countries, undernutrition is in reality also common among elderly, precarious or hospitalized populations. In hospitals, it affects up to 70% of the elderly and 60% of cancer patients. It is also very common in intensive care units (3).
Statistics show that:
1.9 billion adults are overweight or obese, while 462 million are underweight (1).
52 million young children aged five or less are wasted, 17 million are severely wasted and 155 million are stunted, while 41 million are overweight or obese (1).
Around 45% of deaths are linked to undernutrition. These mostly occur in low- and middle-income countries. At the same time, in these same countries, rates of childhood overweight and obesity are rising (1).
2 The social, developmental, economic, and medical impacts of the general hamper of malnutrition are to take seriously, for the benefit of individuals, their families, communities and also countries.
Numerous factors can be the cause of malnutrition, mostly the ones related to poor diet or severe and repeated infections, especially in underdeveloped countries. Inappropriate diet and illness are much associated with the general standard of living, the environmental conditions, and whether a population can meet its basic needs such as food, housing, and health care.
Thus, malnutrition is a health outcome as well as a risk factor for disease and worsened malnutrition, and it can expand the risk both of morbidity and mortality.
At the end of the 20th century and beginning of a new millennium, hospital malnutrition continues to be prevalent. Malnutrition has been related to:
Increased morbidity, mortality, length of hospital stay and costs (4–7). Malnourished patients stayed in the hospital for 16.7 days vs. 10.177 days
compared to well-nourished(8).
Hospital costs in malnourished patients were increased up to 308.9% (8). Undernutrition is a complex pathophysiological situation, resulting from a deficit in energy and/or protein intake more or less associated with metabolic disturbances secondary to the disease. This means that if the disease promotes and/or worsens undernutrition, undernutrition worsens the disease and limits the effectiveness of treatments. Undernutrition is a global public health issue since more than a billion human beings are affected. It is one of the four major causes
3 of death with an estimate of more than a billion and a half of annual deaths.
Undernutrition is also rampant endemic in hospitals in the most economically developed countries where patients pay a heavy price in terms of morbidity and mortality, while society sees the most additional hospital costs of undernutrition increase with the progress of medicine.
Any pathology can be accompanied by undernutrition, but the extreme ages of life are the most affected. The development of "quality procedures" must lead to the development of screening and treatment strategies for hospital undernutrition. The treatment of undernutrition in hospitalized patients involves improving the supply of food care (dietitians), the rational use of oral supplementation, enteral or even parenteral nutrition (9).
According to the World Health Organization (WHO), cardiovascular diseases are the leading cause of mortality worldwide, taking an estimated 17.9 million lives each year(10), with some variation in epidemiology due to the factors associated with lifestyle, behavioral risk factors, genetic and racial differences (11). In daily practice, the most frequent emergency consultation motif is the heart failure syndrome. Different cardiology societies determined numerous criteria for defining heart failure (HF).
The prevalence of undernutrition during heart failure varies between 10% and 68%, depending on the heart disease considered and the stage of the disease. Undernutrition is often linked to anorexia, eating difficulties in advanced forms due to the increase in postprandial oxygen consumption which can be a real stress test.
4 It is in these situations that splitting the feed can be helpful. Undernutrition is a prognostic factor correlated with survival in forms of chronic heart failure. It is not always easy to correct. Indeed, when the loss of lean mass is a physiological mechanism of adaptation to chronic hypoxia, any attempt at re-nutrition is generally a failure when it does not aggravate hypoxia (12).
However, precedently, no systematic review of mortality risk related to malnutrition in patients admitted with acute heart failure has been performed. We systematically reviewed the observational epidemiology literature to determine the all-cause mortality in undernourished patients with acute heart failure or at risk of malnutrition through a meta-analysis of observational studies.
Ac
cute hear
maln
rt fai
lnutri
ilure
rition
relat
n
ted
56 Decreased intake or assimilation of nutrients will result in classic malnutrition (e.g. undernutrition), but there is a growing understanding that disease-associated inflammatory and other mechanisms may also contribute to malnutrition (i.e. undernutrition).
No single existing approach has achieved boundless global acceptance, making it difficult to compare findings beyond regions across the world or even between hospitals within regions.
The malnutrition criteria for deliberation were identified from existing universally used approaches. Then they were graded by election among the Global Leadership Initiative on Malnutrition participants (13).
There was a vigorous approbation of three phenotypic criteria (weight loss, low body mass index, and reduced muscle mass) and two etiologic criteria (reduced food intake or assimilation, and inflammation or disease burden).
1. Phenotypic malnutrition criteria (13)
Weigh loss: more than 5% within the past 6 months or more than 10% beyond 6 months;
Low Body Mass Index (BMI): less than 20 Kg/m2 if the patient has 70 years old or younger or less than 22 Kg/m2 if the patient is aged more than 70 years old;
Reduced muscle mass: validated body composition measuring techniques.
7
2. Etiologic malnutrition criteria (13)
The etiological criteria are two:
Inflammation: from acute disease or injury, or chronic disease-related; Reduced food intake or assimilation: less than 50% of energy requires
more than a week or any reduction that exceeds two weeks, or any gastrointestinal condition that impacts absorption and/or food assimilation.
The requirement for the diagnosis of malnutrition speculated the existence of at least 1 phenotypic criterion and 1 etiologic criterion.
3. Approach to malnutrition diagnosis, severity grading, and classification
Nutritional screening and assessment to differentiate malnourished and non-malnourished patients are the first steps in successful nutritional management in all patients (14,15).
Anthropometric parameters (16), such as BMI, triceps skinfold measurement and mid-arm circumference, and biochemical parameters (17), such as albumin, prealbumin, and cholesterol, are traditional nutritional evaluation indexes and have long been used in isolation to evaluate nutritional status (18,19). However, the use of these indexes alone cannot provide comprehensive and accurate indications of nutritional status (17,19).
Therefore, the Academy of Nutrition and Dietetics (the Academy) and the American Society for Parenteral and Enteral Nutrition (ASPEN.) also recommend the use of two or more of the following multidimensional evaluation technologies for improved nutritional evaluations: inadequate energy intake,
8 weight loss, waste of muscle mass, loss of subcutaneous fat, localized or generalized fluid accumulation that may occasionally mask weight loss and diminished functional status as measured by handgrip strength(20).
Moreover, numerous nutritional screening tools composed of multiple objective nutritional parameters and subjective data from case histories have been developed to enable improved nutritional status evaluations (21).
Generally, multidimensional evaluation tools refer to nutritional assessment tools and nutritional screening tools (18). Nutrition assessment and screening constitute the first of four steps of the nutrition care process and are thus very important. Nutritional screening and nutritional assessment are terms that are often used interchangeably in the literature and in practice despite their differences (21).
The nutrition screening is described by ASPEN as ‘‘a process to identify
an individual who is malnourished or who is at risk for undernutrition to determine if a detailed nutrition assessment is indicated’’ (22) and incorporates many instruments: Nutritional Risk Screening (NRS) (23), the prognostic nutritional index (PNI) (13), the Nutritional Risk Index (NRI) (24) and the Geriatric Nutritional Risk Index (GNRI) (25).
The nutritional assessment has been defined by ASPEN as ‘‘a
comprehensive approach to diagnosing nutrition problems that uses a combination of the following: medical, nutrition and medication histories; physical examination; anthropometric measurements; and laboratory data’’ (26) and includes the Mini Nutritional Assessment (MNA) (21).
T screeni (18,20) diagno existin conseq particip GLIM There was ing to iden ). When t osis and se ng approa quently im pants who participan Table s a strong ntify ‘‘at-the ‘‘at-ri everity gra aches used mplemente o ranked t nts elected 1 : Screeni g consens -risk’’ stat sk’’ statu ading shou d in scre ed (Table the criteri d the follo
ing and ass
sus that t tus by the us is estab uld be con ening and 1). A re a identifie owing core sessment of the first use of an blished, th nducted. A d assessm ferendum ed by the e criteria ( f malnutrit step is m ny validate hen further A compreh ment of m was regu study. A 13).
ion and cac
malnutritio ed screeni r assessm hensive su malnutritio ulated by vast majo chexia. 9 on risk ing tool ment for urvey of on was GLIM ority of
Figu ure 1 : The scre Global Le eening, asse adership In essment, dia nitiative on agnosis and n Malnutrit d grading o tion diagno of malnutri ostic schem ition. 10 me for
Ma
Ac
alnut
ute h
tritio
heart
on in
t fail
n the
lure
1112
1. Definition of acute heart failure
Heart failure (HF), known as well as congestive heart failure (CHF) or congestive cardiac failure (CCF), is when the heart is unable to pump sufficiently to maintain blood flow to meet the body's needs (27,28).It is the inability of the heart to keep up with the demands on it and, specifically, failure of the heart to pump blood with normal efficiency.
Acute heart failure has two forms: according to the 2016 ESC HF guidelines that if a chronic stable HF patient deteriorates it was described as “decompensated”, meantime if it was the first admission it was expressed as “de novo”(29).
Newly arisen (“de novo”) acute heart failure:
Generally, de novo (literally 'of new') is Latin expression used in the English language to hint 'from the beginning', 'anew'. In the case of acute heart failure, it means a firstly occurred episode.
Acutely decompensated chronic heart failure (ADCHF) (29):
Acute decompensated heart failure is described as the rapid or graduate outbreak of the signs or symptoms of heart failure demanding unplanned office visits, emergency room visits, or hospitalization (30). Handless of the critical precipitant of the exacerbation, pulmonary and systemic congestion due to increased left- and right-heart filling pressures is a nearly universal finding in ADHF (31).
13 Another important factor that can be added for a better definition of the HF is the ejection fraction (EF) given its importance in the diagnosis and the surveillance of the heart condition:
Diastolic HF with normal EF: HF with preserved EF (HFpEF)
Patients may seem to have a normal heart to pump a normal portion of the blood that enters it. However, heart muscle thickening may cause the ventricle to hold an abnormally small volume of blood. Thus, even if the heart’s output may continue to emerge to be in the normal range, its limited resources are insufficient to meet the body’s requirements.
Systolic HF otherwise called: HF with reduced ejection fraction (HFrEF) Here the heart muscle is unable to contract adequately and consequently expels less oxygen-rich blood into the body. Patients with this form of the disease will have lower-than-normal left ventricular ejection fraction on an echocardiogram (32).
2. Epidemiology of undernutrition and risk of undernutrition (26)
There is a lack of epidemiological investigations of the prevalence of undernutrition in HF because a consensus regarding nutritional assessment tools has not been reached. The prevalence of undernutrition and the risk of undernutrition varied greatly among the 17 systematically retrieved studies from 16 to 90 %. We speculate that differences in the subpopulations of HF patients were the main cause of this discrepancy. Studies have demonstrated that the prevalence of undernutrition is higher in both the advanced HF and acute decompensated HF patient subpopulation, at approximately 75–90 %. The prevalence of undernutrition ranges from 16 to 62 % in stable heart patients
14 according to five studies. These findings explain why the incidence of undernutrition or the risk of undernutrition increases with disease severity (4). This speculation is also consistent with Sargento and Al. (33) and Narumi and Al. (34); these studies indicated that nutritional status as assessed using nutritional assessment and screening tools is also associated with the Nt-Pro BNP, the most important surrogate marker of disease severity in HF. Earlier nutrition screening and interventions are essential for preventing HF cachexia and reducing mortality (35,36). Other possible reasons for the differences in the prevalence of undernutrition include the acquisition of data using different nutritional assessment and screening tools and the relatively small sample size
3. Physiopathology of malnutrition in heart failure
Malnutrition is considered a high risk for cardiac failure, but the evidence is limited (37). It seems to be a mediator of disease progression and determines a poor prognosis especially in advanced stages (38). Malnutrition mechanisms in heart failure may result from the following mechanisms:
3.1. Decreased Energy supply
Reduced energy intake and negative energy balance have been associated with lower intake of all macronutrients, including total and saturated fat, protein, and carbohydrate intake (41–43). Anorexia is characterized as both an inadequate food intake and suppressed appetite, can be attributed to the underlying pathophysiology of their disease, defined by a chronic inflammatory state and fluid overload, which leads to nausea, loss of appetite and early satiety from gastrointestinal edema, and hepatic congestion (44,45).
15 The development of appetite suppression, early satiety, and insulin resistance is further exacerbated by neurohormonal etiologies of anorexia (46). Malnutrition in patients with HF is a consequence of anabolic and catabolic imbalance, favoring the catabolic state with impaired gastrointestinal absorption as well as reduced food intake, adding the factor of anorexia, and the psychological disorders.
3.2. Gastrointestinal and hepatic disorders
Moreover, gastrointestinal malabsorption due to gastrointestinal edema or congestion and the hypoperfusion of the bowel in patients with HF are associated with poor nutrition (47,48). Both hepatic congestion and gastric distention contribute to an early postprandial feeling of fullness, and they also could lead to intolerance of food intake.
The reasons for appetite loss are multifactorial, and the drugs frequently prescribed to patients with HF could affect appetite (49). Intestinal congestion and redistribution of blood flow away from the splanchnic circulation due to increased sympathetic activity may contribute to intestinal mucosal barrier dysfunction, which causes lipopolysaccharide translocation into the systemic circulation, and may worsen malnutrition in patients with acute heart failure (AHF) (50).
Figurre 2 : Intesttinal conges loss, inflam stion and r mmation, a right ventri and cachexi icular dysfu ia in heart f unction a li failure(50). ink with ap . 16 ppetite
17
3.3. Cytokine production (51)
Elevated levels of inflammatory mediators have been identified in patients with heart failure, including heart failure with reduced and preserved ejection fraction, as well as acute decompensated heart failure (52). The link between heart failure and inflammation was first recognized in 1990 by Levine and Al. (53) who reported elevated levels of tumor necrosis factor (TNF) in heart failure patients.
Both innate and adaptive immune responses are activated in the heart in response to tissue injury that results from pathogens or environmental injury (e.g. ischemia or hemodynamic overloading). Whereas the innate immune system provides a global, non-specific defense against pathogens and/or tissue injury, the adaptive immune system provides a highly specific response that is mediated by B and T cells.
The “cytokine hypothesis”(54)for heart failure postulates that heart failure progresses, at least in part, as a result of the deleterious effects exerted by endogenous cytokine cascades on the heart and the peripheral circulation. The literature suggests that TNF modulates myocardial function through an immediate pathway that is manifest within minutes and is mediated by activation of the neutral sphingomyelinase pathway.
Several reports have demonstrated enhanced expression and release of inflammatory cytokines such as tumor necrosis factor (TNF)α, interleukin (IL)-1, IL-6, IL-18, and cardiotrophin-(IL)-1, as well as several chemokines (e.g. monocyte chemoattractant peptide (MCP)-1/CCL2, IL-8/CXCL8 and macrophage inflammatory protein-1α/CCL3) in HF patients (55–59).
T to be e New Y ventric mediat traditio 3. D aldoste improv extrem Admin to acce The plasma elevated i York Hea cular eject tors have onal risk m F .4. Drug u Despite the erone (RA ved the o mely poor nistered m entuate the a levels o in direct p art Assoc tion fract been foun markers (6 Figure 3 : I use e introduc AA) sys outcomes, r, especia medications e loss of a f inflamm proportion ciation cla tion (LVE nd to give 61). nnate Imm ction over tem anta the quali ally in th s in the tr ppetite an matory cyt n to the d assificatio EF)) (56,5 e prognos munity and r the last agonists, ity of life he advanc reatment p nd thus con tokines an degradatio on) and c 57,60). M stic inform the Failing twenty y beta-bloc fe, the fun
ced stage protocol o ntribute to nd other ch n of func cardiac co Moreover, mation out g Heart (52 ears of re ckers and nctional c es of the of acute he o weight lo hemokine ctional cla onduct (i several o t of the ra 2). enin-angio d devices capacity r e disease( eart failur oss. 18 es seem ass (i.e. i.e. left f these ange of otensin-s have remains (62,63). re seem
19
3.5. Electrolytes and micronutrients disorders’
Another futile energy expending cycle involves the sodium, potassium transporter Na+ K+ ATPase, an enzyme complex that uses ATP to pump Na out of cells(64). The failing heart is an energy-compromised organ, characterized by “metabolic remodeling” (65).
In addition, ischemia and oxidative stress may further reduce energy expenditure, resulting in cardiomyocyte injury (66). A larger number of micronutrient deficiencies have been shown to be associated with significantly shorter event-free survival, therefore underlining the importance of micronutrient status and high-quality dietary intake.
Such information is particularly important within the context of an association between sodium restriction and decreased intake of other micronutrients, including calcium, phosphate, thiamine, and folate, in addition to reduced intake of energy and carbohydrates (67).
While deficiencies in HF patients have been described for micronutrients that are involved in carbohydrate and fatty acid metabolism, calcium homeostasis, renin production, and antioxidant properties, their effects on energy utilization, cardiac contractility, endothelial function, and reactive oxidative stress have not been fully described in patients with HF (44,45,68–72).
3. So propor energy renal i malnut 3. P catecho decrea In patient splanch inflamm one, an .6. Increas expendi ome pati rtion incre y expendit insufficien trition. .7. Increas atients wi olamines, sed anabo ncreased c ts throug hnic circ matory cy nd excessi Figure sed nutriti iture (40) ients with eases with ture (REE ncy, cance sed Energy ith HF ar includin olic hormo catecholam gh the de culation ytokine rel ive protein 4 : Malnut ional requ h HF hav h symptom E) (73). C er, and ch y demand re in a hy ng epinep ones, such mine leve evelopmen leading t lease and n loss on th trition and uirements f ve an in matic clas Common hronic pu : Hyperca ypercatab phrine, n as insulin els likely nt of in to increa can attribu the other h Energy wa from incre ncreased m s, contrib metabolic ulmonary d atabolism( olic state norepineph n-like grow contribut ntestinal i ased perm ute to mal hand (75). aist (44). eased resti metabolic uting to i c comorb disease al (72) with inc hrine, and wth factor te to mal ischemia meability labsorption ing energy c rate, an increased bidities inc lso contrib creased le d cortiso r (74). lnutrition with dec and inc n of lipids 20 y nd this resting cluding bute to vels of ol, and in HF creased creased s on the
21 Therefore, HF disease pathophysiology predisposes patients to a disadvantage in nutritional status, as patients with HF are experiencing malnutrition from an energy imbalance arising from increased energy requirements and decreased energy intake.
3.8. Insulin resistance
Doehner and Al. showed that insulin resistance correlated with higher leptin levels in non-cachectic patients with HF (76). Insulin is an essential hormone for utilizing glucose and facilitating anabolism, thus potentially contributing to muscle mass regulation.
Impaired glucose metabolism has been observed in 43 % of patients with HF, which contributes to further muscle wasting (9). The high rates of ATP production and turnover are critical in maintaining cardiac contractility to deliver blood and oxygen to the other organs. Under normal conditions, cardiac ATP is mainly derived from fatty acid (FA) oxidation (FAO), with glucose metabolism contributing less (77). However, under stress conditions, FAO may be reduced, which is concomitant with increased glucose utilization (78).
3.9. Renal insufficiency
Heart failure pathophysiology is characterized by systolic and diastolic abnormalities of the myocardium that result in reduced cardiac output (CO) and reduced renal perfusion. These trigger compensatory mechanisms, including left ventricular dilatation and activation of the sympathetic and renin-angiotensin-aldosterone systems (RAAS) which lead to a vicious cycle of systemic vasoconstriction, increased blood pressure and heart rate, and sodium and water retention despite existing volume overload.