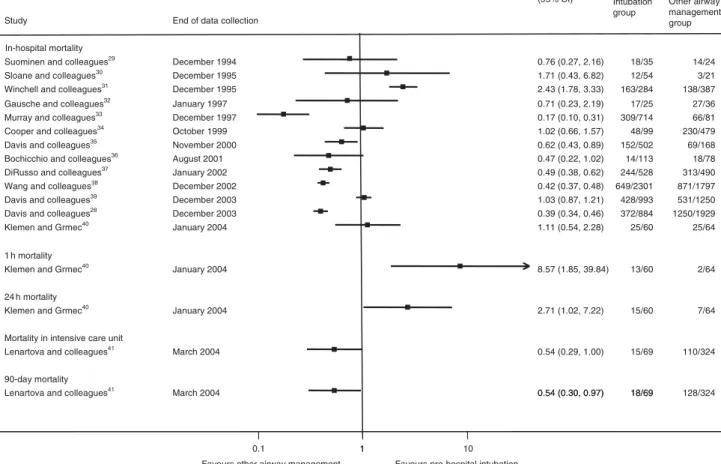
Pre-hospital tracheal intubation in patients with traumatic brain injury: systematic review of current evidence
16
0
0
Texte intégral
Figure
+7
Documents relatifs
