HAL Id: hal-02263665
https://hal-amu.archives-ouvertes.fr/hal-02263665
Submitted on 3 Apr 2020
HAL is a multi-disciplinary open access
archive for the deposit and dissemination of
sci-entific research documents, whether they are
pub-lished or not. The documents may come from
teaching and research institutions in France or
abroad, or from public or private research centers.
L’archive ouverte pluridisciplinaire HAL, est
destinée au dépôt et à la diffusion de documents
scientifiques de niveau recherche, publiés ou non,
émanant des établissements d’enseignement et de
recherche français ou étrangers, des laboratoires
publics ou privés.
Maxillary fungus balls due to Fusarium proliferatum
T. Radulesco, A. Varoquaux, S. Ranque, P. Dessi, J. Michel, C. Cassagne
To cite this version:
T. Radulesco, A. Varoquaux, S. Ranque, P. Dessi, J. Michel, et al.. Maxillary fungus balls due
to Fusarium proliferatum. Journal of Medical Mycology / Journal de Mycologie Médicale, Elsevier
Masson, 2019, 29 (1), pp.59-61. �10.1016/j.mycmed.2019.01.008�. �hal-02263665�
Case
report
Maxillary
fungus
balls
due
to
Fusarium
proliferatum
T.
Radulesco
a,b,*
,
A.
Varoquaux
c,
S.
Ranque
d,
P.
Dessi
a,
J.
Michel
a,b,
C.
Cassagne
da DepartmentofOto-Rhino-LaryngologyandHeadandNeckSurgery,LaConceptionUniversityHospital,Assistancepublique–hoˆpitauxdeMarseille, 13385Marseille cedex,France
b
CNRS,IUSTI,Aix-MarseilleUniversite´,13453Marseille,France
c
DepartmentofRadiology,LaConceptionUniversityHospital,Assistancepublique–hoˆpitauxdeMarseille,13385Marseillecedex,France
d SSA,IRD,IHU—Me´diterrane´eInfection,VITROME,Aix-MarseilleUniversite´,AP–HM,13005Marseille,France
1. Introduction
Fungusballparanasalsinusitis,definedasacompactmassof fungalhyphaeandcellulardebrisinasinusalcavity,isthemost commonformofnon-invasivefungalrhinosinusitis.Fungusballs aremostlyunilateralandaffectpreferentiallythemaxillarysinus, followedbythesphenoidsinusand,inveryrarecases,theethmoid andfrontalsinuses[1].Immunocompetentmiddle-agedorelderly womenaremostcommonlyaffectedbyfungusballs,thatseemto developmostlyinthesmallestsinus[2].
Anotherimportantriskfactorofdevelopingmaxillarysinusitis isthepresenceofendodonticmaterial,particularlycontainingzinc oxide, accidentally pushed into the sinus during endodontic treatment[3].Themostcommonspeciesoffungusrecoveredfrom fungus balls are A. fumigatus and, rarely, other species of Aspergillus, Penicillium, Chrysosporium and Scedosporium [4]. Fusariumspecies,sometimesrecoveredfromotherformsoffungal rhinosinusitis such as allergic fungal rhinosinusitis or acute invasivefungalrhinosinusitis,arepoorlyassociatedwithsinonasal
fungus ball. Toourknowledge, onlyone case studyreported a fungusballtypepan-sinusitisduetoF.proliferatum[5].Here,we describetwofurthercasesofafungusballduetoF.proliferatum and providethefirstdescriptionof thisfungalpathogenwitha fungusballofodontogenicorigin.
2. Casereport1(medicalhistory)
A52-year-oldwomanwasreferredtoourDepartmentof Oto-Rhino-LaryngologyandHeadandNeckSurgeryforleftmaxillary sinusitis fortuitously discovered on CT-scan performed for dysphagia. Her medical history was insignificant except for esophagitis and a 30-pack-year smoking history. She had no functionalimpairment:nopain,norhinorrhea,nonasalbleeding andnoanosmia.Laboratoryvalueswereallnormal.Nomucosalor sub-mucosalabnormalenhancementwasdepictedonCT-scanner. Incidentally, CT-scannerdemonstrated a dental filling migrated fromthemesialrootof27totheleftmaxillarysinuscavity(Fig.1). Soft tissue thickening within the maxillary sinus floor was observed. MRI, performed for soft thickening characterization, showeda14mmmaxillarysinusfloorlesionwithintermediate signal on T1wi and signal void on T2wi consistent with a fungusball.Endoscopicsurgerywasperformedontheleftmaxilla to remove all involved mucosa and maxillary sinus content. Keywords: Fungi Surgery Mycoses Chronicsinusitis Paranasalsinus Maxillarydisease ABSTRACT
Fungus ballis the mostcommon formof non-invasivefungal rhinosinusitis. Aspergillus fumigatus (between44.8%and75%)andAspergillusflavus(14%)arethetwomostcommonspeciesrecovered. However, recent advances in mycological laboratory methods have enhanced the detection and identificationoffungiwithinfungusballs.Fusariumspecies,sometimesrecoveredfromotherformsof fungalrhinosinusitissuchasallergicfungalrhinosinusitisoracuteinvasivefungalrhinosinusitis,are poorlyassociatedwithsinonasalfungusball.Here,wedescribetwofurthercasesofafungusballdueto Fusariumproliferatumandprovidethefirstdescriptionofthisfungalpathogenwithafungusballof odontogenicorigin.ThesecasereportsdemonstratethatuncommonfungalspeciessuchasFusariumspp. mightbeunderestimatedasagentsofsinusalcavityfungusball.Enhancedmycologicaldetectionand diagnostictechniquesmightgiverise,inthenearfuture,totheemergenceofneworrarefungalspecies associatedwiththisclinicalentity.
* Correspondingauthor.DepartmentofOto-Rhino-LaryngologyandHeadand NeckSurgery,LaConceptionUniversityHospital,Assistancepublique–hoˆpitauxde Marseille,147,boulevardBaille,13005Marseille,France.
Multiple biopsiedfragments were collected during surgery for histopathologicalexaminationandmicrobiologicalanalysis. 3. Casereport2(medicalhistory)
A58-year-oldwomanwasreferredtoourDepartmentforleft maxillary sinusitis discovered on CT-scanner performed for chronicrhinosinusitiswithcrusts.Shehasnosignificantmedical historyexceptacoronaryarterydisease(2stents),dyslipidemia andobesity.Shehadnootherfunctionalimpairmentthannasal obstruction. Standard laboratory values were all normal. CT-scannerfoundasinusfillingandMRIasignalvoidonT2wi.
Inbothcases,alltheinvolvedmucosaandthefungalmasses wereremovedsurgically(FunctionalEndoscopic SinusSurgery). The fungal disease was thus considered as eradicated and no antifungal treatment was initiated. Prophylactic treatment by amoxicillinplusclavulanicacidwasadministeredfor 7days to reducetheriskofinfectionfollowingsurgery.Oneyearlater,no recurrencewasdetected.
4. Microbiologicalwork-up
Inbothcases,histologicalexaminationofthesinusalmucosa followingPeriodic Acid Schiffand Hematoxylinand Eosinstain showedaninflammatorysinusalmucosainfiltratedbynumerous polynuclearneutrophils.Microscopicdirectexaminationfollowing alactophenolbluestain(Lactophenolbluesolution,Sigma-Aldrich, France) showedhyaline and septate hyphae with acute angles (Fig.2).Otherpiecesofthebiopsiedtissuewereinoculatedonto Sabourauddextrose agar plates supplemented withgentamicin andchloramphenicol(SGC)(Oxoid,Dardilly,France)andincubated at308Cupto10days.Theculturemediawereexamineddailyfor microbialgrowth.
For Case1,sixdaysafterinoculation,awhitecottonycolony wasobservedontheSGCmedium.Microscopicexaminationofthe colonyshowedhyaline,septatehyphaeandsickled-shapeconidia suggestingaFusariumspecies.Thecolonywasfurtheridentified bothbyMALDI-TOFmassspectrometryandDNAsequence-based identificationasdescribedrespectivelybyCassagneetal.[6]and Gautieretal.[7].ThecolonywasidentifiedasF.proliferatumboth by MALDI-TOF mass spectrometry identification (with the interpretationcriteriadescribedin[5]andDNAsequence-based identification[>98% identity]). Theobtained ITS sequence was blastedagainstGenBanknucleotidesequencesandmatchedwith
100%identitywiththeF.proliferatumsequenceKY425734.1.For Case2,abiopsiedsinusalfragmentincubatedat308Cgrewawhite cottony colony at day four after incubation. The colony was identified by MALDI-TOF mass spectrometry as F. proliferatum
[6].Inparallel,directDNAsequencingidentificationtargetingthe rRNAITS2region(primersequences,[GCATCGATGAAGAACGCA GC]and[TCCTCCGCT TATTGATATGC]) andthepartial beta-tubulingene(primersequences[GGTAACCAAATCGGTGCTGCT TTC]and[ACCCTCAGTGTAGTGACCCTTGGC])wasperformedin parallelonanotherspecimenofthesinusalcontent.Theobtained sequencesmatched99%and100%withtheF.proliferatumGenbank accessionnumbersKJ767073.1andKX421566,respectively.
5. Discussion
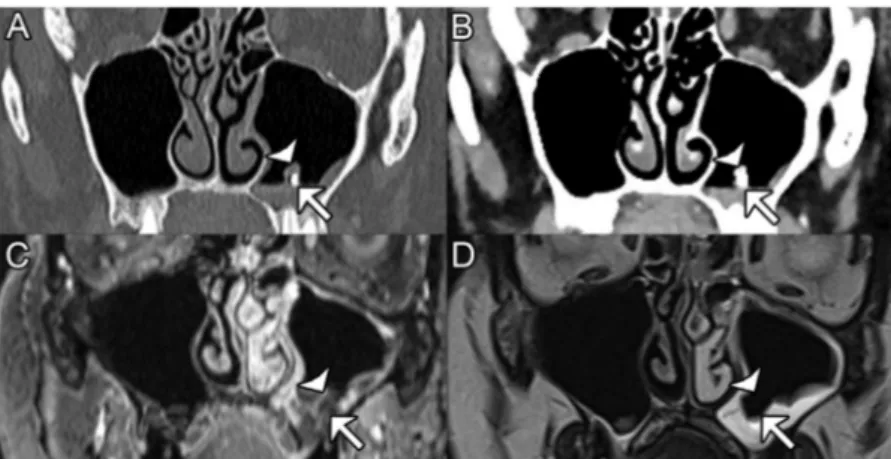
Fungalspeciescausingparanasalsinusitisfungusballsremain largelyunknownfortwomainreasons.First,fewfungusballsare sent for histopathological and/or mycological analysis after surgery.Second,fungus ballcultures areoftennegative,maybe onaccountofthepoorviabilityofthefungalcomponentwithina fungusball.Onlyabout23%to50%ofthefungusballsgrewon Fig.1.Justvisiblemaxillaryfungusball:coregisteredCT-scanner(A,B)andT1withgadolinum(C,axial3DVibegradientrecallafter2Dreslicinginthecoronalplane coregisteredwithT2),T2wi(D).Metaldentalfilling(arrow)migratedintothemaxillarysinuscavityisshownonCTusingbonewindowinginbonealgorithm.Very small-sizedfungusball(arrowhead)isseenasadenselesionabovethedentalamalgamonCTwithsofttissuealgorithmandwindowing(B),containingsecretionsinsignalvoidT2 (D) comparedtoT1(C).Notetheabsenceofmicro-concretionseenonCTwithbonealgorithm(A).
Fig.2.Lactophenolblue-stainedsmearofsinusdischargeshowingdichotomous branchedandseptatehyphae.
mycological culture media [8]. Although hyphae are often observed in surgical samples, direct microscopic examination cannotidentifythefungalspecies.A.fumigatus(between44.8%and 75%) and A. flavus (14%) are the two most common species recovered [8–10]. However, recent advances in mycological laboratorymethodshaveenhancedthedetectionand identifica-tionoffungiwithinfungusballs.Directsequencingfromsamples andidentificationbyMALDI-TOFmassspectrometryhavegreatly improved the mycological diagnosis over the last few decades
[11].BesidesAspergillusspp.,agrowingnumberofunusualspecies have been identified from sinuses fungus balls. For example, nucleotidesequencingisahelpfultoolfordiagnosing Schizophyl-lumcommune, anuncommonbasidiomycete,in fungal sinusitis
[11,12]. Other rare fungal genera involved in fungus ball are Alternaria,Bipolaris, Cochliobolus, Paecilomyces, Mucor, Scedospo-riumandPenicillium[10,13].WhileFusariumspeciesarefrequently isolatedfromtheenvironment,accordingtoKatkaretal.,theyare rarelyinvolvedinfungusball.[14].Fewcasesoffungusballdueto Fusariumsolaniarereportedintheliterature,andonlyonecaseof fungus ball due to F. proliferatum. In this paper, we described several very rare cases of F. proliferatum fungus ball maxillary sinusitis.Our casesdiffered fromthefirstone publishedbyits endodonticorigin[5].Presenceofendodonticmaterialinmaxillary sinushasbeenprovedtobeariskfactorforfungusball,evenifthe mechanism still remains unclear. Here, functional endoscopic sinussurgerywassufficienttocurethepatientsbyremovingthe fungalmaterialandinvolvedmucosa.Therewasnodifferencein clinical presentation compared to maxillary sinusitis due to Aspergillusspecies.Antifungaltreatmentisnotrequiredfor non-invasivefungalrhinosinusitis.Thesecasereportsdemonstratethat uncommon fungal species such as Fusarium spp. might be underestimatedasagentsofsinusalcavityfungusball.Enhanced mycologicaldetectionanddiagnostictechniquesmightgiverise,in thenear future,totheemergenceofneworrarefungalspecies associatedwiththisclinicalentity.
Ethics
Allproceduresperformedinstudiesinvolvinghuman partici-pants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964Helsinkideclarationanditslateramendmentsorcomparable ethical standards. Informed consent was obtained from all individualparticipantsincludedinthestudy.
Informedconsent:yes.
Ethicalresponsibilitiesofauthors
The manuscript has not been submitted to more than one journalforsimultaneousconsideration.
Themanuscripthasnotbeenpublishedpreviously(partlyorin full).
No data have been fabricated or manipulated (including images)tosupportourconclusions.
Nodata,text,ortheoriesbyothersarepresentedasiftheywere theauthor’sown(‘‘plagiarism’’).Properacknowledgementstoother worksmustbegiven(thisincludesmaterialthatiscloselycopied (near verbatim), summarized and/or paraphrased), quotation
marksareusedforverbatimcopyingofmaterial,andpermissions aresecuredformaterialthatiscopyrighted.
Consent to submit hasbeen received explicitly fromall co-authors,aswellasfromtheresponsibleauthorities– tacitlyor explicitly–attheinstitute/organizationwheretheworkhasbeen carriedout,beforetheworkissubmitted.
Authors whose names appear on the submission have contributedsufficientlytothescientificworkandthereforeshare collectiveresponsibilityandaccountabilityfortheresults. Funding
None.
Sourcesofsupportintheformofgrants:none. Disclosureofinterest
Theauthorsdeclarethattheyhavenocompetinginterest. Acknowledgement
None. References
[1]NicolaiP,LombardiD,TomenzoliD,VillaretAB,PiccioniM,MensiM,etal. Fungusballoftheparanasalsinuses:experiencein160patientstreatedwith endoscopicsurgery.Laryngoscope2009;119:2275–9.
[2]MichelJ,RadulescoT,ManciniJ,PaganelliA,VaroquauxA,AdalianP,etal. Maxillarysinusvolume:newphysiopathologicaldatainfungalballgenesis?A retrospectivestudy. ClinOtolaryngol2017;42:831–6.
[3]Mensi M,PiccioniM,MarsiliF, NicolaiP, SapelliPL. Latronicon.Risk of maxillaryfungusballinpatientswithendodontictreatmentonmaxillary teeth:acase-controlstudy.OralSurgOralMedOralPatholOralRadiolEndod 2007;103:433–6.
[4]Ferreiro J, Carlson B, Cody D. Paranasal sinus fungus balls. Head Neck 1997;19:481–6.
[5]HashemiS,ArdehaliM,RezaieS,ZibafarE,ShoarM,Rezaei-MatehkolaeiA, etal.Acaseoffungusball-typepansinusitisduetofusariumproliferatum. Mycopathologia2015;180:251–5.
[6]CassagneC,RanqueS,NormandAC,FourquetP,ThiebaultS,PlanardC,etal. Mouldroutineidentificationintheclinicallaboratorybymatrix-assistedlaser desorption ionizationtime-of-flight massspectrometry.PLoS One2011;6 [e28425].
[7]GautierM,RanqueS,NormandAC,BeckerP,PackeuA,CassagneC,etal. Matrix-assistedlaserdesorptionionizationtime-of-flightmassspectrometry: revolutionizingclinicallaboratorydiagnosisofmouldinfections.Clin Micro-biolInfect2014;20:1366–71.
[8]FergusonBJ.Fungusballsoftheparanasalsinuses.OtolaryngolClinNorthAm 2000;33:389–98.
[9]KlossekJ,SerranoE,PeloquinL,PercodaniJ,FontanelJ,PesseyJ.Functional endoscopicsinussurgeryand109mycetomasofparanasalsinuses. Laryngo-scope1997;107:112–7.
[10]MontoneK,LivolsiV,FeldmanM,PalmerJ,ChiuA,LanzaD,etal.Fungal rhinosinusitis: a retrospective microbiologic and pathologic review of 400 patients at a single university medical center. Int J Otolaryngol 2012;2012[684835].
[11]BaronO,CassaingS,PercodaniJ,BerryA,LinasMD,FabreR,etal.Nucleotide sequencingfordiagnosisofsinusalinfectionbySchizophyllumcommune,an uncommonpathogenicfungus.JClinMicrobiol2006;44:3042–3.
[12]MichelJ,MaubonD,VaroquauxDA,BoulzeC,NormandAC,RighiniCA,etal. Schizophyllumcommune:anemergentormisdiagnosedfungalpathogenin rhinology?MedMycol2016;54:301–9.
[13]GautierM,MichelJ,NormandAC,CassagneC,PiarrouxR,RanqueS. Cochlio-bolushawaiiensissinusitis,atropicaldisease?Acasereportandreviewofthe literature. Mycopathologia2015;180:117–21.
[14]KatkarVJ,TankhiwaleSS,KurhadeA.Fusariumsolonimycetoma.IndianJ Dermatol2011;56:315–7.