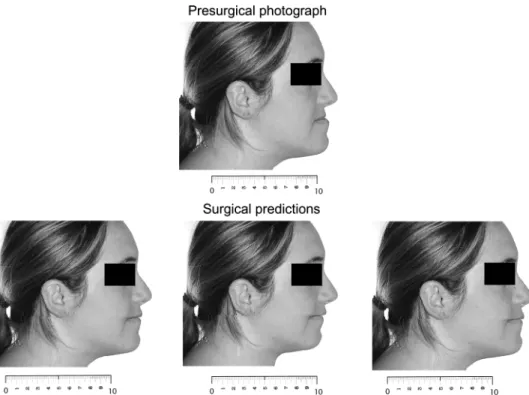
Professionals' and laypersons' appreciation of various options for Class III surgical correction
Texte intégral
Figure




Documents relatifs
The Swedish medical IR test collection, MedEval, from Språkbanken, Uni- versity of Gothenburg, will be used to find features specific for professional language
Appendix 20: A systematic review and meta-analysis including GRADE qualification of the risk of surgical site infections after prophylactic negative pressure wound therapy compared
The lateral fissure is subdivided in 3 segments (Figure 1); the middle one parallels the main axis of the temporal lobe and separates the opercular part of the inferior frontal
The SSP problem is divided into two steps; the first step is the advance scheduling, referred in the literature as the Surgical Case Assignments problem (SCAP)
Der Anteil des Wallis an ben Vurgunderkriegen 93 o H Dr.. Auf vorliegende Arbeit bin ich durch Herru Prof. %ib<;xt Büchi zu Freiburg i. liiip gefilhrt Worden. Seiu
L’archive ouverte pluridisciplinaire HAL, est destinée au dépôt et à la diffusion de documents scientifiques de niveau recherche, publiés ou non, émanant des
Coupez et coller le prochain object qui devrait apparaitre dans la suite1. `
Our technique was based on our experience in the massive weight loss patients, and permits to correct grade III gynecomastia and also major chest deformations following
