JCTM
ORIGINAL ARTICLES
First Clinical Judgment by Primary Care Physicians
Distinguishes Well Between Nonorganic and Organic
Causes of Abdominal or Chest Pain
Benedict Martina, MD, Bruno Bucheli, MD, Martin Stotz, MD,
Edouard Battegay, MD, Niklaus Gyr, MD
OBJECT/VE: To evaluate t h e a c c u r a c y of a preliminary diag- n o s i s based solely on p a t i e n t history and p h y s i c a l e x a m i n a - tion in m e d i c a l o u t p a t i e n t s w i t h abdominal or c h e s t pain. D E S I G N : Prospective observational study.
S E T T I N G : General m e d i c a l o u t p a t i e n t clinic in a u n i v e r s i t y t e a c h i n g hospitai.
PART/C/PANTS: One h u n d r e d n i n e t y n e w , c o n s e c u t i v e pa- t i e n t s w i t h a m e a n age of 4 4 years (SD = 14 years, range 3 0 - 5 8 years) w i t h a m a i n c o m p l a i n t of abdominal or c h e s t pain. M E A S U R E M E N T S A N D M A I N R E S U L T S : T h e preliminary diag- nosis, e s t a b l i s h e d on t h e basis of p a t i e n t h i s t o r y and p h y s i c a l examination, was compared w i t h a final diagnosis, obtained af- ter workup at completion of the chart. A nonorganic cause w a s established in 6 6 (59%) of 112 p a t i e n t s w i t h abdominal pain and in 6 5 (83%) of 78 w i t h c h e s t pain. The preliminary diagno- sis of "nonorganic" versus "organic" causes was correct in 79% of p a t i e n t s w i t h abdominal pain and in 88% of p a t i e n t s w i t h c h e s t pain. An "undoubted" preliminary diagnosis pre- dicted a correct a s s e s s m e n t in all p a t i e n t s w i t h abdominal pain and in all b u t one p a t i e n t w i t h c h e s t pain. Overail, o n l y 4 p a t i e n t s (3%) were initially incorrectly diagnosed as having a nonorganic cause of pain rather than an organic cause. In ad- dition, final nonorganic diagnosis (n = 131) was compared w i t h long-term follow-up b y obtaining information from pa- t i e n t s and, i f n e c e s s a r y , from treating p h y s i c i a n s . Follow-up information, obtained for 71% of t h e s e p a t i e n t s after a m e a n of 29 m o n t h s (range 1 8 - 5 6 m o n t h s ) i d e n t i f i e d three other pa- t i e n t s t h a t h a d b e e n m i s d i a g n o s e d as having a b d o m i n a i pain of nonorganic causes. Compared w i t h foUow-up, t h e diagnos- tic a c c u r a c y for nonorganic abdominal and c h e s t pain at chart c o m p l e t i o n w a s 93% and 98%, respectively.
C O N C L U S I O N S : A preliminary diagnosis of nonorganic versus organic a b d o m i n a l or c h e s t pain b a s e d on p a t i e n t h i s t o r y and p h y s i c a i e x a m i n a t i o n proved remarkably reliable. A c c u r a c y w a s a l m o s t c o m p l e t e in p a t i e n t s w i t h an "undoubted" prelim-
R e c e i v e d f r o m the Medical O u t p a t i e n t Clinic. D e p a r t m e n t o f In- ternal Medicine. University Hospital. Basel. S w i t z e r l a n d .
D r B a t t e g a y w a s a S C O R E f e l l o w o f the S w i s s National S c 5 ence F o u n d a t i o n (grant 3 2 3 t ,948.91).
A d d r e s s correspondence a n d reprint r e q u e s t s to Dr. Martincc Medical O u t p a t i e n t Clinic. University Hospital. CH-4031 Basel. S w i t z e r l a n d .
inary diagnosis, s u g g e s t i n g that w a t c h f u l w a i t i n g can be r e c o m m e n d e d in such cases.
K E Y W O R D S : abdominal pain; c h e s t pain; outpatients; nonor- ganic diagnosis; p a t i e n t history.
J GEN INTERN MED 1 9 9 7 ; 1 2 : 4 5 9 - 4 6 5 .
A
b d o m i n a l a n d c h e s t p a i n a r e a m o n g t h e m o s t fre q u e n t m a i n c o m p l a i n t s o f p a t i e n t s i n a m b u l a t o r y c a r e . 1,~ A s u b s t a n t i a l p e r c e n t a g e of t h e s e c o m p l a i n t s d o n o t h a v e r e a d i l y d i s c e r n i b l e o r g a n i c c a u s e s . N o n o r g a n i c d i a g n o s e s a r e m a d e i n u p to 6 0 % of p a t i e n t s i n p r i m a r y c a r e t h a t p r e s e n t w i t h a b d o m i n a l p a i n . 3 m i d i n a p p r o x i - m a t e l y 8 0 % of p a t i e n t s w i t h c h e s t p a i n . * A n e x t e n s i v e w o r k u p i n p a t i e n t s w i t h a b d o m i n a l o r c h e s t p a i n s u s p e c t e d of h a v i n g n o n o r g a n i c c a u s e s m a y i d e n t i f y o n l y a few p a t i e n t s w i t h o r g a n i c c a u s e s a n d m a y t h e r e f o r e h a v e a v e r y low d i a g n o s t i c yield. ->~ T h i s s u g g e s t s t h a t a d d i t i o n a l a n d s o m e t i m e s c o s t l y i n v e s t i g a t i o n s m i g h t b e u n - n e c e s s a r y . 1,5,,_~-13 T h e r e a r e a few s t u d i e s o n t h e d i a g n o s t i c a c c u r a c y o f p h y s i c i a n s " i n i t i a l a s s e s s m e n t s of n o n o r g m f i c v e r s u s or- g a n i c d i a g n o s e s i n p a t i e n t s w i t h a b d o m i n a l o r c h e s t p a i n i n p r i m a r y c a r e . 1,3,13 1~ H o w e v e r , m o s t of t h e s e s t u d i e s a r e n o t p r o s p e c t i v e , a n d n o n e a r e w i t h p a t i e n t s i n g e n e r a l m e d i c a l c l i n i c s t h a t i n c l u d e a l o n g t e r m follow u p . F u r t h e r m o r e , it is n o t e n t i r e l y c l e a r h o w d i a g n o s t i c a c c u r a c y v a r i e s w i t h t h e d e g r e e of c e r t a i n t y t h a t t h e p r i m a r y c a r e p h y s i c i a n a t t a c h e s to t h e i n i t i a l d i a g n o s i s . C o n s e q u e n t l y , p r i m a r y c a r e p h y s i c i a n s a r e o f t e n m i r e d i n d o u b t a b o u t w h e t h e r to r e l y o n t h e i r i n i t i a l a n d p r e l i m i n a r y d i a g n o s i s o f a n o n o r g a n i c c a u s e o f p a i n o r w h e t h e r to i n i t i a t e m o r e e x t e n s i v e t e s t i n g . T h e a i m o f t h i s p r o s p e c t i v e s t u d y w a s to a p p r a i s e t h e q u a l i t y of t h e p h y s i c i a n ' s i n i t i a l d i a g n o s t i c a s s e s s m e n t b a s e d o n p a t i e n t h i s t o r y a n d p h y s i c a l e x a m i n a t i o n for p a - t i e n t s p r e s e n t i n g i n g e n e r a l m e d i c a l o u t p a t i e n t c l i n i c s w i t h a b d o m i n a l o r c h e s t p a i n . Two c o m p a r i s o n s w e r e p e r f o r m e d . I n i t i a l d i a g n o s e s c h a r a c t e r i z e d a s " u n d o u b t e d " o r " p r o b a b l e " w e r e c o m p a r e d w i t h (11 t h e f i n a l d i a g n o s i s e s - t a b l i s h e d a f t e r w o r k u p a n d c o m p l e t i o n of t h e c h a r t , a n d (21 l o n g - t e r m f o l l o w - u p r e s u l t s . 4594,60 Marttrta et al.. First D i n g n o s i s in A b d o m i n a l or C h e s t Patrt JGIM
METHODS
Setting and Medical Staff
The Medical Outpatient Clinic is a division of the De- p a r t m e n t of Internal Medicine of the University Hospital Basel. This teaching hospital provides prinmpj, secondary, a n d tertiary care for a region with approximately 200.000 inhabitants, E a c h year a b o u t 20.000 general internal medi- cal consultations for a p p r o ~ m a t e l y 5,000 new patients are provided by the Medical O u t p a t i e n t Clinic. which is open to the public without referral. Approximately 80o/0 of the cases are primary care walk in patients: 20% of the patients are referred to the clinic by physicians of other departments, by general practitioners, or by specialists in town,
The m e d i c a l staff c o n s i s t s of 14 r e s i d e n t s in i n t e r n a l medicine, most of w h o m have undergone more thin1 4 y e a r s of postgraduate clinical training, mid three supervising at- tending physicians. A recent evaluation at our clinic set the duration of the first consultation at 35 m i n u t e s (range 2 0 - 75 minutes), This consultation usually consists of taking a careful patient history and a general physical examination.
Patients
All 1.032 n e w a n d consecutive general internal medi- cine o u t p a t i e n t s were prospectively evaluated a n d screened for the s t u d y during the 3 - m o n t h inclusion period from April through J u n e 1992, O u t p a t i e n t s who were seen in subspecialty clinics were not evaluated for inclusion into the study, Of 1.032 patients. 190 fulfilled inclusion crite- ria: i.e.. they h a d a b d o m i n a l or chest pain a s their m a i n complaint or symptom. These 190 patients were included in the p r e s e n t study,
Preliminary Diagnosis (Initial Assessment)
For all patients, r o u t i n e p a t i e n t history a n d physical e x a m i n a t i o n were performed by one of 14 r e s i d e n t s ac- cording to s t a n d a r d protocol. W h e n necessary, interpret- ers helped to obtain the history from p a t i e n t s s p e a k i n g foreign languages. Patients were s u b s e q u e n t l y p r e s e n t e d to a n a t t e n d i n g physician (A) who c h e c k e d directly with p a t i e n t s w h e n n e c e s s a r y to c o n f i r m e l e m e n t s of the his tory or physical e x a m i n a t i o n . A t t e n d i n g physician A a n d resident together reached a preliminary diagnosis, The pre- liminary diagnosis w a s i m m e d i a t e l y r e c o r d e d onto a s t a n dardized f o r m mid w a s rated as " u n d o u b t e d " or "proba- ble," An " u n d o u b t e d " p r e l i m i n a r y diagnosis w a s b a s e d on c h a r a c t e r i s t i c a n d specific findings allowing a d i a g n o s i s with a very high level of confidence by the involved physi- cians. A p r e l i m i n a r y d i a g n o s i s b a s e d on v a g u e or n o n s p e cific findings or a mere s u s p i c i o n w a s called "probable."
Workup
F u r t h e r w o r k u p i n c l u d e d routine laboratory testing a n d all m e a s u r e s d e e m e d n e c e s s a r y to r e a c h a d i a g n o s i s
t h a t might benefit the patient. Results of the individual diagnostic w o r k u p a n d i m m e d i a t e follow up visits over a m e a n d u r a t i o n of 2 w e e k s were recorded. T h e m o s t fre- q u e n t l y p e r f o r m e d i n v e s t i g a t i o n s in p a t i e n t s with ab- d o m i n a l pain were stool c u l t u r e for p a r a s i t e s or bacteria, a b d o m i n a l u l t r a s o u n d , g a s t r o d u o d e n a l endoscopy, a n d colonic endoscopy, The m o s t frequently performed inves- tigations in p a t i e n t s with c h e s t p a i n were c h e s t radiogra p h y a n d treadmill ergometry, In addition to treadmill er- gometry, m y o c a r d i a l p e r f u s i o n s c i n t i g r a p h y w a s done p a r t i c u l a r l y in p a t i e n t s with a n g i n a like c h e s t pain or c a r d i o v a s c u l a r risk factors,
Based on the diagnosis, reasons for abdominal or c h e s t p a i n were classified a s being of n o n o r g a n i c v e r s u s organic c a u s e s , Nonorganic c a u s e s of a b d o m i n a l p a i n were u n - specific pain s y m p t o m s s u c h as n o n u l e e r d y s p e p s i a a n d irritable bowel syndrome. Organic c a u s e s of abdominal pain were gastritis, peptic ulcer, parasitoses, enteritis, motility disorders due to alcohol consumption, cholelithiasis, chole cystitis, pancreatitis, a n d diverticulitis. Nonorganic c a u s e s of c h e s t pain were unspecific c h e s t pain s y m p t o m s a n d anxiety disorders. Organic c a u s e s of c h e s t pain were cor o n a r y h e a r t disease of a n y stage, pleuritis, t r a c h e o b r o n chitis, e s o p h a g e a l refltzx, c h e s t wall t r a u m a , a n d t u m o r s ,
"Gold Standard" Diagnosis
A final d i a g n o s i s w a s e s t a b l i s h e d by the r e s i d e n t a n d a t t e n d i n g physician A w h e n p a t i e n t s were discharged from the care of the Medical O u t p a t i e n t Clinic. i,e.. after test re- suits were entered into the chart mid a diagnosis was made, S u b s e q u e n t l y , all d i a g n o s e s were analyzed t o g e t h e r by at t e n d i n g p h y s i c i a n B a n d the resident. A s e c o n d diagnosis w a s reached, however, b e c a u s e attending physician B was n o t blinded to the s t u d y a i m s or the preliminary diagnosis: subsequently, a n o t h e r independent attending physiciml (C). who w a s blinded to the a i m s of the s t u d y a n d the prelimi n a r y diagnosis, reviewed all c h a r t s a n d m a d e the final di agnosis. The second a n d third "final" exact diagnoses were c o m p a r e d u s i n g the Kappa test. 1~' Thereafter. final diag- n o s e s were r e e v a l u a t e d a n d classified as being either n o n organic or organic by c o n s e n s u s b e t w e e n a t t e n d i n g physi- cimls B mid C. T h i s final c o n s e n s u s decision served as the gold s t a n d a r d to a s s e s s sensitivity, specificity, a c c u racy. a n d the likelihood ratio of the p r e l i m i n a r y diagnosis.
Follow-up of Patients with Nonorganic Causes of
Pain at Final Diagnosis
P a t i e n t s with n o n o r g a n i e a b d o m i n a l or c h e s t p a i n were c o n t a c t e d after a m e a n of 29 m o n t h s (range 18-56 months) after t h e i r first c o n s u l t a t i o n to verify the diagno- sis. Telephone interviews or, if necessary, a m b u l a t o r y c h e c k u p e x a m i n a t i o n s at o u r i n s t i t u t i o n were executed, To r e a c h as m a n y p a t i e n t s as possible, t e l e p h o n e calls were repeated. W h e n needed, specially trained i n t e r p r e t ers helped to r e c r u i t as m a n y p a t i e n t s a s possible for fol-
JGIM Volume 12. A u g u s t 1997 461
low-up. T h e p a t i e n t s w e r e a s k e d a b o u t n e w c o m p l a i n t s . c h a n g e of c o m p l a i n t s , f u r t h e r i n v e s t i g a t i o n s , i n t e r v e n i n g t r e a t m e n t s , a n d h o s p i t a l i z a t i o n s d u r i n g t h e f o l l o w - u p ob- s e r v a t i o n period, In all c a s e s w i t h s u s p e c t e d n e w diag- n o s e s , t h e r e s p o n s i b l e g e n e r a l p r a c t i t i o n e r w a s c o n t a c t e d to c o n f i r m or r e j e c t a l t e r n a t i v e d i a g n o s e s .
RESU LTS
Patients
O f 1,032 c o n s e c u t i v e n e w p a t i e n t s in t h e g e n e r a l Med- ical O u t p a t i e n t Clinic s c r e e n e d for t h e study, 190 fulfilled t h e i n c l u s i o n criteria: i,e,. t h e y h a d e i t h e r a b d o m i n a l p a i n (n 112) o r c h e s t p a i n (n 78) a s t h e i r m a i n c o m p l a i n t . T h e m e a n age w a s 4 4 y e a r s (SD = 14): 101 p a t i e n t s w e r e male. a n d 89 w e r e f e m a l e .
Definition of the Gold Standard
I n t e r o b s e r v e r a g r e e m e n t b e t w e e n a t t e n d i n g p h y s i e i a n s B a n d C on t h e final d i a g n o s i s a s well a s s e p a r a t i o n into n o n o r g a n i c o r o r g a n i c w a s e x c e l l e n t , w i t h a K = 0 . 9 5 in b o t h i n s t a n c e s . S u b s e q u e n t l y , all 190 p a t i e n t s w e r e c l a s s i f i e d b y c o n s e n s u s by t h e two a t t e n d i n g p h y s i c i a n s B a n d C a s h a v i n g a n o n o r g a n i c (n = 131) o r o r g a n i c (n = 59) final d i a g n o s i s .
Accuracy of Preliminary Diagnoses Based on
History and Physical Examination Alone
We i n v e s t i g a t e d w h e t h e r a p r e l i m i n a r y d i a g n o s i s of n o n o r g m l i c v e r s u s o r g a n i c c a u s e of p a i n w a s reliable, i,e,. w h e t h e r it c o m p a r e d f a v o r a b l y w i t h t h e d i a g n o s i s w h e n t h e p a t i e n t ' s c a s e w a s c o n s i d e r e d c l o s e d (see t h e gold s t a n d a r d above). A b d o m i n a l Pain, O f t h e 112 p a t i e n t s w i t h a b d o m i n a l p a i n a s t h e i r m a i n c o m p l a i n t , 4 7 (41%) h a d u p p e r a b d o m - i n a l pain, 3 0 (27%) h a d l o w e r a b d o m i n a l pain, a n d 35 (31%) h a d diffuse n o n l o c a l i z e d a b d o m i n a l pain. T h e pre- l i m i n a r y d i a g n o s i s w a s n o n o r g m l i c for 51 p a t i e n t s m i d or- ganic for 61 p a t i e n t s . After t h e final diagnosis, a n organic c a u s e w a s f o u n d in 4 6 (41%) of 112 p a t i e n t s {Table 1A), G a s t r i t i s (n 9). peptic u l c e r d i s e a s e (n 6). a n d a m e b i a - sis (n = 4) w e r e t h e m o s t f r e q u e n t o r g a n i c findings. SLxty six (59%) of 112 p a t i e n t s w e r e c o n s i d e r e d to h a v e a n o n o r - gmlic c a u s e of t h e i r p a i n (Table 1A).
T h e a c t u a l p r e l i m i n a r y d i a g n o s i s c o m p a r e d w i t h t h e a c t u a l final d i a g n o s i s w a s n o t c o r r e c t in 31 (28%) of 112 p a t i e n t s . As m a n y a s 19 of t h e s e 31 p a t i e n t s w e r e ulti- m a t e l y d i a g n o s e d w i t h a n o n o r g a n i c c a u s e of t h e i r pain: i.e., m o s t e r r o n e o u s J u d g m e n t s o c c u r r e d in p a t i e n t s t h a t w e r e initially d i a g n o s e d a s h a v i n g a p a i n of o r g a n i c origin a n d w e r e u l t i m a t e l y c l a s s i f i e d a s h a v i n g a p a i n of n o n o r gmlic origin, In 8 o t h e r p a t i e n t s a n o r g a n i c c a u s e o t h e r thin1 t h e p r e v i o u s l y s u s p e c t e d o n e w a s d i s c o v e r e d , e.g,. a p e p t i c u l c e r i n s t e a d of c h o l e l i t h i a s i s . O n l y 4 p a t i e n t s h a d
Table IA. Preliminary Diagnosis of Nonorganic Versus
Organic Abdominal Pain Compared with Final Diagnosis
Final Diagnosis
Preliminary Diagnosis
Nonorganic
Organic
Total
Nonorganic 47 4 51
Organic 19 42 * 61
T o t a l 6 6 4 6 1 1 2
*Eight patients hozl organ& ~ causes o f pain. different from t}re orue originalZy suspect~l,
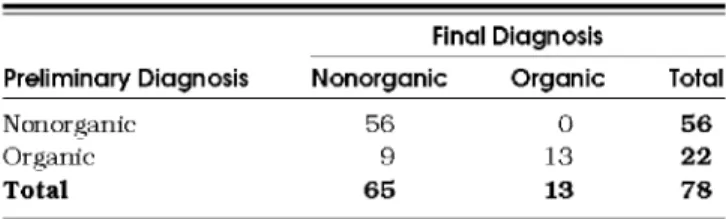
Table IB. Preliminary Diagnosis of Nonorganic Versus
Organic Chest Pain Compared with Final Dignosis
Final Diagnosis
Preliminary Diagnosis
Nonorganic
Organic
Total
Nonor~anic 56 0 5 6
Organic 9 13 2 2
T o t a l 6 5 1 3 7 8
a n o r g a n i c final d i a g n o s i s w h e n a p a i n of n o n o r g a n i c ori- gin h a d o r i g i n a l l y b e e n s u p p o s e d (one u r i n a r y infection, o n e a p p e n d i c i t i s , o n e p e p t i c ulcer, a n d o n e e n t e r i c a m e b i - asis), In 2 o f t h e p a t i e n t s w i t h a w r o n g p r e l i m i n a r y n o n o r - g a n i c d i a g n o s i s , t h e c o r r e c t d i a g n o s i s w a s m a d e w i t h i n a n h o u r a f t e r t h e p r e l i m i n a r y d i a g n o s i s o n t h e b a s i s of r o u - t i n e l a b o r a t o r y t e s t i n g ( d i a g n o s i s of a c u t e a p p e n d i c i t i s af- t e r l e u k o c y t e c o u n t a n d a b d o m i n a l u l t r a s o u n d , u r i n a r y i n f e c t i o n a f t e r urinalysis). In t h e r e m a i n i n g 2 p a t i e n t s , a c o r r e c t d i a g n o s i s w a s m a d e w i t h i n 2 d a y s : u p p e r e n d o s - c o p y led to t h e d i a g n o s i s of n o n b l e e d i n g p e p t i c ulcer, a n d p o s i t i v e stool t e s t s to t h e d i a g n o s i s of a m e b i a s i s . All 31 p r e l i m i n a r y d i a g n o s e s t h a t t u r n e d o u t to b e w r o n g h a d b e e n c h a r a c t e r i z e d a s "probable" b y t h e t r e a t i n g p h y s i c i a n s . In o t h e r w o r d s , t h e c o n f i d e n c e of t h e t r e a t i n g p h y s i c i m l s in t h e reliability of t h e i r d i a g n o s i s w a s low. Con- s e q u e n t l y , f u r t h e r w o r k u p w a s solicited t h a t r e s u l t e d in the final, c o r r e c t d i a g n o s i s in all of t h e s e c a s e s , In 4 0 (38%) of 112 c a s e s t h e p r e l i m i n a r y d i a g n o s i s h a d b e e n r a t e d a s " u n - d o u b t e d . " I n t h e s e c a s e s t h e d i a g n o s i s w a s a l w a y s c o r r e c t w h e n c o m p a r e d w i t h t h e final d i a g n o s i s (Tables 2 m i d 3). Hence, 81 (72%) of all 112 p a t i e n t s w i t h a b d o m i n a l p a i n h a d a n e x a c t final d i a g n o s i s c o r r e c t l y a s s e s s e d o n t h e b a s i s of h i s t o r y m i d p h y s i c a l e x a m i n a t i o n a l o n e (Table 3). T h e cor- r e s p o n d i n g sensitivity, specificity, a n d a c c u r a c y a r e excel l e n t for a n " u n d o u b t e d " p r e l i m i n a r y d i a g n o s i s a n d i n t e r m e d i a t e for a " p r o b a b l e " p r e l i m i n a r y d i a g n o s i s (Table 2), C h e s t Pain. O f 78 p a t i e n t s c o m p l a i n i n g m a i n l y of c h e s t pain, 65 (83%) h a d u n s p e c i f i c c o m p l a i n t s o f m u s e u l o s k e l - eta1 o r i g i n o r o t h e r s y m p t o m s t h a t w e r e c l a s s i f i e d a s n o n - o r g a n i c in final d i a g n o s i s (Table 1t3). In o n e t h i r d of t h e s e p a t i e n t s f u r t h e r i n v e s t i g a t i o n s s u c h a s t r e a d m i l l e r g o m e - t r y o r c h e s t r a d i o g y a p h y w e r e u s e d to e x c l u d e p o t e n t i a l o r g a n i c c a u s e s of c h e s t pain. O n l y 13 p a t i e n t s w i t h c h e s t p a i n (17~ r e c e i v e d a final d i a g n o s i s of o r g a n i c d i s e a s e
462 Marttna et ol.. First Diagnosis in Abdorntn01 or Chest Pare JGIM
Table 2. Quality of the Preliminary Diagnosis Preliminary Diagnosis of
Abdominal Pain
Preliminary Diagnosis of Chest Pain
Undoubted Probable Undoubted Probable
Measure (n = 40) (n = 72) (n = 56) (n = 22)
Sensitivity, % i00 57 98 69
Specificity, % 100 86 100 100
Accuracy, % 100 68 98 64
Likelihood ratio (95% CI) ':~ 3.97 (1.55,10.21) . . . .
(Table 1B): 4 p a t i e n t s (5%) h a d s y m p t o m a t i c c o r o n a r y h e a r t disease, a n d 9 (12%) h a d a n o t h e r organic final di- agnosis, m o s t frequently pleuritis (n = S). t r a c h e o b r o n c h i tis (n 2). or e s o p h a g e a l reflux (n 2).
Of the 78 patients. 69 (88%) h a d a correct prelimi- n a r y diagnosis on the b a s i s of history a n d physical e x a m ination alone. In 55 (80%) of t h e s e patients, the prelimi- n a r y d i a g n o s i s h a d b e e n c o n s i d e r e d " u n d o u b t e d . " a n d in 14 (2(YYo) "probable." Final diagnosis did not c o r r e s p o n d to p r e l i m i n a r y diagnosis in only 9 (12%) of the p a t i e n t s (Table 3). In 8 of t h e s e 9 patients, p r e l i m i n a r y d i a g n o s i s w a s m a d e with little confidence, a n a l o g o u s to the r e s u l t s in p a t i e n t s with a b d o m i n a l pain. Thus. the p r e l i m i n a r y diagnosis was rated as "probable" orgmfic disorder, mostly a n g i n a pectoris, in t h e s e patients. T h e s e 8 p a t i e n t s re ceived a final diagnosis of n o n o r g a n i c c h e s t pain. A single p a t i e n t received a n " u n d o u b t e d " p r e l i m i n a r y diagamsis of a n g i n a pectoris b a s e d on the p a t i e n t ' s history of m y o c a r dial inlZarction a n d a history of p e r c u t a n e o u s t r a n s l u m i - nal c o r o n a r y a n g i o p l a s t y (KFCA). However, t h a l l i u m scin tigraphy did not reveal any ischemia, w h i c h led to a final diagnosis of nonorganic c a u s e of pain despite the patient's history of c o r o n a r y h e a r t disease. Interestingly, t h i s p a tient w a s later found to have c o r o n a r y pain (successful PTCA. see below) in the follow-up investigation.
T h u s , all n o n o r g a n i c p r e l i m i n a r y d i a g n o s e s were c o r f e e t in 56 of 78 p a t i e n t s with c h e s t pain (Tables 2 a n d S).
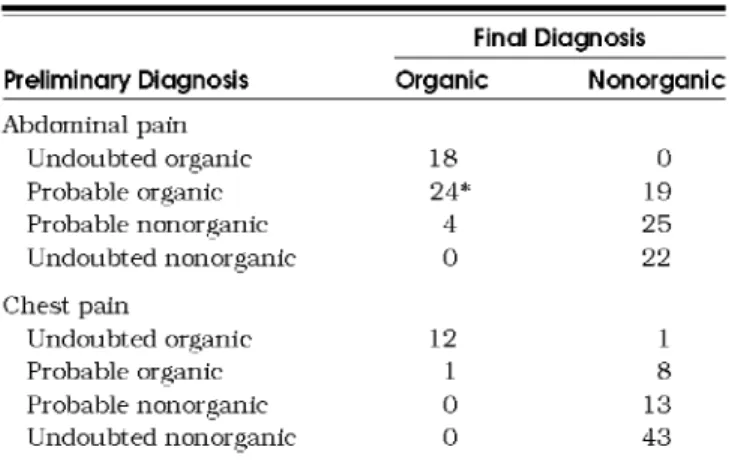
Table 3. Comparison of Final Diagnoses According to Confidence in Preliminary Diagnosis
Final Diagnosis
Preliminary Diagnosis Organic Nonorganic
Abdominal pain Undoubted organic 18 0 Probable organic 24* 19 Probable nonor~anic 4 25 Undoubted nonorganic 0 22 Chest pain Undoubted organic 12 1 Probable organic 1 8 Probable nonorganic 0 13 Undoubted nonorganic 0 43
*Eight patients had organic causes o f pctm dt~'erent from the one orgtnctlly suspected.
No orgmfic c a u s e of pain w a s missed. This m e a n s a speci- ficity of n o n o r g a n i c p r e l i m i n a r y diagnosis of 10(YYo (Table 2). Similar to a b d o m i n a l pain, a n exceedingly high speci ficity a n d sensitivity w a s r e a c h e d w h e n the t r e a t i n g physi- c i a n s rated the c a u s e of c h e s t pain as " u n d o u b t e d " or ganic or n o n o r g a n i c (Table 2).
F o l l o w - u p E x a m i n a t i o n of Patients with N o n o r g a n J c A b d o m i n a l or C h e s t Pain
Missing an organic c a u s e of pain t h a t is not i m m e d i ately a p p a r e n t on s t a n d a r d w o r k u p m i g h t have dire conse- q u e n c e s for a patient. It w o u l d therefore be of great ad- v a n t a g e to k n o w w h e t h e r a first clinical J u d g m e n t of a nonorgmfic cause of pain is reliable in the long term, To that end a n d to a s s e s s the final diagnosis serving as gold s t a n dard, we c o n d u c t e d a long t e r m follow up of 131 p a t i e n t s with a nonorgmfic a b d o m i n a l or c h e s t pain at final diag- nosis gold standard.
Thirty eight p a t i e n t s (29%) could n o t be r e a c h e d for follow-up investigation, Most of these p r e d o m i n a n t l y y o u n g p a t i e n t s (e.g., s t u d e n t s a n d expatriates) h a d m o v e d away. T h e i r diagnostic a n d d e m o g r a p h i c c h a r a c t e r i s t i c s are given in Table 4. Of 131 patients, 93 (71%) could be r e a c h e d for a follow up e x a m i n a t i o n after a m e a n of 29 m o n t h s (range 18~56 months). Of t h e s e patients, 46 h a d n o n o r g a n i c a b d o m i n a l pain a n d 47 h a d n o n o r g a n i c c h e s t p a i n a s their final diagnosis (Table 5). Patients h a d a tele p h o n e interview or c h e c k u p investigation at o u r institu tion. They were a s k e d a b o u t n e w d i a g n o s e s mid a b o u t the evolution of t h e i r pain s y m p t o m s .
Nonorganic Abdominal Pain.
Of the 46 p a t i e n t s t h a tcould be followed, p a i n h a d resolved completely in 15 (33%), improved in 10 (21%), r e m a i n e d u n c h a n g e d in 15 (33%). mid w o r s e n e d in 6 (13%) (Table 5). In three pa- tients who originally h a d a final d i a g n o s i s of n o n o r g a n i c a b d o m i n a l pain, the follow u p investigation revealed a n orgmfic diagnosis. Two p a t i e n t s h a d gastric ulcer, a n d one u n d e r w e n t s u r g e r y for diverticulosis of the colon. T h u s , a c c u r a c y in p a t i e n t s d i a g n o s e d as having n o n o r ganic a b d o m i n a l pain at final diagnosis w a s 92% w h e n c o m p a r e d with l o n & t e r m follow up.
N o n o r g a n i r
Chest Pain.
Of the 47 p a t i e n t s with c h e s t pain t h a t could be followed, pain had resolved completely inJGIM Volume 12. A u g u s t 1 9 9 7 463
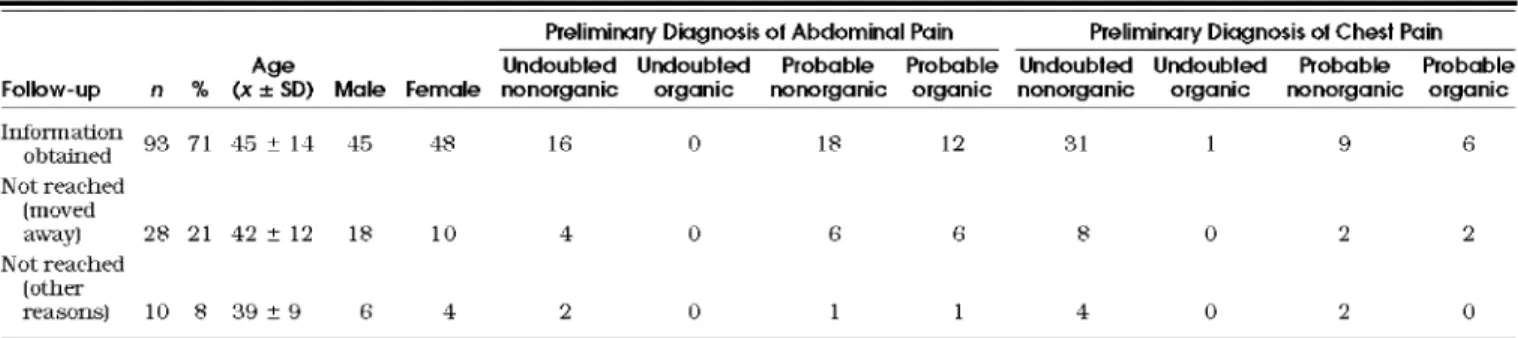
Table 4. Description of Patients with Nonorganic Diagnoses by Follow-up Status
Preliminary Diagnosis of Abdominal Pain Preliminary Diagnosis of Chest Pain
Age Undoub|ed Undoubled Probable Probable Undoubled Undoubled Probable Probable
Follow-up n % (x_+SD) Male Female nonorganic organic nonorganic organic nonorganic organic nonorganic organic
Illform a t i o n 93 71 45 + 14 45 48 1G 0 18 12 31 1 9 G obt't2~led N o t r e a c h e d [ m o v e d away) 28 21 42 _+ 12 18 10 4 0 6 6 8 0 2 2 N o t r e a c h e d [ o t h e r r e a s o n s ) 10 8 39 _+ 9 6 4 2 0 1 1 4 0 2 0 17 (36%), improved in 13 (28%), remained u n c h a n g e d in 11 (23%), a n d worsened in 6 (13%) (Table 5). The gold s t a n d a r d mid diagnosis w a s correct in 980/0. In one patient a final di- agnosis of nonorganic c h e s t pain had been made because of a negative r e s u l t on t h a l l i u m scintigraphy. A m o n t h later coronary h e a r t disease w a s detected at coronary angiogra- phy, a n d PTCA a b r o g a t e d the pain. Interestingly, the pre liminary diagnosis w a s "undoubted" organic c a u s e of pain.
D I S C U S S I O N
A b d o m i n a l pain, c h e s t pain, fatigue, b a c k pain, h e a d ache, a n d d y s p n e a are the m o s t f r e q u e n t s y m p t o m s in m e d i c a l outpatients,1 In the collective p a t i e n t s s c r e e n e d for o u r study, a b d o m i n a l p a i n a n d c h e s t p a i n were the m o s t c o m m o n complaints. This case mkx of o u t p a t i e n t s c o m p a r e s well with general internal practitioners in the local region, lr a n d o t h e r regions. 1 In o u t p a t i e n t s , 40% to 85% of c o m p l a i n t s have no discernible organic cause: i.e., t h e y are "nonorganic" in origin. 1,s,1~1 It m a y be crucial to diagnose a n o n o r g a n i c c a u s e of pain early in o r d e r to pre v e n t u n n e c e s s a r y w o r k u p a n d cost. 1,1s It m a t t e r s w h e t h e r p a t i e n t s cml be diagnosed reliably a n d early with a nonor- ganic c a u s e of pain, a l t h o u g h this m a y be more difficult t h a n in pain of organic origin. To appraise w h e t h e r a n o n
organic diagnosis c a n be d i s t i n g u i s h e d reliably from an organic one by clinical m e a n s alone, we prospectively s t u d i e d 190 c o n s e c u t i v e general medical o u t p a t i e n t s with a b d o m i n a l or c h e s t pain,
Table 5. Outcome at Long-Temn Follow-up of 93 Patients with Nonorganic Abdominal or Chest Pain
Abdominal Pain Chest Pain Outcome (n = 46) (n = 47) FoUow-up dia~losis Nonor~anic 43 46 Organic 3 1 Symptom status Resolved 15 (33) 17 (36) Improved 10 (21) 13 (28) Unchanged 15 (33) 11 (23) Worsened 6 (13) 6 (13) A clinical J u d g m e n t b a s e d on p a t i e n t history a n d p h y s i c a l e x a m i n a t i o n alone correctly predicted final diag n o s i s at completion of the c h a r t in b o t h a b d o m i n a l (72%) a n d c h e s t pain (88%). W h e n a distinction b e t w e e n n o n o r ganic a n d organic pain, b u t n o t a precise diagnosis, w a s made, a c c u r a c y i n c r e a s e d to 79% for a b d o m i n a l pain a n d r e m a i n e d at 88% for c h e s t pain. T h e s e findings m a t c h o t h e r reports on the pivotal diagnostic c o n t r i b u t i o n of careful history taking a n d physical e x a m i n a t i o n alone in v a r i o u s p a t i e n t populations. 1,~>e.,11-zs,~
Medical p r a c t i t i o n e r s often rely on experience a n d feelings t h a t are d e s c r i b e d a s "probable" or " u n d o u b t e d . " Here we provide some evidence c o n c e r n i n g the a d e q u a c y of s u c h t e r m s in the c o n t e x t of n o n o r g a n i c v e r s u s organic a b d o m i n a l mid c h e s t pain, The p r e l i m i n a r y diagnosis w a s a l m o s t completely a c c u r a t e w h e n residents, t o g e t h e r with t h e i r s u p e r v i s i n g a t t e n d i n g physicians, felt very confident a b o u t t h e i r p r e l i m i n a r y diagnosis. A c c u r a c y of a n "un- doubted" p r e l i m i n a r y d i a g n o s i s w a s 99% c o m p a r e d with the final diagnosis. Conversely, the a c c u r a c y of a "proba ble" p r e l i m i n a r y diagnosis of a b d o m i n a l p a i n a n d c h e s t p a i n c o m p a r e d with the final diagnosis w a s only 68% a n d 64%, respectively.
One m i g h t argue t h a t p a t i e n t s with a n " u n d o u b t e d " p r e l i m i n a r y d i a g n o s i s only rarely h a d additional investi g a t i o n s to dispel t h e i r initial diagnosis, However. the fol- low-up investigation of p a t i e n t s with nonorgmlic final di- a g n o s i s after an average of 29 m o n t h s (range 18~56 months) did not identify a n y e r r o n e o u s J u d g m e n t in the s u b s e t of p a t i e n t s with " u n d o u b t e d " diagnoses, Diagnos- tic a c c u r a c y for b o t h u n d o u b t e d a n d probable n o n o r g a n i c final d i a g n o s e s after completion of the c h a r t (gold s t a n - dard) in p a t i e n t s with a b d o m i n a l a n d c h e s t p a i n w a s 93% a n d 98%, respectively, a s c o m p a r e d with the follow up in vestigation. This is c o m p a r a b l e to a report of 100 p a t i e n t s followed for n o n o r g a n i c a b d o m i n a l pain who were as- s e s s e d with a n equally high diagnostic a c c u r a c y of 95%. 14 O u r s t u d y did n o t a i m to d i s c e r n w h e t h e r p a t i e n t his tory or p h y s i c a l e x a m i n a t i o n c o n t r i b u t e d more to diag- nostic accuracy. However, p a t i e n t history i n f l u e n c e s diag nostic e v a l u a t i o n more t h a n physical e x a m i n a t i o n does, the latter revealing crucial i n f o r m a t i o n in a p p r o x i m a t e l y 20% or less of all cases, r,l>ls O u r follow up investigation revealed an i m p r o v e m e n t of n o n o r g a n i c a b d o m i n a l p a i n
464 M a r t i n a et ~ , . First D ~ g r ~ s i s in A b d o m i n ~ or C h e s t P a i n JG1M i n a p p r o x i m a t e l y 5 0 % o f t h e p a t i e n t s . S i m i l a r l y , n o n o ~ g m n c a b d o m i n a l p a i n . s o t h e r g a s t r o i n t e s t i n a l c o m p l a i n t s , s a n d m i s c e l l a n e o u s s y m p t o m s I i m p r o v e d i n a p p r o x i m a t e l y h a l f o f all c a s e s a f t e r a p r o l o n g e d o b s e r v a t i o n p e r i o d . N o n o r g a n i c c h e s t p a i n i n o u r p a t i e n t s i m p r o v e d i n 64o/o, S i m i - l a r r e s u l t s w e r e r e p o r t e d i n p a t i e n t s w i t h a t y p i c a l c h e s t p a i n a n d n o r m a l c o r o n a r y arteries.ZS' T h e s e a r c h for low c o s t a n d h i g h - q u a l i t y c a r e is o n g o i n g , P a t i e n t w i s h e s f o r i n - t e r v e n t i o n s h a v e to b e c o n s i d e r e d . ~s Yet o u r d a t a , a s well a s o t h e r s " ~4 s u g g e s t t h a t l o w e r c o s t is n o t n e c e s s a r i l y a s s o c i a t e d w i t h low q u a l i t y o f c a r e , W e c o n c l u d e t h a t o n l y d i a g - n o s e s o f n o n o r g a n i c p a i n t h a t a r e r a t e d a s " p r o b a b l e " n e e d f u r t h e r i n v e s t i g a t i o n s a n d w o r k u p . O u r s t u d y h a s s e v e r a l l i m i t a t i o n s . F i r s t . o u r c o n s e c u - tive o u t p a t i e n t s w i t h a b d o m i n a l o r c h e s t p a i n a r e b e t t e r s u i t e d for t h e s t u d y o f n o n o r g a n i c c a u s e s o f p a i n t h a n o ~ g a n i c o n e s . T h e n u m b e r o f o u r p a t i e n t s w i t h o r g a n i c d i a g - n o s e s i s r e l a t i v e l y s m a l l , h e t e r o g e n e o u s , a n d r e p r e s e n t s a l i m i t e d n u m b e r o f d i s e a s e s w i t h a l o w n u m b e r o f c a s e s i n e a c h c a t e g o r y o f d i s e a s e , T h i s . a n d t h e h i g h p r e v a l e n c e o f p o o r l y c i r c u m s c r i b e d c o m p l a i n t s o f a b d o m i n a l a n d c h e s t p a i n i n d a i l y m e d i c a l p r a c t i c e . 1,~- l e d u s to f o c u s o n t h e re l i a b i l i t y o f d i a g n o s e s for n o n o r g a n i c c a u s e s o f p a i n . S e c o n d , e a c h p a t i e n t h a d h i s o r h e r i n d i v i d u a l w o r k u p : e.g., i n v e s t i g a t i o n s s u c h a s t r e a d m i l l e r g o m e t r y o r e n d o s c o p y w e r e p e r f o r m e d o n l y w h e n c l i n i c a l l y i n d i - c a t e d . I n d i v i d u a l i z a t i o n o f w o r k u p h a s a l s o b e e n de s c r i b e d i n o t h e r s i m i l a r s t u d i e s t h a t r e f l e c t c o n d i t i o n s o f d a i l y m e d i c a l p r a c t i c e , 1,s T h i r d . a s h o r t c o m i n g o f a n y in- v e s t i g a t i o n like o u r s i s t h e l a c k o f a t o t a l l y r e l i a b l e g o l d s t a n d a r d . I n o u r s t u d y t h e f i n a l d i a g n o s i s s e r v e d a s a g o l d s t a n d a r d to m e a s u r e t h e q u a l i t y o f t h e p r e l i m i n a r y d i a g - n o s i s . H o w e v e r , s t a n d a r d i z e d a n d m o r e a g g r e s s i v e i n v e s t i g a t i o n s m a y h a v e s o m e w h a t a l t e r e d t h e f i n a l d i a g n o s i s . T o a s s e s s t h e g o l d s t a n d a r d , w e p e r f o r m e d a f o l l o w - u p i n - v e s t i g a t i o n o f n o n o r g a n i c d i a g n o s i s . It w a s p o s s i b l e to r e a c h 7 1 % o f t h e p a t i e n t s . It a p p e a r e d t h a t o u r g o l d s t a n d a r d w a s v e r y g o o d . 9 3 % for a b d o m i n a l p a i n a n d 9 8 % f o r c h e s t p a i n . F o u r t h . s c r e e n i n g for p s y c h i a t r i c c o n d i t i o n s w a s n o t p e r f o r m e d . A n u m b e r o f n o n o r g a n i c d i a g n o s e s i n o u r p a - t i e n t s c o u l d h a v e b e e n b e t t e r c i r c u m s c r i b e d a n d d e f i n e d w i t h q u e s t i o n n a i r e s s u c h a s t h e P R I M E - M D p a t i e n t q u e s - t i o n n a i r e . ~c' W e d i d n o t s t r i v e to m a k e a s p e c i f i c d i a g n o s i s i n p a t i e n t s w i t h p a i n o f n o n o r g a n i c origin. Yet, f u r t h e r p s y c h o l o g i c a l w o r k u p a n d c a r e a r e c l e a r l y n e c e s s a r y i n t h e s e p a t i e n t s , ~ W i t h t h e s e l i m i t a t i o n s i n m i n d , o u r s t u d y still i n d i c a t e s t h a t a n " u n d o u b t e d " p r e l i m i n a r y n o n o r g a n i c d i a ~ n o s i s i s h i g h l y p r e c i s e a n d r e l i a b l e . T h e s p e c i f i c i t y o f 1 0 0 % s h o w s t h a t n o o r g a n i c d i a g n o s i s w a s m i s s e d . T h u s , w a t c h f u l w a i t i n g w i t h little o r n o a d d i t i o n a l l a b o r a t o r y o r o t h e r i n v e s t i g a t i o n s i s a p p r o p r i a t e i n t h e s e c a s e s , I n c o n c l u s i o n , t h i s s t u d y d e m o n s t r a t e s t h a t t h e f i r s t J u d g m e n t o f e x p e r i e n c e d p h y s i c i a n s b a s e d o n c a r e f u l p a t i e n t h i s t o r y a n d p h y s i c a l e x a n l i n a t i o n a l o n e i s r e l i a b l e i n m e d i c a l o u t p a t i e n t s w i t h a b d o m i n a l o r c h e s t p a i n . Reli a b i l i t y i n c r e a s e s w i t h t h e c o n f i d e n c e w i t h w h i c h t h e d i a g - n o s i s c a n b e m a d e . I n p a t i e n t s t h a t h a v e b e e n c o n f i d e n t l y d i a g n o s e d w i t h a n o n o r g a n i c c a u s e o f p a i n , t h e r e d o e s n o t s e e m to b e a n e e d f o r a d d i t i o n a l w o r k u p , A v o i d i n g u n n e c - e s s a r y w o r k u p m a y c o n t r i b u t e to h i g h - q u a l i t y a n d low- c o s t a m b u l a t o r y m e d i c i n e . F u r t h e r s t u d i e s to e v a l u a t e t h e a p p r o p r i a t e i n v e s t i g a t i o n s a r e r e q u i r e d i n a m b u l a t o r y c a r e p a t i e n t s w i t h n o n o r g a n i c c o m p l a i n t s .
The authors thank H.C. Bucher, MD, MPH, and M, B(#tegay, MD, for discussing and expertly reviewing the manuscript. Mrs. F. Vogel and $. Jaquemet are acknowledged for their out- st(mding secret(~ri(~l assistc~nce~
REFERENCES
1. Kroenke K, Mangelsdorff AD. Common symptoms in ambulatory care: incidence, evaluation, therapy and outcome. Am J Med. 1989: 8 6 : 2 6 2 ~ .
2. M a r ~ t a B. Konsultations._eytinde i n der a m b u l a n t e n an_~emeinen im~eren Medizin, Schweiz R u n d s c h Med Prax, 1994:83:1 2, 3, Bleijenberr G, Fermis J F M , Anamnestic and psycholo.~ical tea
tm-es in diagnosis a11d pro.alosis of functional abdominal cam plahlts: a prospective study, Gut. 1989:30:1076 81,
4. Kroe~kke K. Lucas CA, Rosenbei~ ME. et al. Causes of persistent dizziness. Ann Intern Med. 1992:117:898-904.
5. Deyo R/k Rainville J, Kent DL. What can the history and physical examination tell u s about low back pain? JAMA. 1992: 268:760-5. 6. Schmitt BP, Kushner MS, Wiener SL. The dia_~nostic usefulness of
the history of the patient with dyspnea, J Gen Intern Med. 1986: 1:38643,
7. Hampton JR, Harrison MDG. Mitchell JRA. }h-ichm-d JS, Seymom- C. Relative conti-ibutions of histoi~al~hl.g, physical e,~amination and laboratory investigation to dia~losis and mailagement of medical outpatients. BMJ. 1975;2:486-9.
8. Kroenke K, Arrin.gton ME, Man.gelsdorff AD. The prevalence of symptoms in medical outpatients and the adequacy of therapy. Arch Intern Med. 1990; 150:1685-9.
9. Komaroff AL. Minor illness symptoms. Arch Intern Med. 1990: 150:1586 7.
10. Katon W. Kleinmai1 A. Rosen G. Depression and somatization a review, A m J Med, 1982:72:12745. 241 7,
11. Rich EC. Crowson TW. Harris IB, The dia.alostic value of the reed ical history. Arch Intern Med. 1987; 147:1957-68.
12. Peterson MC, Holbrook JH, Van Hales DE, Smith NL Staker LV. Contributions of the history, physical examination and laboratory examination in making_ medical diagnoses. W e s t J Med. 1992; 156:
1 6 3 - 5 .
13. Smldler G, The importance of the history in the medical clinic and the cost of urmecessary tests, Am Heart J. 1980:100:928 31, 14. Svendsen JH. Mmlck LK. Andersen JR. In-itable bowel syn
drom~pro.gnosis and dia.alostic safety, A 5 year tallow up study. Scalld J Gastroenterol. 1985:130:1171 3,
15. Lanti.ga LJ, Spranfkin RP, McCroskery JH, Baker MT, Warner RA~ Hill NE. One-year psychosocial follow-up of patients with chest pain and an_~io.graphically normal coronary arteries. Am J Cardiol. 1988;62:209-13.
16. Holma11 CDJ, Analysis of hlterobserver variation on a pro.a-aroma ble calculator. Am J Epidemiol, 1984:120:15-t60.
17. Koechlhl PH. Kulsti-mkk M. Dubach UC. Vermittelt das Ambulato rium ehler Medizinischen Universit~its PoliklhKk genfi.gend praxis bezo.gene Weiterbildml.~? Schweiz Ae~ztezeitmlg. 1991:72:206 9,
JGIM Volume 12. A u g u s t t 9 9 7 465
18, F r y m o y e r J W . B a c k p a i n a n d sciatica. N En~l J Med. 1988:318: 291 300,
19. W o o d h o u s e CRJ, B r o c k n e r S. C h r o n i c a b d o m i n a l pain: a s u r . ~ c a l o r p s y c h i a t r i c s y m p t o m ? B r J S u r g . 1979; 6 6 : 3 4 8 - 9 .
20. Manning._ AP, T h o m p s o n WG, H e a t o n KW, Morris AF. T o w a r d s p o s - itive dia._anosis of t h e irritable bowel. BMJ. 1 9 7 8 ; 2 : 6 5 3 - 4 . 21. Cohen D, Frey D. Colon i r r i t a b f l ~ a oder n d n ? Ist die A n a m n e s e
eine Entscheidun~shilfe? Schweiz ivied Wochensclar, 1 9 8 2 : 1 1 2 : 5 3 1 4 .
22, K a p o o r WN. D i a g n o s t i c e v a l u a t i o n of s y n c o p e . Am J Med, 1991: 90:91 106,
23. E m a n u e l L. The s e a r c h for l o w - c o s t - h i g h q u a l i t y care. J G e n In- t e r n Med. 1 9 9 5 : 1 0 : 2 3 2 - 3 .
24. Staffield B, P o w e r N, Weiner J R . et al. C o s t s v s q u a l i t y i n different t y p e s of p r i m a r y c a r e setiings. JAMA. 1 9 9 4 ; 2 4 : 1 9 0 3 ~ .
25. K r o e n k e K, Spitzer RL, Williams JBW, et al. P h y s i c a l s y m p t o m s i n pi-imary care. A r c h Faro Med, 1 9 9 4 : 3 : 7 7 4 ~ .