Effect of midazolam on transfer function between beat-to-beat arterial pressure and inter-beat interval length
7
0
0
Texte intégral
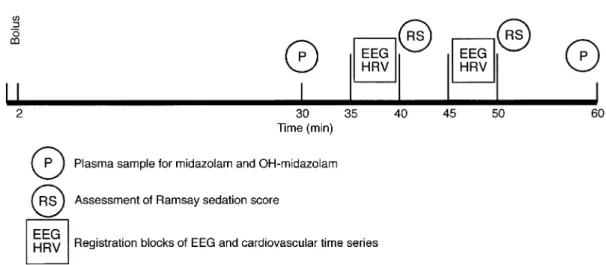
(2) Scha¨ chinger et al.. Fig 1 Sequence of procedures during one infusion period.. (greater than 0.15 Hz) components of this association.5 However, the role of these techniques for monitoring the sedative effects of drugs needs to be investigated further. Thus, we performed a volunteer study to assess the effects of midazolam on APV, HRV and on transfer functions between AP and IBI using a simple dose regimen which also included administration of the benzodiazepine antagonist flumazenil. An electroencephalogram (EEG) was assessed simultaneously as a standard technique for monitoring sedative effects.. Subjects and methods The study was performed according to the principles of the Declaration of Helsinki and was approved by the Local Ethics Committee of the Department of Medicine, University Hospital of Basel. We studied 11 male, healthy, non-smoking volunteers (aged 23–42 yr). All volunteers had a normal physical examination, and electrocardiography, routine blood chemistry and haematology and urine analysis were normal, with no evidence or history of illicit drug abuse or use of sedatives. Participants signed an informed consent before participating in the study. Subjects entered the hospital at 08:00 after a light breakfast without caffeine-containing beverages. The study took place in the intensive care unit ward to guarantee optimal monitoring. Two peripheral venous lines were inserted into antecubital veins. Subjects were in supine position throughout the experiment. The sequence of interventions is illustrated in Figure 1. Five successive periods were studied (see Fig. 1). The first was a 60-min control period. During the second experimental period, midazolam 0.02 mg kg–1 was administered i.v., half of the dose as a bolus (0.01 mg kg–1 over 2 min) followed by continuous infusion of the remainder. (0.01 mg kg–1 over the remaining 58 min). During the third and fourth experimental periods, midazolam 0.06 and 0.14 mg kg–1 were given by bolus and infusion as above. The total dose of midazolam for a subject with a body weight of 70 kg was 15.4 mg. During the fifth experimental period, midazolam infusion was stopped and the benzodiazepine antagonist flumazenil was given i.v. (0.002 mg kg–1 as a bolus followed by 0.002 mg kg–1 as a constant infusion over the remaining hour) while the agonist was still present. Plasma samples were obtained 30 min after the start of each period and at the end of each period (60 min). Samples were centrifuged and stored at –20°C for HPLC analyses of midazolam7 with a detection limit of 1 ng ml–1. During the flumazenil period, the 60-min sample was omitted. Averages of 30- and 60-min plasma midazolam concentrations were calculated.. Monitoring of cardiovascular data During each infusion period, two 5-min blocks of cardiovascular and ECG data were recorded simultaneously. Non-invasive arterial finger AP was assessed continuously using the Finapres system.8 Beat-to-beat systolic and diastolic AP were determined offline from the Finapres analogue output. Single-lead electrocardiogram was stored on personal computer (PC) by analogue to digital (AD) conversion (1 kHz per channel) for offline determination of IBI length. Ventilatory frequency was assessed by inductive plethysmography. Pulse oximetry was monitored continuously and standard cuff AP intermittently (Dinamap, Criticon, Florida, USA) for safety reasons.. Beat-to-beat analysis APV was calculated by fast Fourier transform (FFT) after equidistant representation of systolic AP data.9 HRV was determined by low-pass filtering of the event series (LPFES. 317.
(3) Midazolam effect on cardiovascular transfer function. method), as suggested by Rompelman, Snijders and van Spronsen.10 APV and HRV were analysed for each of the following frequency bands: total band (0.02–0.5 Hz), high band (0.15–0.4 Hz), low band (0.07–0.14 Hz) and very low band (0.02–0.06 Hz). HRV was adjusted to mean HR (modulation index, MI) as suggested previously.11 All variables were log-transformed to achieve normally distributed measures; HRV was expressed as ln MI2 and APV as ln mm Hg2. Transfer function analysis of beat-to-beat changes in IBI length and systolic AP data was performed using ACTS software in accordance with previous publications.6 12 13 The modulus gain function was calculated over the frequency range 0.02–0.5 Hz. The modulus gain function is expressed in ms mm Hg–1. For further statistical analysis, this function was adjusted to the coherence function, as suggested previously.6 For graphical illustration of the modulus gain function over the entire spectrum (0.02–0.5 Hz), it was not adjusted to the coherence function between systolic AP and IBI length. We calculated separately the low and high frequency components of the transfer function between systolic AP and IBI by integrating the modulus gain function over the low and high frequency bands, thus resulting in two variables (LF and HF components of the transfer function between systolic AP and IBI). All variables were first derived for each 5-min block and then averaged between both blocks.. EEG registration At the same time as cardiovascular variables were assessed, EEG data were recorded from FP1-T3, T3-O1, FP2-T4, T4-O2 (according to the International 10–20 System) with the subject’s eyes closed. Ground was placed at the central forehead. The skin was prepared to yield impedance values lower than 3 kW at each electrode site. A Moberg Neurotrac II Continuous EEG Monitor (frequency range 0.5–45 Hz) was used to display and store (AD conversion 12 bit, 128 Hz) EEG data in consecutive 2-s epochs. To minimize artefacts, a 50-Hz notch filter was used. Variables analysed by FFT for each epoch included absolute power in the following frequency bands: entire spectrum (1.0–30.0 Hz), α power (8.0–12.5 Hz), β1 power (12.5–20.0 Hz), β2 power (20.0–30.0 Hz), δ power (1.0–4.0 Hz) and θ power (4.0– 8.0 Hz). Because of the skewed distribution of absolute power values, natural logarithmic transforms (ln) were calculated. In addition, power in each frequency band was calculated as percentage of total power for each 2-s epoch, respectively. Median values of all EEG variables were calculated for each of the 5-min blocks, respectively. Averages of the two blocks were then calculated to yield final values which were entered into the statistical analysis. Because of this procedure the power values presented may not necessarily add up to 100%.. Subjective sedation score Subjects were rated by two physicians according to a scale proposed by Ramsay and colleagues.14 The Ramsay sedation. score is defined as follows: awake levels—(1) anxious and/ or agitated; (2) co-operative, oriented, and tranquil; (3) responds to commands; asleep levels—(4) quiescent with brisk response to light glabelar tap or loud auditory stimulus; (5) sluggish response to light glabelar tap or loud auditory stimulus; and (6) no response. Scores of the two physicians were averaged.. Statistical analysis All statistical calculations were performed using SAS software (release 6.12, SAS Institute Inc., Cary, NC, USA). Data are reported as mean (SEM). A repeated measures analysis of variance (SAS General Linear Model Procedure) was applied for multivariate testing of dose and drug effects. Averages of the Greenhouse–Geisser and Huynh–Feldt adjusted P values are reported.15 Contrasts between the third midazolam infusion period and flumazenil period were constructed a priori (non-adjusted P values are reported in tables). All testing was two-tailed. P⬍0.05 was considered significant.. Results Midazolam and flumazenil were well tolerated by all subjects. No adverse events occurred during infusion and pulse oximetry revealed no clinically significant desaturation. Plasma midazolam concentrations at 30 and 60 min for each period are shown in Table 1. Ramsay sedation scores increased with higher doses of midazolam (baseline, median 2 (range 1–2); midazolam infusion of 0.02 mg kg–1, 3 (2–4); midazolam infusion of 0.06 mg kg–1, 4 (4–5); midazolam infusion of 0.14 mg kg–1, 5 (4–6)) and decreased during flumazenil infusion (3 (2–4)). Power analysis of EEG data revealed decreasing α power, increasing δ power and increasing β1 power. All of the above effects were reversible during infusion of flumazenil (Table 2). AP, HR and respiratory frequency data are shown in Table 3. HR and respiratory frequency increased whereas AP remained unaffected during infusion of midazolam. In general, there was an increase in HRV and APV (Table 4) during the first midazolam dose followed by a decrease during higher midazolam doses. Administration of flumazenil did not result in significant changes in HRV or APV. However, the fast component (0.15–0.4 Hz) of the transfer function between AP and IBI showed a very close dose– response association to midazolam and this index increased substantially after administration of flumazenil. This was not true for the low frequency component. Figure 2 illustrates the averaged transfer functions between AP and IBI with increasing dose of midazolam. There was substantial overlap of the low frequency component (0.07–0.14 Hz) of the transfer function at different midazolam doses. This was not the case for the high frequency component. Figure 3 indicates that infusion of flumazenil induced an increase in the fast component of the transfer function between AP. 318.
(4) Scha¨ chinger et al. Table 1 Mean (SEM) plasma concentrations of midazolam (MDZ) and 1-α-hydroxy-midazolam (OH-MDZ) 30 and 60 min after the onset of midazolam and flumazenil (FLU) infusions. *Below the limit of detection, na⫽not applicable Plasma concn MDZ (ng ml–1) OH-MDZ (ng. ml–1). Time (min). Baseline. MDZ (0.02 mg kg–1). MDZ (0.06 mg kg–1). MDZ (0.14 mg kg–1). FLU (0.03 mg kg–1). 30 60 30 60. * * * *. 12.8 (3.8) 11.5 (2.5) 1.4 (0.4) 0.7 (0.4). 36.8 36.6 2.2 2.7. 94.4 90.5 5.6 6.5. 62.9 (4.0) na 7.1 (0.8) na. (2.7) (1.9) (0.4) (0.4). (4.3) (4.8) (0.7) (1.0). Table 2 Mean (SEM) EEG variables (α 8–12.5 Hz, β1 12.5–20 Hz, β2 20–30 Hz, δ 1–4 Hz, q 4–8 Hz) during midazolam (MDZ) and flumazenil (FLU) infusions. Relative α power decreased, β1 power and δ power increased progressively with higher midazolam doses; all of these effects were antagonized by flumazenil. p1⫽Repeated measures ANOVA for baseline/midazolam effect; p2⫽linear contrast between highest level of midazolam infusion and flumazenil period EEG variable Log power (ln µV2) α power β1 power β2 power δ power θ power Total power Relative (%) α power β1 power β2 power δ power θ power. MDZ (0.02 mg kg–1). Baseline. MDZ (0.06 mg kg–1). MDZ (0.14 mg kg–1). FLU (0.03 mg kg–1). p1. 5.9 4.1 3.7 5.5 4.8 6.8. (0.4) (0.1) (0.1) (0.1) (0.2) (0.2). 5.1 4.5 3.4 6.4 5.1 7.1. (0.3) (0.2) (0.1) (0.2) (0.2) (0.1). 5.0 4.7 3.2 7.6 5.4 8.0. (0.2) (0.1) (0.1) (0.3) (0.2) (0.2). 5.1 5.2 3.6 7.4 5.1 7.9. (0.2) (0.3) (0.3) (0.3) (0.1) (0.2). 0.005 0.0001 0.05 0.0001 0.04 0.0006. 40.9 9.4 6.7 32.9 14.7. (6.2) (1.3) (1.0) (3.6) (1.5). 19.7 8.6 3.6 53.1 14.6. (6.2) (1.0) (0.8) (4.0) (1.1). 10.5 5.4 1.7 72.6 8.8. (5.3) (0.8) (0.7) (4.6) (0.6). 8.9 14.3 3.4 65.5 6.7. (3) (5.8) (1.5) (7.9) (0.6). 0.0001 0.21 0.008 0.0001 0.0002. 4.8 4.6 3.9 5.5 4.4 6.6. (0.4) (0.2) (0.2) (0.1) (0.2) (0.1). 25.4 (6.4) 16.7 (2.5) 8.9 (1.4) 38.2 (4.0) 11.8 (0.6). p2. 0.62 0.008 0.21 0.001 0.01 0.001 0.01 0.54 0.008 0.005 0.0001. Table 3 Mean (SEM) heart rate increased with higher doses of midazolam (MDZ) and decreased during flumazenil (FLU) infusion. Arterial pressure and respiratory frequency did not change significantly. p1⫽Repeated measures ANOVA for baseline/midazolam effect; p2⫽linear contrast between highest level of midazolam infusion and flumazenil period. Heart rate (beat min–1) Systolic arterial pressure (mm Hg) Diastolic arterial pressure (mm Hg) Respiratory frequency (Hz). Baseline. MDZ (0.02 mg kg–1). MDZ (0.06 mg kg–1). MDZ (0.14 mg kg–1). p1. FLU (0.03 mg kg–1). p2. 59 (2.6) 119 (1.2). 62 (3.3) 120 (1.6). 67 (3.7) 117 (2.5). 72 (5) 118 (2.1). 0.01 0.48. 63 (3.6) 119 (2.7). 0.002 0.23. 63 (2). 65 (2.4). 60 (2.6). 61 (1.6). 0.13. 64 (3). 0.29. 0.23 (0.01). 0.23 (0.01). 0.25 (0.01). 0.27 (0.02). 0.06. 0.26 (0.01). 0.59. Table 4 Mean (SEM) heart rate variability, arterial pressure variability and transfer function magnitude between arterial pressure and inter-beat-interval (IBI) length in different frequency bands during midazolam (MDZ) and flumazenil (FLU) infusions. Frequency bands are defined as VLF⫽very low frequency, LF⫽ low frequency, HF⫽high frequency. Transfer magnitude in the HF range decreased progressively with higher midazolam doses and this effect was antagonized by flumazenil. p1⫽Repeated measures ANOVA for baseline/midazolam effect; p2⫽linear contrast between highest level of midazolam infusion and flumazenil period Baseline Heart rate variability, log-transformed (ln MI2) Total band (0.01–0.5 Hz) VLF (0.02–0.06 Hz) LF (0.07–0.14 Hz) HF (0.15–0.4 Hz) Arterial pressure variability, log-transformed (ln mm Hg2) VLF (0.02–0.06 Hz) LF (0.07–0.14 Hz) Transfer function between arterial pressure and IBI (ms mm Hg–1) LF (0.07–0.14 Hz) HF (0.15–0.4 Hz). 8.2 6.7 6.9 7.3. (0.3) (0.2) (0.3) (0.4). MDZ (0.02 mg kg–1). 8.9 7.6 7.4 7.6. (0.2) (0.2) (0.2) (0.4). MDZ (0.06 mg kg–1). 8.1 6.6 6.4 7.2. (0.2) (0.2) (0.2) (0.3). MDZ (0.14 mg kg–1). p1. 8.0 6.9 6.3 6.4. (0.3) (0.4) (0.5) (0.5). 0.06 0.05 0.03 0.18. 8.5 7.4 7.1 7.1. (0.4) (0.3) (0.3) (0.5). 0.35 0.45 0.17 0.21. 2.4 (0.2) 1.5 (0.2). 0.43 0.82. 14.0 (3.2) 21.5 (3.2). 0.22 0.002. 2.5 (0.2) 1.5 (0.2). 3.3 (0.2) 2.0 (0.2). 2.7 (0.4) 1.4 (0.3). 2.7 (0.4) 1.5 (0.4). 0.11 0.02. 15.4 (2.2) 26.5 (3.7). 14.1 (2.4) 19.2 (2.9). 9.2 (1.3) 12.8 (1.7). 8.5 (1.4) 8.4 (1.6). 0.03 0.0003. 319. FLU (0.03 mg kg–1). p2.
(5) Midazolam effect on cardiovascular transfer function. Fig 2 Transfer function between systolic arterial pressure (AP) and interbeat interval (IBI) length during baseline and drug infusion. The high frequency component (0.15–0.4 Hz) of the transfer function between AP and IBI decreased according to the midazolam infusion dose. Substantial overlapping of the low frequency component (0.07–0.14 Hz) is evident. Data are mean (SEM).. Fig 3 Increasing magnitude of the transfer function between systolic arterial pressure and inter-beat interval length during infusion of flumazenil. Data are mean (SEM).. and IBI. This fast component represented the only variable which decreased progressively with increasing dose of midazolam and increased again after administration of flumazenil in each subject (for individual changes see Fig. 4).. Discussion Our main finding was that the high frequency component (0.15–0.40 Hz) but not the low frequency component (0.07– 0.14 Hz) of the transfer function between systolic AP and IBI revealed a close relationship to midazolam dose, plasma concentration and antagonism with flumazenil. High and low frequency components of the transfer function between AP and IBI are influenced by baroreflex HR control.5 16 17 Indeed, transfer function analysis may be used to estimate baroreflex sensitivity.6 12 18–23 Frequently, the magnitudes of the high and low frequency components have been averaged18 19 to yield a single variable. However,. Fig 4 Individual data revealing progressive decrements of the high frequency (HF) component of the transfer function between systolic arterial pressure and inter-beat interval length in all subjects (only one subject showed an increase in the last midazolam infusion period) during midazolam infusion, and increments during flumazenil infusion.. baroreflex efferents are divided into two pathways: the fast parasympathetic branch to the sinus node and to other cardiac regions via the vagus nerve and the sympathetic branch, which is characterized by a slower signal transduction to cardiac and vascular effector cells. High frequency components (greater than 0.15 Hz) of AP and HR variations, therefore, cannot be of sympathetic origin. Modern signal analysis techniques, such as the transfer function analysis of beat-to-beat AP and HR data which were used in our investigation, make it possible to estimate the magnitude of the transfer function between AP and HR data separately in the vagally dominated high frequency range and in the low frequency range (which is believed to be of mixed sympathetic and parasympathetic origin).24 We believe that this differentiation is of major importance as previous studies in animals have indicated an effect of benzodiazepines only on the vagal component of baroreflex HR control25–29 whereas the sympathetic component remained unaffected. Our results are in accordance with animal data during pentobarbital anaesthesia when cross-spectral analysis of AP and HR revealed a gradual and dose-related decrease in the magnitude of the transfer function between AP and HR and baroreflex sensitivity.30 Flumazenil antagonized the effects of midazolam on the fast component of the transfer function between AP and HR data. Flumazenil was given in the presence of midazolam. We cannot speculate about the intrinsic effects of flumazenil on baroreflex function and the transfer function between AP and HR data. One might expect increased baroreflex HR control, but data from animal studies indicated decreased baroreflex sensitivity after administration of benzodiazepine partial inverse agonists.31 Thus this issue remains to be studied. Traditional determination of baroreflex sensitivity in humans does not distinguish between sympathetic and parasympathetic effects of HR control.32 Using standard. 320.
(6) Scha¨ chinger et al.. techniques, it was shown that the sedative effects of benzodiazepines were accompanied by attenuated baroreflex HR control,33 which is opposite to the effects of normal sleep.34 Several studies have addressed HRV during anaesthesia.35 In our well controlled investigation of healthy volunteers, we found decreased HRV during higher midazolam doses, as was suggested by previous work.36 37 Using standard EEG techniques, we replicated the benzodiazepine-induced EEG changes and flumazenil effects described by others. This was true for the spectral EEG measures δ power, β power and α power.38 However, several disadvantages limit the use of EEG techniques in routine clinical practice. The raw EEG signal is delicate, complex and needs to be judged correctly by trained staff. Furthermore, several procedures have been proposed to distinguish EEG changes during sedation (i.e. subjective judgement methods of the raw EEG signals; quantitative methods such as Fourier transformation; aperiodic analysis of EEG waveforms).39 Complex, non-linear effects of benzodiazepines on the EEG have been described39 thus making interpretation of EEG measures even more difficult. It is promising that assessment of the transfer function between AP and IBI is not limited by such disadvantages. There would be no need for additional equipment other than that already used for cardiovascular monitoring, such as electrocardiography and continuous AP monitoring. Assessment does not depend on behavioural activity or verbal report, and may be obtained during neuromuscular block. A single variable can be derived. A disadvantage of the method is that it is applicable only in the presence of a sinus rhythm. In summary, our investigation in healthy young volunteers revealed a close association between midazolam dose and spectral assessment of the fast component of the transfer function between AP and IBI. We suggest the use of frequency domain-based transfer function analysis for monitoring of the effects of midazolam in further patient studies. It is necessary to confirm these findings in real clinical settings.. References 1 Hobbs WR, Rall TW, Verdoorn TA. Hypnotics and sedatives; Ethanol. In: Hardman JG, Limbird LE, Molinoff PB, Ruddon RW, eds. Goodman and Gilman’s the Pharmacological Basis of Therapeutics, 9th Edn. New York: McGraw-Hill, 1996; 361–96 2 Burns AM, Shelly MP, Park GR. The use of sedative agents in critically ill patients. Drugs 1992; 43: 507–15 3 Ritz R. Benzodiazepine sedation in adult ICU patients. Intensive Care Med 1991; 17 (Suppl. 1): 11–14 4 Bauer TM, Ritz R, Haberthu¨ r C, et al. Prolonged sedation due to accumulation of conjugated metabolites of midazolam. Lancet 1995; 346: 145–7 5 Saul JP, Berger RD, Albrecht P, Stein SP, Chen MH, Cohen RJ. Transfer function analysis of the circulation: unique insight into cardiovascular regulation. Am J Physiol 1991; 261: H1231–45. 6 Robbe HWJ, Mulder LJM, Ru¨ ddel H, Langewitz W, Veldman JBP, Mulder G. Assessment of baroreceptor reflex sensitivity by means of spectral analysis. Hypertension 1987; 10: 538–43 7 Ha HR, Rentsch KM, Kneer J, Vonderschmitt DJ. Determination of midazolam and its alpha-hydroxy metabolite in human plasma and urine by high-performance liquid chromatography. Ther Drug Monit 1993; 15: 338–43 8 Parati G, Casadei R, Groppelli A, Di Rienzo M. Comparison of finger and intra-arterial blood pressure monitoring at rest and during laboratory testing. Hypertension 1989; 13: 647–55 9 Mulder LJM, van Dellen HJ, van der Meulen P, Opheikens B. A spectral analysis program for cardiovascular time series. In: Maarse FJ, Mulder LJM, Sjouw W, Akkerman A, eds. Computers in Psychology: Methods, Instrumentation and Psychodiagnostics. Amsterdam: Swets and Zeitlinger, 1988; 30–38 10 Rompelman O, Snijders JB, van Spronsen CJ. The measurement of heart rate variability spectra with the help of a personal computer. IEEE Trans Biomed Eng 1982; 29: 503–10 11 van Dellen HJ, Aasman J, Mulder LJM, Mulder G. Time domain versus frequency domain measures of heart rate variability. In: Orlebeke JF, Mulder G, van Doornen LJP, eds. Psychophysiology of Cardiovascular Control. New York: Plenum Press, 1985; 233–48 12 Scha¨ chinger H, Langewitz W, Ru¨ ddel H, et al. Spectral measures of short-term blood pressure and heart rate variations: Methodological considerations. Homeostasis 1996; 37: 97–105 13 Haberthu¨ r C, Scha¨ chinger H, Langewitz W, Ritz R. Effect of beta blockade with and without sympathomimetic activity (ISA) on sympathovagal balance and baroreflex sensitivity. Clin Physiol 1999; 19: 143–52 14 Ramsay MAE, Savege TM, Simpson BRJ, Goodwin R. Controlled sedation with alphaxalone–alphadalone. BMJ 1974; 2: 656–9 15 Stevens J. Applied Multivariate Statistics for the Social Sciences, 3rd Edn. New Jersey: Lawrence Erlbaum Associates, 1996 16 de Boer RW, Karemaker JM, Strackee J. Hemodynamic fluctuations and baroreflex sensitivity in humans: a beat-to-beat model. Am J Physiol 1987; 253: H680–9 17 de Boer RW, Karemaker JM, Strackee J. Comparing spectra of a series of point events particularly for heart rate variability data. IEEE Trans Biomed Eng 1984; 31: 384–7 18 Pitzalis MV, Mastropasqua F, Passantino A, et al. Comparison between noninvasive indices of baroreceptor sensitivity and the phenylephrine method in post-myocardial infarction patients. Circulation 1998; 97: 1362–7 19 James MA, Panerai RB, Potter JF. Applicability of new techniques in the assessment of arterial baroreflex sensitivity in the elderly: a comparison with established pharmacological methods. Clin Sci 1998; 94: 245–53 20 Watkins LL, Fainman C, Dimsdale J, Ziegler MG. Assessment of baroreflex control from beat-to-beat blood pressure and heart rate changes: a validation study. Psychophysiology 1995; 32: 411–14 21 Watkins L, Grossman P, Sherwood A. Noninvasive assessment of baroreflex control in borderline hypertension. Comparison with the phenylephrine method. Hypertension 1996; 28: 238–43 22 Maestri R, Pinna GD, Mortara A, La Rovere MT, Tavazzi L. Assessing baroreflex sensitivity in post-myocardial infarction patients: comparison of spectral and phenylephrine techniques. J Am Coll Cardiol 1998; 31: 344–51 23 Lord SW, Clayton RH, Hall MC, et al. Reproducibility of three different methods of measuring baroreflex sensitivity in normal subjects. Clin Sci 1998; 95: 575–81 24 Stauss HM, Anderson EA, Haynes WG, Kregel KC. Frequency response characteristic of sympathetically mediated vasomotor waves in humans. Am J Physiol 1998; 274: H1277–83. 321.
(7) Midazolam effect on cardiovascular transfer function. 25 Sakomoto M, Yasumoto, Oshumi H, Choi H, Shibata Y, Kano T. Effects of midazolam and flumazenil on carotid sinus baroreflex control of circulation in rabbits. Br J Anaesth 1994; 73: 384–7 26 DiMicco JA. Evidence for control of vagal tone by benzodiazepine receptors. Neuropharmacology 1987; 26: 553–9 27 DiMicco JA. Blockade of forebrain gamma-aminobutyric acid (GABA) receptors and reflex activation of the cardiac vagus in anesthetized cats. J Pharmacol Exp Ther 1982; 223: 654–61 28 Conahan ST, Vogel WH. The effect of diazepam administration on heart rate and mean arterial blood pressure in resting and stressed conscious rats. Res Commun Chem Pathol Pharmacol 1986; 53: 301–17 29 Gerold M, Cavero I, Riggenbach H, Wall M, Haeusler G. Analysis of cardiac chronotropic responses to diazepam and bromazepam in conscious trained dogs. Eur J Pharmacol 1976; 35: 361–8 30 Yang CC, Kuo TB, Chan SH. Auto- and cross-spectral analysis of cardiovascular fluctuations during pentobarbital anesthesia in the rat. Am J Physiol 1996; 270: H575–82 31 Berntson GG, Hart S, Sarter M. The cardiovascular startle response: anxiety and the benzodiazepine receptor complex. Psychophysiology 1997; 34: 348–57 32 Smyth HS, Sleight P, Pickering GW. Reflex regulation of arterial pressure during sleep in man. A quantitative method of assessing baroreflex sensitivity. Circ Res 1969; 24: 109–21. 33 Marty J, Gauzit R, Lefevre P, et al. Effects of diazepam and midazolam on baroreflex control of heart rate and on sympathetic activity in humans. Anesth Analgesia 1986; 65: 113–19 34 Conway J, Boon N, Jones JV, Sleight P. Involvement of the baroreceptor reflexes in the changes in blood pressure with sleep and mental arousal. Hypertension 1983; 5: 746–8 35 Pomfrett CJD, Barrie JR, Healy TEF. Respiratory sinus arrhythmia: an index of light anaesthesia. Br J Anaesth 1993; 71: 212–17 36 Haberthu¨ r C, Lehmann F, Ritz R. Assessment of depth of midazolam sedation using objective parameters. Intensive Care Med 1996; 22: 1385–90 37 Galletly DC, Williams TB, Robinson BJ. Periodic cardiovascular and ventilatory activity during midazolam sedation. Br J Anaesth 1996; 76: 503–7 38 Feshchenko VA, Veselis RA, Reinsel RA. Comparison of the EEG effects of midazolam, thiopental, and propofol: The role of underlying oscillatory systems. Neuropsychobiology 1997; 35: 211–20 39 Bu¨ hrer M, Maitre PO, Hung O, Stanski DR. Electroencephalographic effects of benzodiazepines: choosing an electroencephalographic parameter to measure the effect of midazolam on the central nervous system. Clin Pharmacol Ther 1990; 48: 544–54. 322.
(8)
Figure


Documents relatifs