ContentslistsavailableatScienceDirect
Resuscitation
j o ur na l h o me pa g e:ww w . e l s e v i e r . c o m / l o c a t e / r e s u s c i t a t i o n
Clinical
paper
Prehospital
cooling
to
improve
successful
targeted
temperature
management
after
cardiac
arrest:
A
randomized
controlled
trial
夽
D.C.
Scales
a,b,c,d,∗,
S.
Cheskes
e,f,
P.R.
Verbeek
e,f,
R.
Pinto
a,
D.
Austin
g,
S.C.
Brooks
h,i,
K.N.
Dainty
c,i,
K.
Goncharenko
i,
M.
Mamdani
j,
K.E.
Thorpe
j,k,
L.J.
Morrison
c,e,i,
on
behalf
of
the
Strategies
for
Post-Arrest
Care
SPARC
Network
aDepartmentofCriticalCareMedicine,SunnybrookHealthSciencesCentre,Toronto,Ontario,Canada
bInterdepartmentalDivisionofCriticalCare,DepartmentofMedicine,UniversityofToronto,Toronto,Ontario,Canada cInstituteforHealthPolicy,ManagementandEvaluation,UniversityofToronto,Toronto,Ontario,Canada
dInstituteofClinicalandEvaluativeSciences,Toronto,Ontario,Canada
eDivisionofEmergencyMedicine,DepartmentofMedicine,UniversityofToronto,Toronto,Ontario,Canada fSunnybrookCentreforPrehospitalMedicine,SunnybrookHealthSciencesCentre,Toronto,Ontario,Canada gDepartmentofEmergencyMedicine,MarkhamStouffvilleHospital,Markham,Ontario,Canada
hDepartmentofEmergencyMedicine,FacultyofHealthSciencesQueen’sUniversity,Kingston,Ontario,Canada iRescu,LiKaShingKnowledgeInstitute,St.Michael’sHospital,Toronto,Ontario,Canada
jAppliedHealthResearchCentre,LiKaShingKnowledgeInstitute,St.Michael’sHospital,Toronto,Ontario,Canada kDallaLanaSchoolofPublicHealth,UniversityofToronto,Toronto,Ontario,Canada
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:Received16May2017 Receivedinrevisedform 25September2017 Accepted2October2017 Keywords:
Targetedtemperaturemanagement Out-of-hospitalcardiacarrest Qualityimprovement Randomizedcontrolledtrial Knowledgetranslation Criticalcare
Prehospitalintervention Safety
a
b
s
t
r
a
c
t
Rationale:Targetedtemperaturemanagement(TTM)improvessurvivalwithgoodneurologicaloutcome
afterout-of-hospitalcardiacarrest(OHCA),butisdeliveredinconsistentlyandoftenwithdelay. Objective:Todetermineifprehospitalcoolingbyparamedicsleadstohigherratesof‘successfulTTM’, definedasachievingatargettemperatureof32–34◦Cwithin6hofhospitalarrival.
Methods:PragmaticRCTcomparingprehospitalcooling(surfaceicepacks,coldsalineinfusion,wristband reminders)initiated5minafterreturnofspontaneouscirculation(ROSC)versususualresuscitationand transport.Theprimaryoutcomewasrateof‘successfulTTM’;secondaryoutcomeswereratesofapplying
TTMinhospital,survivalwithgoodneurologicaloutcome,pulmonaryedemainemergencydepartment,
andre-arrestduringtransport.
Results:585patientswererandomizedtoreceiveprehospitalcooling(n=279)orcontrol(n=306). Pre-hospitalcoolingdidnotincreaseratesof‘successfulTTM’(30%vs25%;RR,1.17;95%confidenceinterval [CI]0.91–1.52;p=0.22),butincreasedratesofapplyingTTMinhospital(68%vs56%;RR,1.21;95%CI 1.07–1.37;p=0.003).Survivalwithgoodneurologicaloutcome(29%vs26%;RR,1.13,95%CI0.87–1.47; p=0.37)wassimilar.Prehospitalcoolingwasnotassociatedwithre-arrestduringtransport(7.5%vs8.2%; RR,0.94;95%CI0.54–1.63;p=0.83)butwasassociatedwithdecreasedincidenceofpulmonaryedemain emergencydepartment(12%vs18%;RR,0.66;95%CI0.44–0.99;p=0.04).
Conclusions:Prehospitalcoolinginitiated5minafterROSCdidnotincreaseratesofachievingatarget temperatureof32–34◦Cwithin6hofhospitalarrivalbutwassafeandincreasedapplicationofTTMin
hospital.
©2017TheAuthors.PublishedbyElsevierIrelandLtd.ThisisanopenaccessarticleundertheCC BY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Abbreviations: CI,confidenceinterval;CPR,cardiopulmonaryresuscitation;DSMC,DataSafetyandMonitoringCommittee;EMS,emergencymedicalservices;GCS, GlasgowComaScale;ILCOR,InternationalLiaisonCommitteeonResuscitation;MRS,ModifiedRankinScale;OHCA,out-of-hospitalcardiacarrest;RCT,randomizedcontrolled trial;ROSC,returnofspontaneouscirculation;RR,relativerisk;SPARCNetwork,StrategiesforPostArrestCareNetwork;TTM,targetedtemperaturemanagement.
夽 ASpanishtranslatedversionoftheabstractofthisarticleappearsasAppendixinthefinalonlineversionathttps://doi.org/10.1016/j.resuscitation.2017.10.002. ∗ Correspondingauthorat:DepartmentofCriticalCareMedicine,SunnybrookHealthSciencesCentre,2075BayviewAvenue,RoomD108,Toronto,ON,M4N-3M5,Canada.
E-mailaddress:[email protected](D.C.Scales). https://doi.org/10.1016/j.resuscitation.2017.10.002
0300-9572/©2017TheAuthors.PublishedbyElsevierIrelandLtd.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense( http://creativecommons.org/licenses/by-nc-nd/4.0/).
Background
Targeted temperature management applied after hospital arrival has been shown to improve survival with good neuro-logicoutcomeandisrecommendedforpatientsresuscitatedfrom out-of-hospitalcardiacarrest(OHCA)followingareturnof spon-taneouscirculation(ROSC)[1,2].Althoughitsmechanismis not completelyunderstood,areductionincorebodytemperaturelikely reducestheinflammatoryresponsethatoccursfollowing ischemia-reperfusioninjury,directlydiminishescellularinjury,andincreases cerebralneuronalhealingbyreducingcerebraloxygendemandand intracranialpressure[3].
TheAmericanHeartAssociation,InternationalLiaison Commit-teeonResuscitation,andotherinternationalagenciesnowstrongly recommendTTMforeligiblepatientsfollowingresuscitationfrom cardiacarrest[4,5].Despitetheserecommendations,TTMis deliv-ered inconsistently, incompletely, and often with delay [6–9]. Reasonscitedtoexplainthisincompleteadoptionincludelackof awarenessof recommendedpractice,perceptions of poor prog-nosis,limitedtimeandresources,andstaffingshortages[10–14]. Hospital-basedknowledgetranslation interventionsdesignedto increaseuseofTTMhavebeenonlymodestlysuccessful[15].
Wehypothesizedthatprehospitalcoolingbyemergency medi-calservices(EMS)providers(paramedics)couldactasacatalystto encouragemoretimelyapplicationofTTMbyin-hospitalclinicians, andthatearliercoolingmightalsoimproveclinicaloutcomes[16]. Wetestedthishypothesisbyconductinganopen-labelpragmatic randomizedcontrolledtrial(RCT)toanswerthefollowing ques-tion:Doesprehospitalcoolingusingsurfaceicepacks,infusionof intravenouscoldsaline,andapplicationofawristbandreminder –compared tonoprehospital cooling– leadtohigher rates of ‘successfulTTM’inOHCApatients,definedasachievingatarget temperatureof32–34◦Cwithin6hofhospitalarrival?(Initiation ofCoolingbyEmergencymedicalservicestoPromotetheAdoption
ofin-hospitaltherapeutichypothermiainCardiacarrestSurvivors,
theICEPACSRCT).
Methods
Participantsandsetting
The study was conducted by 4 large EMS systems (Halton ParamedicServices,PeelParamedicServices,TorontoParamedics Services,andYorkParamedicServices)servingtheGreaterToronto Areaand their24 receivinghospitalsin theStrategiesfor Post-ArrestCareNetwork [17]. Patientswereeligible iftheyhad an EMS-treatedOHCA;age≥18years;sustainedROSCof≥5minand hadsystolicbloodpressure≥100mmHg;andwereunresponsiveto verbalstimuliorrequiredendotrachealintubation.Patientswere ineligibleif theetiology of cardiac arrest wastrauma,burn, or exposurehypothermia;oriftheyhadclinicalevidenceofactive severebleeding,severesepsis,knowncoagulopathy,known do-not-resuscitate(DNR)order,knownpregnancy,orprisonerstatus. Randomization
We randomized (1:1) eligible patients into 2 groups using sequential,numbered,opaque,sealedenvelopesandvariable(4–6) blocksizes[18].Thisapproachhasbeenshowntobean accept-ablemethodformaintainingallocationconcealment,andhasbeen successfullyusedinthepastbyparticipatingEMSsystems[19,20]. Studyintervention
AmbulancesinparticipatingEMSsystemswerestockedatthe beginningofeach12-hparamedicshiftwithacoolercontaining
coldsalineandicepacks[22,23].Patientsrandomizedtoreceive prehospitalcoolinghadicepacksappliedtotheirneck,axillae,and bothgroinsandinfusionofupto2Lofcoldsaline(0.9%sodium chloridesolutionatapproximately4◦C)viaapressureinfusionbag andstandardintravenouslineduringtransporttohospital.Patients weregivenasingledoseofmidazolam5mg,andaseconddose (maximum10mg)ifneededtopreventshivering.Theparamedics fastenedawristbandtothepatientwiththefollowingmessage: “CardiacArrest Survivor – TherapeuticHypothermia Initiated– ConsiderContinuationofCooling”.Patientsrandomizedtothe con-trolarmreceivedconventionalpost-resuscitativesupportivecare butnoprehospitalcoolingorwristbandreminders.
Inbothstudygroups,allin-hospitalproceduresincludingthe applicationofTTMwerelefttothediscretionofthetreating clin-icalteam.Alldestinationhospitalswereinvolvedinourprevious implementationstudy,theStrategiesforPost-ArrestCare(SPARC) steppedwedgeclusterRCT[15].Thispreviousstudyensuredthat allhospitalshadimplementedprotocolsandordersetsfor deliv-eringtargetedtemperaturemanagement,typicallyusingsurface coolingmeasures,intheemergencydepartmentandincoronary careunitsandintensivecareunits.
Datacollection
AllconsecutiveOHCApatientswhoweretreatedby participat-ingEMS systemsand transported toa participatingdestination hospitalwereidentifiedandenteredintoaregionalclinicalregistry calledRescuEpistry[21,22].RescuEpistryisaweb-baseddata man-agementinterfacethatlinkselectronicambulancecallreportdata fromEMSsystemsandFireServiceswithin-hospitaldatato iden-tifyallOHCApatientsintheCityofTorontoandadjacentregions (Halton,Peel,Simcoe,Muskoka,Toronto,York,andDurham).Rescu Epistryincorporatescomprehensiveandautomatedsearchingof EMSrecordsthatresultsinnegligibleratesofmissedcases.Trained dataabstractorsblindedtotreatmentallocationcollectin-hospital datafromtheseOHCApatients,includingelementsofin-hospital post-arrestcare, and clinicaloutcomesuntil hospitaldischarge. Thesedataareenteredmanuallywithpointofentrylogicanderror checkstominimizeerrors.Duplicatedataabstractionoccursona randomsampleof10%ofabstractedchartsforeachin-hospitaldata collector[22].
Outcomes
Theprimaryoutcomewas‘successfulTTM’,definedasachieving atargettemperatureof32–34◦Cwithin6hofemergency depart-ment(ED)arrival[15].Secondaryoutcomesincludedratesof(ever) applyingTTMin-hospital;survivaltohospitaldischargewithgood neurologicaloutcome,definedasascoreof0,1,or2onthe Mod-ifiedRankinScale[23];survivalto6handtohospitaldischarge; re-arrestduringtransport tohospital;pulmonaryedema identi-fiedintheED;firsttemperaturerecordedin-hospital;andtimeto achievetargettemperatureamongpatientseverreachingtarget temperature.
Analyses
We summarized baseline characteristics using descriptive statistics.Theprimaryoutcomeandallsecondaryoutcomeswere analysedaccountingforthestratifiedrandomization(byEMS sys-tem)[24];allrelativeriskscomparingdichotomousvariableswere estimatedusingmodifiedPoissonregressionwithrobuststandard errorandfixedeffectsfortheEMSsystem.Ratesofsurvivaland survivalwithgoodneurologicaloutcomewerealsocomparedafter adjustmentforage,sex,EMSsystem,andshockablerhythm [ven-triculartachycardia (VT)or ventricularfibrillation(VF)vsother
rhythm][25].Weusedt-teststocomparetotalfluidinfusedand firsttemperaturerecordedinEDandWilcoxonrank-sumteststo comparetimestoachievesuccessfulTTM.ScoresontheModified RankinScaleathospitaldischargewerecomparedusingFisher’s exacttest.
Samplesizeestimate
Duringthe28monthsofourSPARCin-hospitalhypothermia study,therewere4399OHCApatientswhoweretreatedbyEMS systemsin participatingregions and1737(40%) achievedROSC [15].Ofthese,934(22%)survivedtransporttohospitalandwere deemedeligibleforTTM.Basedontheserates,weanticipatedthat paramedicswouldscreenapproximately4000patientsafterOHCA duringtheICEPACStrialandapproximately900eligiblepatients wouldberandomizedandalsosurvivetohospitaladmission.This samplesizewouldprovidesufficient(>80%)powertodetecta30% relativeimprovementintheprimaryoutcomeof‘successfulTTM’ fromabaselineeventrateof30%(i.e.anabsoluteincreaseto39%). Thissamplesize wouldalsoprovidesufficient power(>80%)to detectabsoluteimprovementsfrom20%to28%inratesofsurvival withgoodneurologicaloutcome.
Interimanalyses
Weplannedtoconduct2interimanalysesafterrandomization ofone-third(n=300)andtwo-thirds(n=600)ofthetotalsample size.Thetrialcouldbestoppedearlyforharmaccordingtothe earlystoppingcriteriaofHaybittle-Petoatasignificancelevelof p<0.001,fordifferencesineitherofthefollowing2pre-specified endpoints:mortalityduringtransporttohospitalandsurvivalwith goodneurologicaloutcomeathospitaldischarge[26].
Atthefirstscheduledinterimanalysisafterenrolmentof315 patients,itwasdeterminedthatthetrialwasunlikelytoachieve theplannedsamplesizeof900patientsduetolowerthanexpected recruitment rates. The Data Safety and Monitoring Committee (DSMC)recommendedthatenrolmentshouldcontinueuntilthe studyoperatingfunds weredepleted(revisedfinal samplesize, approximately500patients).Whenmakingthisrecommendation, theDSMCalsoconsideredtheimpactof2studiesthatwere pub-lishedafterthelaunchoftheICEPACSRCT.ThefirstwasaRCTof prehospitalcoolingforpatientswithOHCA,whichdetectedno sur-vivalbenefitbutahigherre-arrestrateassociatedwithprehospital cooling[27].However,attheinterimanalysis,noexcessinre-arrest rateswasobservedforeithergroupintheICEPACStrial.The sec-ondstudywasaRCTthatshowedsimilarclinicaloutcomeswhen in-hospitalTTMwasappliedtoachieveeitheratargettemperature of33◦Cor36◦C[28],raisingtheconcernthattheprimaryoutcome of‘successfulTTM’(i.e.achievingatargettemperatureof32–34◦C within6hofEDarrival)couldbecomeinfeasible.TheDSMCnoted, however,thatprehospitalcoolingmightstillaffectclinically impor-tantsecondaryendpoints,forexampleratesof(ever)applyingTTM in-hospitalorsurvivalwithgoodneurologicaloutcomeathospital dischargeandsafetyendpointsofpulmonaryedemaorre-arrest. Patientinvolvement
Patientswerenotinvolvedinthedevelopmentoftheresearch questionorthedesignofthisRCT.
Ethics
Thetrialwasreviewedand approvedbytheResearch Ethics BoardsofSunnybrookHealthSciencesCentreandLakeridgeHealth and wasconducted under exception from informedconsent in
emergencyresearch.Allenrolledpatients(ortheirsurviving rela-tives)weresentaletterofnotificationthatexplainedtheirinclusion inthetrialusingawaiverofconsent.Theresearchethicsboardsof allparticipatingdestinationhospitalsapprovedthenecessarychart reviewstoobtainrelevantclinicaloutcomesforthetrial.Thetrial wasregisteredwiththeU.S.NationalInstitutesofHealth (Clinical-Trials.govNCT01528475).
Results
Patientsandmeasurements
BetweenJuly 3,2012and Jan8,2016,17,940 patientswere treated byparticipatingEMSsystems, and3312 achievedROSC (Fig. 1). Of these, 700 patients satisfied eligibility criteria and 585wererandomized.Eligiblebutnon-randomizedpatientswere youngerandhadshortertransporttimes,butwereotherwise sim-ilartorandomizedpatients(TableA1inSupplementarymaterial). Theidentityof3patientsinthecontrolgroupcouldnotbeobtained and thus could not be linked to hospital records, leaving 582 patientsforthefinalintention-to-treatanalysis(Table1).
Primaryoutcome
Ratesof‘successfulTTM’werenotincreasedamongpatients randomizedtoreceiveprehospitalcoolingcomparedtocontrols [85(30%)vs77(25%);RR1.17(95%CI0.91–1.52),p=0.22;Table2]. Similarresults wereobtainedin a sensitivity analysisthat was restrictedtotheperiodpriortothepublicationofthein-hospital TTMtrial(TableA2inSupplementarymaterial)[28].
Secondaryoutcomes
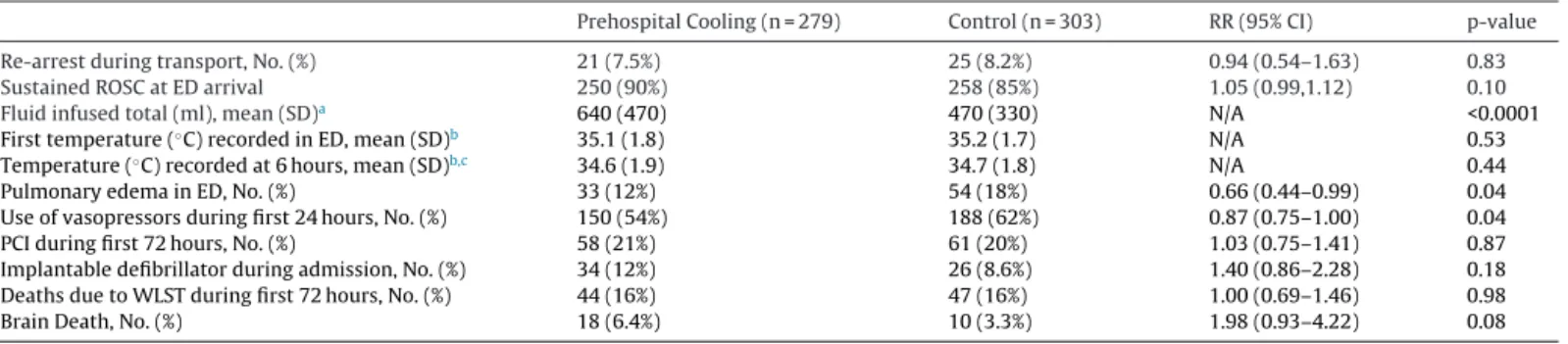
Patientsintheprehospitalcoolinggroupweremorelikelyto (ever)receiveTTMinhospital[190(68%)vs170(56%);RR1.21, p=0.003] than patientsin the control group. Rates of survival to hospital discharge and survival with good neurological out-comesweresimilarinbothgroups(Table2andFig.2),evenafter adjustingforage,sex,presenceofashockablerhythm,andEMS system[survivaltohospitaldischarge,RR1.01(95%CI0.83–1.23), p=0.93;survivalwithgoodneurologicaloutcomesRR1.11(95%CI 0.88–1.39),p=0.38].Noincreaseinratesofre-arrestduring trans-port[7.5%vs8.2%;RR0.94(95%CI0.54–1.63),p=0.83]wasobserved among patientsreceivingprehospital cooling,and rates of pul-monaryedemainEDwerelowerthanincontrolpatients[12%vs 18%,RR0.66(95%CI0.44–0.99),p=0.04;Table3].
Coolingprocessmeasures
Themajority(239,86%)ofpatientsrandomizedtoreceive pre-hospitalcoolingreceivedeithersurfacecoolingorinfusionofcold saline,butapplicationofboth wasnotconsistent(Table4).The meanvolumeoftotalfluidinfusedduringtransportwasgreaterin theprehospitalcoolinggroup(640vs470ml,p<0.0001),andthe meanvolumeofcoldsalineinfusedduringprehospitalcoolingwas 490ml(SD420ml).Threepatientsinthecontrolgroupreceived infusionsofcoldsalineasprotocolviolations.Thefirsttemperature measuredintheEDwasnotdifferentbetweengroups(35.1◦Cin patientsreceivingprehospitalcoolingvs35.2◦Cincontrolpatients, p=0.53;Table3).AmongpatientswhoeverreceivedTTMin hos-pital(andwhoeverreachedthetargettemperature),thetimeto achievethetargettemperaturewassimilarintheprehospital cool-inggroupversusthecontrolgroup[median(IQR)5.4h(3.0–8.2)vs 4.8h(2.8–7.7),p=0.45].
Fig.1.PatientFlow. Fig.1showsscreeningandenrolmentofpatientsduringthetrial.
Table1
CharacteristicsofPatients.
PatientCharacteristics PrehospitalCooling(n=279) Control(n=303)
Age–mean(SD) 68(15) 69(16)
Men,No.(%) 196(70%) 184(61%)
Publicarrest,No.(%) 61(22%) 66(22%)
Bystanderwitnessed,No.(%) 163(58%) 188(62%)
BystanderCPR,No.(%) 124(44%) 146(48%)
PADapplied,No.(%) 13(4.7%) 17(5.6%)
InitialrhythmVF/VT,No.(%) 124(45%) 134(44%)
Timefrom911calltoEMSarrival–mean(SD),minutes 6.0(2.6) 6.2(2.5)
TimefromEMSarrivaltoEDarrival–mean(SD),minutes 45(12) 46(12)
TimefromfirstROSCtoEDarrival–mean(SD),minutes 29(10) 29(11)
GCSscorerecordedpostROSC–mean(SD) 3.3(1.6) 3.3(1.4)
Systolicbloodpressurepre-randomization,mmHg(SD) 137(42) 138(42)
Comorbidities
CoronaryarterydiseaseorpreviousMI 44(16%) 34(11%)
Congestiveheartfailure 13(4.7%) 11(3.6%)
Previousaortocoronarybypasssurgery 20(7.2%) 13(4.3%)
Hypertension 103(37%) 126(42%)
Diabetes 55(20%) 66(22%)
Fromnursinghomeorlong-termcarefacility 10(3.6%) 15(5.0%)
Footnotes:
Abbreviations:TTM=TargetedTemperatureManagement;SD=standarddeviation;CPR=cardiopulmonaryresuscitation;PAD=publicaccessdefibrillator;VF=ventricular fibrillation;VT=ventriculartachycardia;EMS=EmergencyMedicalServices;ED=EmergencyDepartment;ROSC=ReturnofSpontaneousCirculation;GCS=GlasgowComa Scale;mmHg=millimetersofMercury;MI=myocardialinfarction.
Table2
Outcomes.
PrehospitalCooling(n=279) Control(n=303) RR(95%CI) p-value
TTMreaching32–34◦Cwithin6hours,No.(%) 85(30%) 77(25%) 1.17(0.91–1.52) 0.22
TTMappliedinhospital(ever),No.(%) 190(68%) 170(56%) 1.21(1.07–1.37) 0.003
Survivaltohospitaldischarge,No.(%)b 92(33%) 98(32%) 1.02(0.81–1.29) 0.88
Survivalto6hoursafterEDadmission,No.(%) 223(80%) 233(77%) 1.15(0.84–1.56) 0.39
Survivaltohospitaldischarge–patientspresentingwithVT/VF,No.(%) 79(64%) 74(55%) 1.16(0.95–1.41) 0.16 Goodneurologicaloutcomeaathospitaldischarge,No.(%)b 82(29%) 76(26%) 1.13(0.87–1.47) 0.37
Neurologicalstatusatdischargeb,c 0.77
Nosymptoms(mRS0),No.(%) 46(16%) 45(15%)
Nosignificantdisability(mRS1),No.(%) 26(9.3%) 23(7.8%)
Slightdisability(mRS2),No.(%) 10(3.6%) 8(2.7%)
Moderatedisability(mRS3),No.(%) 4(1.4%) 4(1.4%)
Moderatelyseveredisability(mRS4),No.(%) 1(0.4%) 5(1.7%)
Severedisability(mRS5),No.(%) 5(1.8%) 5(1.7%)
Dead(mRS6),No.(%) 187(67%) 205(69%)
Footnotes:
Abbreviations:RR=RelativeRisk;CI=confidenceinterval;TTM=TargetedTemperatureManagement;ROSC=returnofspontaneouscirculation;VT/VF=pulselessventricular tachycardia/ventricularfibrillation;mRS=ModifiedRankinScale
aGoodneurologicaloutcomedefinedasascoreof0,1,or2ontheModifiedRankinScale.
bNeurologicalstatusathospitaldischargecouldnotbeobtainedfor8(2.6%)ofpatientsinthecontrolgroupandvitalstatusathospitaldischargecouldnotbeobtained for1patient(0.3%)inthecontrolgroup.
c p-valuebasedonFisher’sexacttestofscoresontheModifiedRankinScalebytreatmentassignment.
Fig.2. NeurologicalOutcomesatHospitalDischarge.
Fig.2showsdistributionofpatients’neurologicaloutcomesathospitaldischargebytreatmentgroupaccordingtoModifiedRankinScale.
Table3
PrehospitalandIn-hospitalProcessData.
PrehospitalCooling(n=279) Control(n=303) RR(95%CI) p-value
Re-arrestduringtransport,No.(%) 21(7.5%) 25(8.2%) 0.94(0.54–1.63) 0.83
SustainedROSCatEDarrival 250(90%) 258(85%) 1.05(0.99,1.12) 0.10
Fluidinfusedtotal(ml),mean(SD)a 640(470) 470(330) N/A <0.0001
Firsttemperature(◦C)recordedinED,mean(SD)b 35.1(1.8) 35.2(1.7) N/A 0.53
Temperature(◦C)recordedat6hours,mean(SD)b,c 34.6(1.9) 34.7(1.8) N/A 0.44
PulmonaryedemainED,No.(%) 33(12%) 54(18%) 0.66(0.44–0.99) 0.04
Useofvasopressorsduringfirst24hours,No.(%) 150(54%) 188(62%) 0.87(0.75–1.00) 0.04
PCIduringfirst72hours,No.(%) 58(21%) 61(20%) 1.03(0.75–1.41) 0.87
Implantabledefibrillatorduringadmission,No.(%) 34(12%) 26(8.6%) 1.40(0.86–2.28) 0.18
DeathsduetoWLSTduringfirst72hours,No.(%) 44(16%) 47(16%) 1.00(0.69–1.46) 0.98
BrainDeath,No.(%) 18(6.4%) 10(3.3%) 1.98(0.93–4.22) 0.08
Footnotes:
Abbreviations:TTM=TargetedTemperatureManagement;RR=RelativeRisk;CI=confidenceinterval;IQR=interquartilerange;SD=StandardDeviation;ED=Emergency Department;◦C=◦Celsius;PCI=percutaneouscoronaryintervention;WLST=withdrawaloflife-sustainingtherapy;N/A=Notapplicable
aTotalfluidinfusedwasnotdocumentedfor98(35%)patientswhoreceivedPrehospitalCoolingand121(40%)controlpatients. bNotemperaturemeasurementwasrecordedfor58(21%)patientswhoreceivedPrehospitalCoolingand60(20%)controlpatients. c Referstolasttemperaturerecordedinchartpriorto6h.
Discussion
WeconductedapragmaticRCTinalargemetropolitanareato compareprehospitalcoolingbyparamedicsofpatientsresuscitated
afterOHCA,tousualcarewithnoTTMapplieduntilhospital.The mainhypothesiswasthataprehospitalcoolingbundleincluding
Table4
PrehospitalCooling.
PrehospitalCooling(n=279)
Anyprehospitalcoolingdocumented 239(86%)
Coldice-packsapplied,No.(%) 186(67%)
Coldfluidinfused,No(%) 201(72%)
Coldfluidinfusedtotal(ml),mean(SD)a 490(420)
Footnotes:
Abbreviations:RR=RelativeRisk;CI=confidenceinterval;SD=StandardDeviation. aTotalvolumeofcoldfluidinfusedwasnotdocumentedfor79(28%)ofpatients intheprehospitalcoolinggroup.
surfaceicepacks,infusionofcoldsaline,andwristbandreminders wouldpromotemoreefficientuseofin-hospitalTTM,bystarting thecoolingprocessearlierandactingasapowerfulreminderto in-hospitalclinicians.Theprimaryoutcomeof‘successfulTTM’– achievingatargettemperatureoflessthan34◦Cwithin6hofED arrival–wasnotsignificantlydifferentcomparinggroups. How-ever,prehospitalcoolingresultedinincreasedapplication(ever) ofin-hospitalTTMcomparedtocontrols(68%vs56%,p=0.003). Thisfindingconfirmsthehypothesisthataprehospitalintervention candirectlyinfluencetheapplicationofevidence-based recom-mendationsbyin-hospitalclinicians,assuggestedbyobservational research[29].
Mostprevioustrialsexaminingprehospitalcoolinghavebeen smallsingle-centredRCTsorfeasibilitystudies[30,31].However, twootherlargetrialsofprehospitalcoolinghavebeenpublished. ARCTconductedbytheEMSsysteminSeattlerandomized1359 patientstoreceiveusualcareorprehospitalcoolinginitiated imme-diatelyafterROSCbyinfusionofcoldintravenoussaline(75%of patientsreceived≥1l),7–10mgofintravenouspancuronium,and 1–2mgofintravenousdiazepam[27].Thetrialshowedno differ-enceintheprimaryoutcomesofsurvivalandneurologicalstatus athospitaldischarge,butdetectedmoreepisodesofre-arrest(26% vs21%)andpulmonaryedemaonfirstchestx-ray(41%vs30%) among patientsin theprehospital cooling group.A recent RCT fromAustraliarandomized1198patientstousualcareor prehos-pitalcoolingbyinfusionofupto2Lofcoldsaline(mean1193ml) initiatedduringthedeliveryofCPR [32].Thistrialwasstopped earlyduetoconcernsthatTTMmanagementinreceiving hospi-talshad changedfollowingpublication oftheNielsenTTMtrial [28];nodifferenceswereobservedintheprimaryoutcomeof sur-vivalathospitaldischarge.However,ROSCwaslessfrequentamong patientsreceivingprehospitalcoolingcomparedtocontrolpatients (41%vs51%).Together,these2largetrialssuggestedthatcooling duringresuscitationorimmediatelyfollowingROSCmaybe harm-ful.Incontrast,ourtrialdetectednoexcessofadverseeventswhen prehospitalcoolingwasdelayeduntil5minaftersuccessfulROSC. Weintentionallydelayedtheinitiationofprehospitalcoolinginour trialtoreducetheriskofre-arrest,whichoccursmostfrequentlyin theminutesimmediatelyfollowingROSC[33,34].Patients random-izedtoprehospitalcoolinginourRCTalsoreceivedlessintravenous coldsalineduringtransportthanwasadministeredintheseother trials,whichmayhavefurtherdecreasedthepotentialfor prehos-pitalcoolingtoinducerecurrentarrhythmiasorpulmonaryedema. Ourtrialhasseverallimitations.Thetrialdidnotachievethe anticipatedsamplesizeduetoslowerthanexpectedenrolment, andmayhavebeenunderpoweredtodetectsmallbutclinically importantdifferencesinprimaryorsecondaryoutcomes.Notall eligiblepatientswereenrolledbyparticipatingparamedics,and thismayaffectthegeneralizabilityofourfindings.Themainreason for not randomizing 16% of eligible patientswas that individ-ualparamedics declinedtoparticipatein research.Randomized patientshadslightlylongertransporttimesandyoungerage,but wereotherwisesimilartoeligiblebutnon-randomizedpatients withnoclearevidenceofsamplingbias.Ourprimaryoutcomeof
‘successfulTTM’–achievingatargettemperatureof32–34◦C–was chosenasafeasibleprocessendpointthatwouldcapturemore effi-cientandtimelydeliveryofTTM.However,itremainsunknown whetherachievingatargettemperaturesoonerisassociatedwith improvedoutcomesaftercardiacarrest[35].Theoptimalendpoint forprehospitaltrialsremainsatopicofdebate[36,37].In partic-ular,strivingtomeasureplausibleincreasesinratesofsurvivalto hospitaldischargemayrequireenormoussamplesizes[38,39].Our primaryoutcomedirectlymeasuredtheeffectivenessof prehospi-talcoolingasanimplementationstrategy,butalternateendpoints thatcouldbeconsideredinfutureresearchincludeimproving phys-iology,limiting disability,alleviatingdiscomfort, and improving patientsatisfaction[40].
Thepublicationofthein-hospitalTTMtrialin2013mayalso havecausedmanyclinicianstoonlytargetatemperatureof36◦C aftercardiacarrest, makingourprimaryoutcome of‘successful TTM’–coolingtoatargetof32–34◦C–lessrelevant.However, theresultsofourprimaryoutcomecomparisonwereunchanged whenanalyseswererestrictedtotheperiodpriortothe publica-tionoftheTTMtrial.Nevertheless,prehospital coolingwasstill associatedwithhigherratesofapplyingin-hospitalTTMoverall, confirmingthehypothesisthatprehospitaltreatmentdecisionscan influencedeliveryofrecommendedpracticesinreceiving hospi-tals.Ourtrialevaluatedtheeffectivenessofaprehospitalcooling bundlethatincludedintravenouscoldfluids,surfaceicepacks,and wristbandreminders;weareunabletodeterminewhich compo-nentofthisbundlewasmosteffectiveatinfluencingin-hospital clinicianbehavior.Patientsrandomizedtoreceiveprehospital cool-inghadthisinterventionincompletelydelivered;onlytwo-thirds ofpatientshadcoldicepacks appliedand aboutthree-quarters receivedinfusionsofcoldsaline.Despitetheuseofpressure infu-sionbags,themeanvolumeofcoldfluidinfusedwasonly490ml, suggesting thattransport timesmaynot have beensufficiently longtofacilitateeffectiveintravenouscooling,orthatthesaline for infusionwasnotuniformly maintainedat4◦C while stored inthecooler.Thislikelyexplainswhyinitialtemperatures mea-suredinEDsweresimilarcomparinggroups,butmayalsoexplain theapparentsafetyofourprotocolcomparedtootherstudiesof prehospitalcooling.
Conclusion
In conclusion, prehospitalcooling initiated 5minafter ROSC didnotleadtohigherratesofachievingatargettemperatureof 32–34◦Cwithin6hofhospitaladmissionafterOHCA,butwassafe andincreasedtheapplicationofTTMinhospital.
Transparencydeclaration
DamonScalesaffirmsthatthemanuscriptisanhonest, accu-rate,andtransparentaccountofthestudybeingreported;thatno importantaspectsofthestudyhavebeenomitted;andthatany dis-crepanciesfromthestudyasplanned(and,ifrelevant,registered) havebeenexplained.RuxandraPintoandDamonScaleshadfull accesstoallofthedatainthestudyandtakeresponsibilityforthe integrityofthedataandtheaccuracyofthedataanalysis.
Authors’contribution
ConceptionofStudy:DCS
DesignofStudy:DCS,SCB,SC,KND,MM,KET,PRV,LJM Implementation:DCS,DA,SC,KG,PRV,LJM
AnalyticalPlan/Analyses:DCS,RP DraftingofManuscript:DCS
EditingofManuscriptforintellectualcontent:DCS,DA,SDB,SC, KND,KG,RP,MM,KET,PRV,LJM.
Sourceoffunding
Thistrial(InitiationofCoolingbyEmergencymedicalservices toPromotetheAdoptionofin-hospitaltherapeutichypothermiain
CardiacarrestSurvivors,theICEPACSRCT)wasfundedbyagrant fromtheCanadianInstituteofHealthResearch.Dr.Scaleswasthe recipientoftheGrahamFarquharsonKnowledgeTranslation Fel-lowshipfromthePhysiciansServicesIncorporatedFoundation.Dr. MorrisonholdstheRobertandDorothyPittsChairinAcuteCareand EmergencyMedicine,LiKaShingKnowledgeInstitute,StMichael’s Hospital,UniversityofToronto.TheSPARCNetworkisalsofunded byaCenterforResuscitationScienceandKnowledgeTranslation grantfromtheLaerdalFoundationforAcuteMedicine–Centre Sup-portProgramandagrantfromtheHeartandStrokeFoundationof CanadaandCanadianInstituteofHealthResearch.
Conflictsofinterest
S.C.receivedspeakinghonorariafromZollMedicalCorporation andPhysio-ControlCorporationforprovidingeducationaltalkson CPRquality.
StrategiesforPostArrestCare–ICEPACSnetwork participatinginstitutions(www.sparcnetwork.ca)
1.Halton Healthcare – Georgetown Hospital, Georgetown, Ontario,Canada
2.HaltonHealthcare–MiltonDistrictHospital,Milton,Ontario, Canada
3.Halton Healthcare – Oakville Trafalgar Memorial Hospital, Oakville,Ontario,Canada
4.HumberRiverHospital–ChurchSite,York,Ontario,Canada 5.HumberRiverHospital–FinchSite,York,Ontario,Canada 6.JosephBrantHospital,Burlington,Ontario,Canada 7.LakeridgeHealth–Oshawa,Oshawa,Ontario,Canada 8.MackenzieHealth,RichmondHill,Ontario,Canada 9.MarkhamStouffvilleHospital,Markham,Ontario,Canada 10.MichaelGarronHospital,Toronto,Ontario,Canada 11.MountSinaiHospital,Toronto,Ontario,Canada 12.NorthYorkGeneralHospital,Toronto,Ontario,Canada 13.Rouge Valley Health System– CentenarySite, Scarborough,
Ontario,Canada
14.RoyalVictoriaRegionalHealthCentre,Barrie,Ontario,Canada 15.The Scarborough Hospital – General Campus, Scarborough,
Ontario,Canada
16.St.Joseph’sHealthCentre,Toronto,Ontario,Canada 17.St.Michael’sHospital,Toronto,Ontario,Canada
18.SunnybrookHealthSciencesCentre,Toronto,Ontario,Canada 19.TrilliumHealthPartners–CreditValleyHospital,Mississauga,
Ontario,Canada
20.TrilliumHealthPartners–MississaugaHospital,Mississauga, Ontario,Canada
21.University Health Network – Toronto General Hospital, Toronto,Ontario,Canada
22.University Health Network – Toronto Western Hospital, Toronto,Ontario,Canada
23.William Osler Health System – Brampton Civic Hospital, Brampton,Ontario,Canada
24.WilliamOslerHealthSystem–EtobicokeGeneralHospital, Eto-bicoke,Ontario,Canada
ICEPACSparticipatingemergencymedicalservices
HaltonParamedicServices PeelRegionalParamedicServices TorontoParamedicServices YorkParamedicServices
Acknowledgements
Michelle Gaudio, Kate Byrne, Aarthi Kamath, and Toula Gonadellesfortrialsupport;SedighehShaeriforrecordreviews; CathyZhanfordataanalysisandAdamByersfordatamanagement. Alloftheaforementionedindividualsweresalariedemployeeson thegrant.
ForoperationalandimplementationsupportateachEMS sys-tem:TorontoParamedicServices:ChiefPaulRaftis,GaryMcauley, DeputyChiefGarrieWright,ErinRoyal,RachelEdwards,Kris Sta-ley,ScottGorsline,AlanCraig;PeelParamedicServices:ChiefPeter Dundas,PriyaKakar,GordonNevels;HaltonParamedicServices: ChiefGregSage,RomanNowickyj;YorkParamedicServices:Chief Norm Barrette, Deputy Chief Chris Spearen, Natalie Kedzierski, SteveDarling,KyleGrant,LouiseLorenc,AndyBenson.
Ascollaboratorsatreceivinghospitals:Dr.PhilipMoran (Lak-eridgeHealth);Dr.DonnaMcRitchie(NorthYorkGeneralHospital); Dr.JoeyButchey(RougeValleyHealthSystem);Dr.RobertCirone (St.Joseph’sHealthCentre);Dr.TomChan(TheScarborough Hos-pital);Dr.AngieStone(MichaelGarronHospital);Dr.JanosPataki andDr.EricLetovsky(TrilliumHealthPartners);Dr.NiallFerguson andDr.EyalGolan(MountSinaiHospitalandUniversityHealth Network);Dr.MichelleWelsford(HamiltonHealthSciences).
TheDataSafetyandMonitoringCommitteewascomprisedof 3 expertsincritical careand emergencymedicine, clinicaltrial methodology, andbiostatistics: H.TomStelfoxMDPhD (Chair; expertin criticalcare,clinicaltrials,andclinicalepidemiology); GeorgeA.Wells,MSc,PhD(methodologicalandstatisticalexpertise intheconductofclinicaltrials);BrianH.Rowe,MD,MSc(expertin emergencymedicine,clinicaltrials,andclinicalepidemiology).
AppendixA. Supplementarydata
Supplementarydataassociatedwiththisarticlecanbefound,in theonlineversion,athttps://doi.org/10.1016/j.resuscitation.2017. 10.002.
References
[1].Bernard SA, Gray TW, Buist MD, etal. Treatment ofcomatose survivors ofout-of-hospital cardiacarrestwith inducedhypothermia.N EnglJMed 2002;346(8):557–63.
[2].Hypothermia after Cardiac ArrestStudy G. Mildtherapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N Engl J Med 2002;346(8):549–56.
[3].YenariMA,HanHS.Neuroprotectivemechanismsofhypothermia inbrain ischaemia.NatRevNeurosci2012;13(4):267–78.
[4].CallawayCW,DonninoMW,FinkEL,etal.Part8:post-cardiacarrestcare:2015 americanheartassociationguidelinesupdateforcardiopulmonaryresuscitation andemergencycardiovascularcare.Circulation2015;132(18Suppl.2):S465–82. [5].HowesD,GraySH,BrooksSC,etal.Canadianguidelinesfortheuseof tar-getedtemperaturemanagement(therapeutichypothermia)aftercardiacarrest: ajointstatementfromTheCanadianCriticalCareSociety(CCCS),Canadian Neu-rocriticalCareSociety(CNCCS),andtheCanadianCriticalCareTrialsGroup (CCCTG).Resuscitation2016;98:48–63.
[6].BrooksSC,ScalesDC,PintoR,etal.Thepostcardiacarrestconsultteam:impact onhospitalcareprocessesforout-of-hospitalcardiacarrestpatients.CritCare Med2016;44(November11):2037–44.
[7].WorthingtonH,PickettW,MorrisonLJ,etal.Theimpactofhospital experi-encewithout-of-hospitalcardiacarrestpatientsonpostcardiacarrestcare. Resuscitation2017;110(January):169–75.
[8].LaverSR,PadkinA,AtallaA,etal.Therapeutichypothermiaaftercardiacarrest: asurveyofpracticeinintensivecareunitsintheUnitedKingdom.Anaesthesia 2006;61(9):873–7.
[9]. StormC,MeyerT,SchroederT,etal.Useoftargettemperaturemanagement aftercardiacarrestinGermany–anationwidesurveyincluding951intensive careunits.Resuscitation2014;85(8):1012–7.
[10].Binks AC, Murphy RE, Prout RE, et al. Therapeutic hypothermia after cardiac arrest –implementation in UK intensive care units. Anaesthesia 2010;65(3):260–5.
[11].BighamBL,Dainty KN,ScalesDC,etal. Predictorsofadoptingtherapeutic hypothermiaforpost-cardiacarrestpatientsamongCanadianemergencyand criticalcarephysicians.Resuscitation2010;81(1):20–4.
[12].DaleCM,SinuffT,MorrisonLJ,etal.Understandingearlydecisionstowithdraw life-sustainingtherapyincardiacarrestsurvivor.Aqualitativeinvestigation. AnnAmThoracSoc2016;13(7):1115–22.
[13].KimYM,LeeSJ,JoSJ,etal.Implementationoftheguidelinesfortargeted tem-peraturemanagementaftercardiacarrest:alongitudinalqualitativestudyof barriersandfacilitatorsperceivedbyhospitalresuscitationchampions.BMJ Open2016;6(1):e009261.
[14].TomaA,BensimonCM,Dainty KN, etal. Perceived barriers to therapeu-tichypothermiaforpatientsresuscitatedfromcardiacarrest:aqualitative study ofemergencydepartment andcritical care workers.Crit Care Med 2010;38(2):504–9.
[15].MorrisonLJ,BrooksSC,DaintyKN,etal.Improvinguseoftargeted tempera-turemanagementafterout-of-hospitalcardiacarrest:asteppedwedgecluster randomizedcontrolledtrial.CritCareMed2015;43(5):954–64.
[16].HalpernSD,UbelPA,AschDA.Harnessingthepowerofdefaultoptionsto improvehealthcare.NEnglJMed2007;357(13):1340–4.
[17].DaintyKN,ScalesDC,BrooksSC,etal.Aknowledgetranslationcollaborative toimprovetheuseoftherapeutichypothermiainpost-cardiacarrestpatients: protocolforasteppedwedgerandomizedtrial.ImplementSci2011;6:4. [18].DoigGS,SimpsonF.Randomizationandallocationconcealment:apractical
guideforresearchers.JCritCare2005;20(2):187–91,discussion91-3. [19].MorrisonLJ,LongJ,VermeulenM,etal.Arandomizedcontrolledfeasibilitytrial
comparingsafetyandeffectivenessofprehospitalpacingversusconventional treatment:‘PrePACE’.Resuscitation2008;76(3):341–9.
[20].MorrisonLJ, Rizoli SB,Schwartz B, etal. The Torontoprehospital hyper-tonic resuscitation-headinjuryand multi organ dysfunction trial(TOPHR HIT)–methodsanddatacollectiontools.Trials2009;10:105.
[21].JacobsI,NadkarniV,BahrJ,etal.Cardiacarrestandcardiopulmonary resus-citationoutcomereports:updateandsimplificationoftheUtsteintemplates forresuscitationregistries.Astatementforhealthcareprofessionalsfromatask forceoftheinternationalliaisoncommitteeonresuscitation(AmericanHeart Association,EuropeanResuscitationCouncil,AustralianResuscitationCouncil, NewZealandResuscitationCouncil,HeartandStrokeFoundationofCanada, InterAmericanHeartFoundation,ResuscitationCouncil ofSouthernAfrica). Resuscitation2004;63(3):233–49.
[22].LinS,MorrisonLJ,BrooksSC.Developmentofadatadictionaryforthe Strate-giesforPostArrestResuscitationCare(SPARC)networkforpostcardiacarrest research.Resuscitation2011;82(4):419–22.
[23].vanSwietenJC,KoudstaalPJ,VisserMC,etal.Interobserveragreementforthe assessmentofhandicapinstrokepatients.Stroke1988;19(5):604–7.
[24].Sedgwick P. Treatment allocation in trials: stratified randomisation. BMJ 2015;350:h978.
[25].CumminsRO,ChamberlainDA,AbramsonNS,etal.Recommendedguidelines foruniformreportingofdatafromout-of-hospitalcardiacarrest:theUtstein StyleAstatementforhealthprofessionalsfromataskforceoftheAmerican HeartAssociation,theEuropeanResuscitationCouncil,theHeartandStroke FoundationofCanada,andtheAustralianResuscitationCouncil.Circulation 1991;84(2):960–75.
[26].LaiTL,ShihMC,ZhuG.ModifiedHaybittle-Petogroupsequentialdesignsfor testingsuperiorityandnon-inferiorityhypothesesinclinicaltrials.StatMed 2006;25(7):1149–67.
[27].KimF, NicholG, MaynardC,etal.Effectofprehospitalinductionofmild hypothermiaonsurvivalandneurologicalstatusamongadultswithcardiac arrest:arandomizedclinicaltrial.JAMA2014;311(1):45–52.
[28].NielsenN,Wetterslev J,Cronberg T,etal. Targetedtemperature manage-mentat33degreesCversus36degreesCaftercardiacarrest.NEnglJMed 2013;369(23):2197–206.
[29].RaoMP,DupreME,PokorneySD,etal.Therapeutichypothermiaforpatients with out-of-hospitalcardiac arrestinnorth carolina.Prehosp EmergCare 2016;20(5):630–6.
[30].DiaoM,HuangF,GuanJ,etal.Prehospitaltherapeutichypothermiaaftercardiac arrest:asystematicreviewandmeta-analysisofrandomizedcontrolledtrials. Resuscitation2013;84(8):1021–8.
[31].HuangFY,HuangBT,WangPJ,etal.Theefficacyandsafetyofprehospital thera-peutichypothermiainpatientswithout-of-hospitalcardiacarrest:asystematic reviewandmeta-analysis.Resuscitation2015;96:170–9.
[32].BernardSA,SmithK,FinnJ,etal.Inductionoftherapeutichypothermiaduring out-of-hospitalcardiacarrestusingarapidinfusionofcoldSaline:theRINSE trial(rapidinfusionofcoldnormalsaline).Circulation2016;134(11):797–805. [33].SalcidoDD,StephensonAM,CondleJP,etal.Incidenceofrearrestafterreturnof spontaneouscirculationinout-of-hospitalcardiacarrest.PrehospEmergCare 2010;14(4):413–8.
[34].SalcidoDD,SundermannML,KollerAC,etal.Incidenceandoutcomesofrearrest followingout-of-hospitalcardiacarrest.Resuscitation2015;86:19–24. [35].LinS,ScalesDC,DorianP,etal.Targetedtemperaturemanagementprocesses
andoutcomesafterout-of-hospital cardiacarrest:anobservationalcohort study*.CritCareMed2014;42(12):2565–74.
[36].MaioRF,GarrisonHG,SpaiteDW,etal.Emergencymedicalservicesoutcomes projectI(EMSOPI):prioritizingconditionsforoutcomesresearch.AnnEmerg Med1999;33(4):423–32.
[37].vandeGlindI,BerbenS,ZeegersF,etal.Anationalresearchagendafor pre-hospitalemergencymedicalservicesintheNetherlands:aDelphi-study.Scand JTraumaResuscitationEmergMed2016;24:2.
[38].AbereggSK,RichardsDR,O’BrienJM.Deltainflation:abiasinthedesignof randomizedcontrolledtrialsincriticalcaremedicine.CritCare2010;14(2):R77. [39].Harhay MO,Wagner J, RatcliffeSJ,et al. Outcomesand statistical power in adult critical care randomized trials. Am J Respir Crit Care Med 2014;189(12):1469–78.
[40].Martin-GillC,GaitherJB,BighamBL,etal.Nationalprehospitalevidence-based guidelinesstrategy:asummaryforEMSstakeholders.PrehospEmergCare 2016;20(2):175–83.