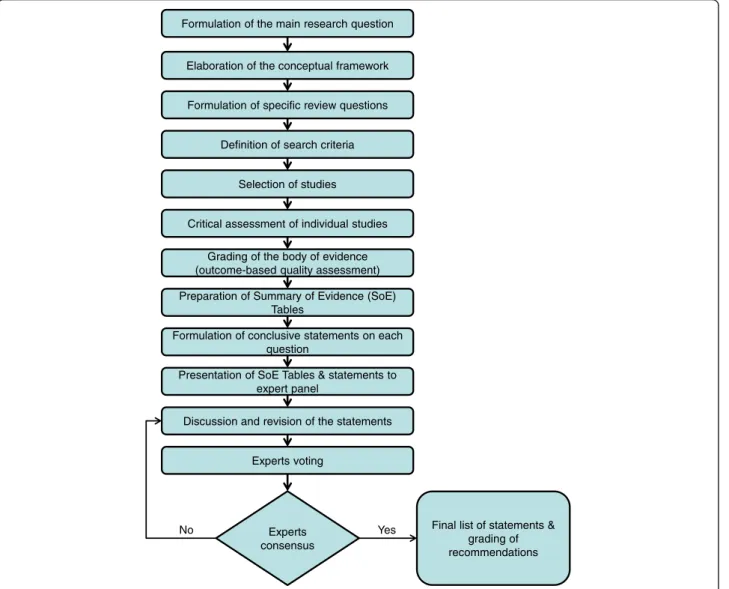
The effectiveness of scoliosis screening programs: methods for systematic review and expert panel recommendations formulation
Texte intégral
Figure

Documents relatifs
National Research Council; OHAT, Office of Health Assessment and Translation; PF, Practical Framework; PN, Prescriptive nature; REL, Relevance; SCENIHR, Scientific Committee on
Approach using Convolutional Neural Network for object recognition where, it can be human, hand or any other object to define, gives another alternative on problem solving
Methods: We followed up for 2 years a RJ State prison for adult males (1429 inmates at the beginning of the study) and performed, in addition to passive case-finding, 1) two
(1995) Grand Canonical Monte Carlo simulations of chain molecules: adsorption isotherms of alkanes in zeolites, Mol.. (1995) Simulating the adsorption isotherms of methane, ethane,
This review (1) identifies multidimensional screening tools that include psychosocial risk factors for the development or maintenance of pain, pain-related distress, and
HCL-32, without modifications. Unavailable Unavailable Adolescents with bulimia endorsed less symptoms in the HCL-32, and significantly correlated with lack of
La section qui suit doit ˆetre vue comme la description d’un prototype, qui fonctionne et a ´et´e test´e dans la premi`ere version de g´en´erateur des pages web de
National Research Council; OHAT, Office of Health Assessment and Translation; PF, Practical Framework; PN, Prescriptive nature; REL, Relevance; SCENIHR, Scientific Committee on
