ArchivesofCardiovascularDisease(2018)111,686—701
Availableonlineat
ScienceDirect
www.sciencedirect.com
CLINICAL
RESEARCH
Accuracy
of
cardiac
magnetic
resonance
imaging
to
rule
out
significant
coronary
artery
disease
in
patients
with
systolic
heart
failure
of
unknown
aetiology:
Single-centre
experience
and
comprehensive
meta-analysis
Intérêt
de
l’imagerie
par
résonance
magnétique
cardiaque
pour
exclure
la
présence
d’une
coronaropathie
sous-jacente
chez
les
patients
avec
insuffisance
cardiaque
systolique
d’étiologie
inconnue
:
expérience
monocentrique
et
méta-analyse
Aurélie
Manchuelle
a,
Franc
¸ois
Pontana
b,c,d,e,
Pascal
De
Groote
a,d,f,
Paul
Lebert
b,
Marie
Fertin
a,
Marine
Baijot
a,
Christopher
Hurt
a,
Nicolas
Lamblin
a,c,d,f,
Nicolas
Debry
a,
Guillaume
Schurtz
a,
Anju
Duva
Pentiah
a,
Arnaud
Sudre
a,
Martine
Remy-Jardin
b,c,
Patrizio
Lancellotti
g,h,
Eric
Van
Belle
a,c,d,e,
Christophe
Bauters
a,c,d,f,
Gilles
Lemesle
a,c,d,e,
Cédric
Delhaye
a,∗aServicedecardiologie,institutcœurpoumon,centrehospitalierrégionaletuniversitairede Lille,59000Lille,France
bServicederadiologie,institutcœurpoumon,centrehospitalierrégionaletuniversitairede Lille,59000Lille,France
cFacultédemédecinedeLille,universitédeLille,59000Lille,France dInstitutPasteurdeLille,59000Lille,France
eInsermU1011,59000Lille,France
Abbreviations:CA,coronaryangiogram/angiography;CAD,coronaryarterydisease;CMR,cardiacmagneticresonanceimaging;HF,heart
failure;LGE,lategadoliniumenhancement;LVEF,leftventricularejectionfraction;NLR,negativelikelihoodratio;PLR,positivelikelihood ratio;st-LGE,subendocardialortransmurallategadoliniumenhancement.
∗Correspondingauthor.Institutcœurpoumon,centrehospitalierrégionaletuniversitairedeLille,boulevardProf.-Leclercq,59037Lille
cedex,France.
E-mailaddress:[email protected](C.Delhaye).
https://doi.org/10.1016/j.acvd.2018.04.004
CMRandHFaetiology 687
fInsermU1167,59000Lille,France
gDepartmentofCardiology,HeartValveClinic,UniversityofLiègeHospital,GIGA
CardiovascularSciences,CHUSartTilman,4000Liège,Belgium
hGruppoVillaMariaCareandResearch,AntheaHospital,70124Bari,Italy
Received20January2018;receivedinrevisedform6April2018;accepted9April2018 Availableonline1June2018
KEYWORDS Coronaryartery disease; Magneticresonance imaging; Lategadolinium enhancement; Coronaryangiogram; Heartfailure Summary
Background.—Coronaryarterydisease(CAD)istheleadingcauseofsystolicheartfailure(HF). Cardiacmagneticresonanceimaging(CMR)isanon-invasivetechniquethatdetectsamyocardial infarctionscarassubendocardialortransmurallategadoliniumenhancement(st-LGE). Aim.—Wesoughttoevaluatewhetheralackofst-LGEcouldruleoutCADinnew-onsetsystolic HFofunknownaetiology.
Methods.—Weincluded232consecutivepatientswithnew-onsetHFandleftventricular ejec-tionfraction ≤35%whounderwentbothcoronaryangiographyandCMRtoassessHFaetiology. CADwasdefinedasthepresenceofcoronaryarterystenosis≥50%onacoronaryangiogram. Weassessedsensitivity,specificity,andpositiveandnegativelikelihoodratios(PLRandNLR)of thepresenceofst-LGEtodetectunderlyingCAD.Acomplementarymeta-analysisof11studies (includingours)wasalsoperformed.
Results.—Inourstudy,49(21.1%)patientshadCAD.Thesensitivityandspecificityofthe pres-ence ofst-LGE to detect CADwere 69 and92%, respectively. PLRand NLR were 8.47and 0.33,respectively.Inthemeta-analysis,1227patientswereincluded,andtheprevalenceof CADrangedfrom19.2to68.3%.Sensitivity,specificity,PLRandNLRwere87%(95%confidence interval[CI]0.80—0.92),93%(95%CI0.89—0.96),12.91(95%CI7.70—21.64)and0.14(95%CI 0.09—0.22),respectively.Altogether,55patientspresentedCADwithnost-LGE;inversely,75 patientspresentedst-LGEwithnoCAD.
Conclusion.—WithaCMRspecificityof93%,theabsenceofst-LGErulesoutsignificant under-lyingCADinpatientswithsystolicHFofunknownaetiologyinmostcases.
©2018PublishedbyElsevierMassonSAS.
MOTSCLÉS Coronaropathie; Imageriepar résonance magnétique; Rehaussement tardif; Angiographie coronaire; Insuffisance cardiaque Résumé
Contexte.—Lacoronaropathieestlaprincipalecaused’insuffisancecardiaque(IC)systolique. L’imagerie parrésonancemagnétiquecardiaque (IRM-C)estune techniquenoninvasivequi permetdedétecterlescicatricesd’infarctusdumyocardesousla formed’unrehaussement tardifsous-endocardiqueoutransmuralaprèsinjectiondegadolinium(st-RT).
Objectif.—L’objectifdecetteétudeestd’évaluersil’absencedest-RTpeutexclurela coro-naropathiechezlespatientsprésentantuneICsystoliqued’étiologieinconnue.
Méthodes.—Autotal,232patientsconsécutifsprésentantuneICavecunefractiond’éjection ventriculairegauche ≤35%etquionteuàlafoisuneangiographiecoronaireetuneIRM-C ontétéinclus.Lacoronaropathieétaitdéfinieparlaprésenced’unesténosecoronaire≥50% enangiographie.Lasensibilité,laspécificité,lesrapportsdevraisemblancepositifsetnégatifs (RVPetRVN)delaprésenced’unst-RTàl’IRM-Cpourdétecterlacoronaropathieontétéévalué. Uneméta-analysecomplémentairede11études(dontlanôtre)aégalementétéréalisée. Résultats.—Dansnotreétude,49(21,1%)patientsavaientunecoronaropathie.Lasensibilité etlaspécificitédelaprésencedest-RTpourdétectercettedernièreétaientde69et92%, respectivement.Les RVPetRVNétaient respectivementde8,47et0,33.Laméta-analysea inclus1227patients.Laprévalencedelacoronaropathievariaitde19,2à68,3%.Lasensibilité, laspécificité,leRVPetleRVNétaientrespectivementde87%(IC95%0,80—0,92),93%(IC95% 0,89—0,96),12,91(IC95 %7,70—21,64)et0,14(IC95%0,09—0,22).Autotal,55 patientsne présentaientpasdest-RTmaisunecoronaropathie;inversement75patientsprésentaientune st-LGEsanscoronaropathie.
Conclusion.—Avecunespécificitédel’IRMcardiaquede93%,l’absencedest-RTexclutune coronaropathie chez les patients présentantune IC systoliqued’étiologie inconnue dans la plupartdescas.
688 A.Manchuelleetal.
Background
Coronaryarterydisease(CAD)iscurrentlytheleadingcause ofsystolicheart failure(HF),andimpactspatient progno-sisand care in practice [1]. In this context, the need to systematicallyperform a coronary angiogram (CA), which is an invasive procedure, in patients with systolic HF of unknownaetiologyhasbeenchallengedbynewtechniques. Cardiac magnetic resonance imaging (CMR) has emerged asa non-invasive technique that provides high-resolution imagesoftheheartinanydesiredplaneandwithout radi-ation; it assesses cardiac morphology and function, and the presence and extent of myocardial infarction scar, by showing subendocardial or transmural late gadolinium enhancement(st-LGE)[2].Recentsmall-scaleinvestigations havesuggestedthatlategadoliniumenhancement(LGE)can distinguish whether HF is related to CAD [3—14]. There-fore,the inclusion of CMR in the clinical management of patientswithsystolicHFofunknownaetiologymightavoid unnecessaryinvasivediagnosticcoronaryangiography(CA) procedures.
Inthepresentstudy,wesoughttoassessthediagnostic accuracyofst-LGEonCMR toruleoutsignificant underly-ingCADinpatientswithnew-onsetsystolicHFofunknown aetiology,andtoincludeourdatainacomprehensive meta-analysisofitsdiagnosticaccuracy comparedwithinvasive CAasareferencestandard.
Methods
Patient
population
Anongoingregistryofcatheter-basedcoronaryprocedures is maintained at our institution. From February 2005 to December 2016, all consecutive patients who underwent CAfornew-onsetsystolicHF(leftventricularejection frac-tion[LVEF]≤35%ontransthoracicechocardiography)were screened.Thosewhohadnoclinicalorelectricalevidence suggestiveofCAD,andforwhomCMRwasavailable,were included inthe present analysis.Duringthe study period, patients presenting withnew-onset HF and reduced LVEF wereroutinely referredforbothCAandCMR.Lackof evi-dence suggestive of CAD was considered in cases of no clinical evidence (no history of documented CAD [history ofunstableangina and/orhistory ofmyocardialinfarction and/orpreviouspercutaneouscoronaryinterventionand/or previouscoronarybypassand/orpreviousCAshowing>50% diameterluminalstenosisinanyepicardialcoronaryartery] orpresenceoftypicalchestpain),andnoelectrocardiogram evidence(pathologicalQwaves).Regionalwallmotion alter-ationontransthoracicechocardiographywasnotconsidered tobediscriminatingforCAD,becausethisvariableisknown tobenon-specific[15].Thefinalstudypopulationconsisted of232patientswithnewsystolicHF.
CA
Conventional techniques were used to perform the CA. Patients were considered to have CAD when≥50% diam-eter luminal stenosis in any epicardial coronary artery (with a diameter>2mm) was observed. Two experienced
interventional cardiologists (A.M. and C.D.) reviewed the CA inblinded conditions.Incases of discrepancy, consen-sus was reached by discussion with a third experienced interventionalcardiologist(G.L.).
CMR
All patients were examined using a 1.5 Tesla MR sys-tem(AchievaTM;PhilipsHealthcare,Best,TheNetherlands).
DetailedinformationabouttheCMRisavailableinAppendix B. LGE imaging was performed 10minutes after an intravenous bolus of 0.4mL/kg (0.2mmol/kg) of gadoter-atemeglumine (Dotarem®; Guerbet, Roissy, France), with optimization of inversion times using inversion recovery pulses to null the signal from the normal myocardium. Images wereevaluatedindependently bytwoexperienced radiologists(F.P.andP.L.),whowereblindedtotheclinical variablesandtheCAresults.Incasesofdiscrepancy, consen-suswasreachedbydiscussionwithathirdradiologist(M.R.). End-diastolicandend-systolicvolumeswerecalculatedfrom manualcontouring.Theleftmyocardiumwasanalysedin17 segmentsaccordingtostandardizedreportedsegmentation. Tobevalidated,LGEmustbepresentinthesamemyocardial segmentinatleasttwodifferentplanes.Whenpresent, st-LGEwasthendescribedusingathree-pointscale,according tothemyocardialthicknessinvolved(1=<25%;2=25—75%; 3=>75%).Onlyst-LGEwasconsideredforthepresent anal-ysis to assess the accuracy of CMR to detect underlying CAD in patients with HF of unknown aetiology. However, subepicardialorintramyocardialenhancementwithoutany coronaryarterydistributionwasalsoreportedandincluded withpatientswithnoLGEinthegroupofpatientswithno st-LGE,accordingtothepreviousliterature[16].
Meta-analysis
The PubMed database was searched for eligible stud-ies, with no time restriction, on 5 April 2017, by using the combined medical subject headings for ‘‘coronary artery disease, left ventricular dysfunction, heart fail-ure,ischaemic,lategadoliniumenhancementandmagnetic resonance imaging’’. The complete search used for PubMed was: (coronary artery disease[Title/Abstract] OR left ventricular dysfunction[Title/Abstract] OR heart fail-ure[Title/Abstract]ORischaemic[Title/Abstract])ANDlate gadoliniumenhancement[Title/Abstract]ORmagnetic res-onance imaging[Title/Abstract]) AND english[Language]. Two investigators (G.L. and C.D.) independently checked retrieved titles and abstracts for eligibility, and relevant fulltextsweresystematicallyretrievedforfurtherdetailed assessment. Major reviews regarding the place of CMR in HFwerealsohand searched.Cross-referencesand quoted paperswerechecked,andexpertswerecontactedto iden-tify other relevant studies. The retrieved studies were examinedtoexcludeduplicateoroverlappingdata. Unpub-lished data were not considered for the present analysis, because results could not be considered as certain and definitive.Meeting abstracts werealsoexcluded, because theycouldnotprovideadequatelydetaileddataandtheir resultsmightnothavebeenfinal.
CMRandHFaetiology 689 • iftheyincludedpatientswithsystolicHFofunknown
aeti-ology;
• iftheyreportedst-LGEbythepresenceofsignificantCAD statusonCA;
• iftheyreportedacleardefinitionofsignificantCAD; • iftheabsolutenumbersoftruepositives,falsepositives,
truenegativesandfalsenegativeswerereportedorcould bederived.
Studieswereexcluded:
• iftheyfocusedonpatientswithknownspecific cardiomy-opathy as post-partum cardiomyopathy, hypertrophic cardiomyopathy, amyloid, sarcoidosis or mitochondrial cardiomyopathy,rightventriculardysplasiaorcongenital heartdisease;
• iftheyfocusedonpatientswithCADonly; • iftheyfocusedonpatientswithoutCAD; • iftheyfocusedonpatientswithLVEF>50%;
• ifacleardefinitionofsignificantCADwasnotreported; • ifst-LGEwasnotreportedbyCADstatus;
• if they were performed with no final report and only abstractsavailable;
• iftheywereperformedinanimals.
The information that was systematically searched for and extracted from each study is presented in Appendix B.Threeinvestigators(G.L.,C.D.andA.M.)performedthe data extraction independently; discrepancies were solved by consensus. Two investigators (G.L. and C.D.) indepen-dentlyassessedthequalityofallincludedstudiesusingthe revised quality assessment of diagnostic accuracy studies (QUADAS-2) tool [17]. Any disagreement wasresolved by consensus.
Statistical
analysis
Continuous variables are expressed as means±standard deviations, except for delays, which are expressed as medians[25th—75thpercentiles].Categoricalvariablesare expressedasnumbers (percentages). Student’s ttest was used to compare continuous variables, and the 2 test
or Fisher’s exact test was used to compare categorical variables.Delaysbetweengroupswerecomparedusingthe Mann-WhitneyUtest.
Sensitivity and specificity were calculated using true positive, true negative, false positive and false nega-tive rates. Sensitivity was calculated as the number of patients with CAD and st-LGE divided by the number of patients with CAD; specificity was calculated as the number of patients without CAD and no st-LGE divided by the number of patients without CAD. Also calcu-latedwere thelikelihoodratios,which expresshowmuch the odds of CAD change in the presence of st-LGE (positivelikelihoodratio[PLR]=sensitivity/[1—specificity]) or in the absence of st-LGE (negative likelihood ratio [NLR]=[1—sensitivity]/specificity). Post-test probability oddsexpressed inpercentages with95% confidence inter-vals(CIs)werecalculated,definedbytheprobabilityofCAD afterapositivetestandafteranegativetest,represented inaFagandiagram.
All these measures of diagnostic accuracy were also calculatedforeach individualstudyincludedin the meta-analysis,andwerereportedaspointestimateswith95%CIs.
Pooledresults for the meta-analysiswerecalculated with STATA software,version 14.0 (StataCorp, College Station, TX,USA)usingtheMIDAScommand.Between-study statis-ticalheterogeneitywasassessedbyusingtheCochranQ2
testandtheI2test.Thestudywasperformedaccordingto
establishedmethods,andincompliancewiththequalityof reportingofmeta-analyses(QUORUM)guidelines[18].
AllstatisticalanalyseswereperformedwithSTATA soft-wareversion14.1 (StataCorp).Statistical significance was assumedataPvalue<0.05.
Results
Single-centre
experience
Population
Thebaselinecharacteristicsofthepatientsaresummarized
in Table 1. In the overall population, the mean age was
57.3±12.3 years. Altogether, 79.3% of cases were male, and15.1% had diabetes. The mean LVEF was22.5±7.5%, asassessedbytransthoracicechocardiography.Themedian delaybetweenCAandCMRwas2[1—6]days.
Significant obstructive CAD was found in 49 patients (21.1%). Patientswith CAD were older (62.4 vs 56 years;
P=0.001) and more often had diabetes (26.5% vs 12.0%;
P=0.012)andhypertension(49.0%vs32.2%;P=0.03)than thosewithoutCADatinclusion.
Regarding CMR data, st-LGE was found in 49 patients (21.1%)intheoverallpopulation.Patientswithst-LGEwere moreoftenmale(91.8%vs76.0%;P=0.015)thanthose with-outst-LGEatinclusion.
Diagnostic
accuracy
of
st-LGE
Altogether,st-LGEwasfoundin34(truepositives,69.4%)of the49patients withCAD,andin15(falsepositives,8.2%) ofthe183patientswithoutCAD.CMRdidnotreportany st-LGEin 15(falsenegatives,30.6%) ofthe 49patients with
CAD(Table2).Repartitionofthepatients accordingto
st-LGEandCADstatusisdepictedinFig.1.Therefore,inour population,thesensitivityandspecificityofthepresenceof st-LGEonCMRtodetectCADwere69%and92%,respectively. PLRandNLRwere8.47and0.33,respectively.The descrip-tionoftheunderlyingCADinthe15patientswithsignificant obstructiveCADbutnost-LGEonCMRisavailableinTable3. Ofnote,11patientshadsingle-vesseldisease(includingonly onewithsevere [>70%]stenosis), threepatients had two-vesseldiseaseandonepatienthadthree-vesseldisease.
Meta-analysis
Search
results
and
study
selection
Wefound3232citationsinPubMedandotherdatasources. Therewere113relevantstudies,forwhichadetailed assess-mentofthefulltextwasperformed.Wefinallyincluded11 studies(includingourown)[3—12]andexcluded102others. The reasonsfor exclusionwere study focused onpatients withCAD only (n=23); study focused onpatients with no CAD(n=53);studydidnotfocusonpatientswithsystolicHF (n=9);studydidnotreportst-LGEbyCADstatus(n=17);and studyhadduplicatedata(n=9).Astudycouldbeexcluded
690 A.Manchuelleetal. Table1 Baselinecharacteristicsofourpopulation.
Total population
WithCAD Without CAD P With st-LGE Without st-LGE P (n=232) (n=49) (n=183) (n=49) (n=183) Demographics Age(years) 57.3±12.3 62.4±11.9 56±12 0.001 57.3±10.9 57.3±12.6 0.987 Malesex 184(79.3) 43(87.8) 141(77.0) 0.100 45(91.8) 139(76.0) 0.015 Riskfactors Bodymassindex (kg/m2) 26.6±5.8 26±4.5 26.8±6.1 0.399 25.9±4.1 26.9±6.2 0.291 Diabetesmellitus 35(15.1) 13(26.5) 22(12.0) 0.012 10(20.4) 25(13.7) 0.248 Hypertension 83(35.8) 24(49.0) 59(32.2) 0.030 19(38.8) 64(35.0) 0.622 Activesmoker 149(64.2) 35(71.4) 114(62.3) 0.236 35(71.4) 114(62.3) 0.236 Hypercholestero-laemia 60(25.9) 15(30.6) 45(24.6) 0.393 11(22.4) 49(26.8) 0.539 Familialhistoryof CAD 40(17.2) 8(16.3) 32(17.5) 0.849 8(16.3) 32(17.5) 0.849 Peripheralarterial diseaseorcarotid disease 20(8.6) 6(12.2) 14(7.7) 0.309 7(14.3) 13(7.1) 0.112 Initialclinical presentation Acutepulmonary oedema 42(18.1) 12(24.5) 30(16.4) 0.191 13(26.5) 29(15.8) 0.085 Othercongestive symptomsa 190(81.9) 37(75.5) 153(83.6) — 36(73.5) 154(84.2) — Electrocardiogram findings Atrialfibrillation 42(18.1) 9(18.4) 33(18.0) 0.970 5(10.2) 37(20.2) 0.103 Leftbundlebranch
block
49(21.1) 14(28.6) 35(19.1) 0.156 12(24.5) 37(20.2) 0.527 LVEFby
echocardiography(%)
22.5±7.5 23.3±7.6 22.3±7.5 0.407 21.7±7 22.7±7.7 0.382 DelaybetweenCAand
CMR(days) 2[1—6] 2[1—4] 3[1—6] 0.036 1[1—5] 3[1—6] 0.099 CAdata ObstructiveCAD 49(21.1) 49(100) — — 34(69.4) 15(8.2) <0.0001 One-vesselCAD 28(12.1) 28(57.1) — — 16(32.7) 12(6.6) <0.0001 MultivesselCAD 21(9.0) 21(42.9) — — 18(36.7) 3(1.6) — Delaybetween
symptomonsetand CA(days) 12[9—21] 12[9—19] 12[9—21] 0.911 12[9—21] 12[9—21] 0.815 CMRdata st-LGE 49(21.1) 34(69.4) 15(8.2) <0.0001 49(100) — — Subepicardialor nodular(atypical) LGE 14(6.0) 1(2.0) 13(7.1) 0.184 — 14(7.7) — Delaybetween symptomonsetand CMR(days)
11[7—15] 6[11—14] 7[11—15] 0.305 6[11—15] 7[11—15] 0.511
Dataareexpressedasmean±standarddeviation,number(%)ormedian[25th—75thpercentiles].CA:coronaryangiogram;CAD:coronary arterydisease;CMR:cardiacmagneticresonanceimaging;LGE:lategadoliniumenhancement;LVEF:leftventricleejectionfraction; NYHA:NewYorkHeartAssociation;st-LGE:subendocardialortransmurallategadoliniumenhancement.
CMRandHFaetiology 691 Table2 Numbersoftruepositive,falsepositive,truenegativeandfalsenegativepatientsinthe11studiesincludedin themeta-analysis.
Study All
patients
TPs(patientswith CADandst-LGE)
FNs(patientswith CADandnost-LGE)
FPs(patientswith noCADandst-LGE)
TNs(patientswithno CADandnost-LGE) McCrohonetal. (2003) 90 27 0 8 55 Casoloetal. (2006) 60 40 1 3 16 Sorianoetal. (2007) 123 39 11 8 65 Schietingeretal. (2007) 26 2 3 0 21 LePolainde Warouxetal. (2008) 71 24 7 5 35 Valle-Munoz etal.(2009) 100 18 3 6 73 Krittayaphong etal.(2011) 98 53 5 0 40 Gaoetal.(2012) 124 59 0 8 57 DiBellaetal. (2016) 187 77 9 6 95 Thompsonetal. (2017) 116 73 1 16 26 Manchuelleetal. (2018) 232 34 15 15 168
Dataareexpressedasnumber.CAD:coronaryarterydisease;FN:falsenegative;FP:falsepositive;st-LGE:subendocardialortransmural lategadoliniumenhancement(atleastonesegment);TN:truenegative;TP:truepositive.
Figure1. Studypopulationaccordingtothepresenceof suben-docardialortransmurallategadoliniumenhancement(st-LGE)and coronaryarterydisease(CAD).HF:heartfailure;LVEF:left ventric-ularejectionfraction.
for severalreasons. The flow chartof thestudy selection processisshowninFig.2.
Study
and
patient
characteristics
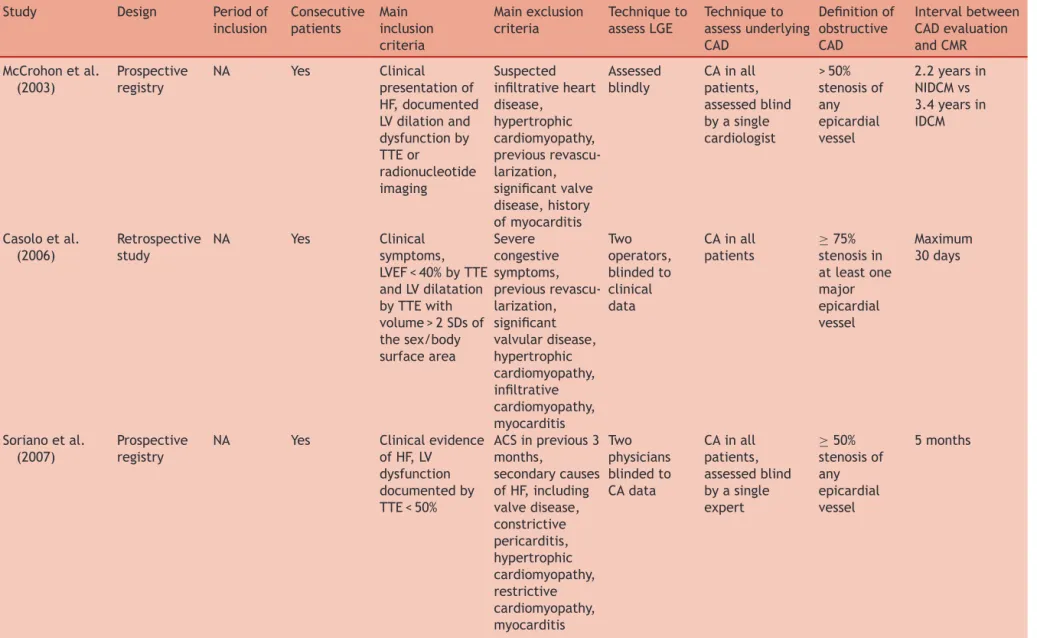
Altogether,11studiesand1227patientswereincludedinthe meta-analysis.Detailedinformationaboutthe11included studies is presented in Table 3 andTable 4: eightstudies were prospective registries and three were retrospective studies.Theyearofpublicationrangedfrom2003to2017. Themedianageofincludedpatientsrangedfrom49to66.4 years.Therateofmalesexrangedfrom65to80.6%,andthe
Figure2. Flowchartofthestudyselectionprocess.CAD: coro-naryarterydisease; HF:heartfailure;st-LGE:subendocardialor transmurallategadoliniumenhancement.*:asinglestudycouldbe excludedforseveralreasons.
rateofdiabetesmellitusrangedfrom11.5to42.9%amongin theeightstudiesthatreportedthisinformation.Themedian LVEFrangedfrom25to40%.ThemediantimebetweenCAD assessmentbyCAandst-LGEassessmentbyCMRrangedfrom 2daysto3.4yearsintheeightstudiesthatreportedthese data.ThedefinitionofobstructiveCADdifferedacrossthe studies.TheprevalenceofCADrangedfrom19.2to68.3%.
692
A.
Manchuelle
et
al.
Table3 Mainpatientcharacteristicsinthe11studiesincludedinthemeta-analysis.
Study Patients (n) Age (years) Men Diabetes mellitus LVEF Prevalenceof obstructiveCAD Prevalence ofst-LGE Prevalence ofatypical LGE
DescriptionofunderlyingCADin patientswithCADandnost-LGE McCrohonetal. (2003) 90 54inNIDCM vs67in IDCM 41(65.0) NA 39%in NIDCMvs 33%in IDCM assessed byCMR
27(30.0) 35(38.9) 18(20.0) NopatientwithCADandnost-LGE
Casoloetal. (2006)
60 66.4 44(73.3) 12(20.0) 35%
assessed byTTE
41(68.3) 56(93.0) 0(0) Onepatient:severelesionoftheLM
Sorianoetal. (2007)
123 60 99(80.5) 32(26.0) 28%
assessed byTTE
50(40.7) 47(38.2) NA 11patients:ninewithsinglevessel
diseaseandtwowithtwo-vessel disease,notinvolvingtheLMor proximalLADinallcases Schietingeretal.
(2007)
26 49 19(73.1) 3(11.5) 25%
assessed byCMR
5(19.2) 2(7.7) 2(7.7) Threepatients:allwithsignificant
stenosisoftheLADandatleastone othermajorcoronaryartery LePolainde Warouxetal. (2008) 71 Mean 56—63 50(70.0) NA Mean 25—29% assessed byCMR
31(43.6) 28(39.4) 11(15.5) Sevenpatients:onewithsingle proximalLADstenosis;onewith proximalLADanddistalLCxstenosis; fourwiththree-vesseldisease;one withdominantRCAstenosis Valle-Munoz
etal.(2009)
100 60.4 68(68.0) 33(33.0) 29.1%
assessed byCMR
21(21.0) 24(24.0) 7(7.0) Threepatients:onewith80%stenosis ofthemidLADand70%inthefirst marginalbranch;onewith80%inthe proximalnon-dominantRCAand70% stenosisofthedistalsegmentofthe LCx;onewith70%stenosisofthemid LAD
CMR and HF aetiology 693 Table3(Continued) Study Patients (n) Age (years) Men Diabetes mellitus LVEF Prevalenceof obstructiveCAD Prevalence ofst-LGE Prevalence ofatypical LGE
DescriptionofunderlyingCADin patientswithCADandnost-LGE Krittayaphong etal.(2011) 98 59.4in NIDCMvs 61.5in IDCM 66(67.3) 42(42.9) 32.8%in IDCMvs 27.1%in NIDCM assessed byCMR
58(59.2) 53(54.1) 10(10.2) Fivepatients:noinformationonCAD pattern
Gaoetal.(2012) 124 61 100(80.6) 30(24.2) 26%
assessed byCMR
59(47.6) 67(54.0) 38(30.6) NopatientwithCADandnost-LGE
DiBellaetal. (2016)
187 61 135(72.2) 37(19.8) 37%
assessed byCMR
86(46.0) 83(44.4) 48(25.7) Ninepatients:noinformationonCAD pattern Thompsonatal. (2017) 116 64 90(77.6) NA 40% assessed byCMR
73(62.9) 89(76.7) 15(12.9) Onepatient:totalocclusionofan epicardialvessel,notinvolvingtheLM orLAD Manchuelleetal. (2018) 232 57 184(79.3) 35(15.1) 22.5% assessed byTTE
49(21.1) 49(21.1) 14(6.0) 15patients:11withsinglevessel disease(including50—70%stenosisof thedistalRCA[n=1],midLAD[n=5] andLCx[n=3];80—90%stenosisofthe midRCA[n=2]);threewithtwo-vessel disease(including60%stenosisofthe midLADand50—70%stenosisofthe LCx[n=2];80%stenosisofthemid LADandCTOofthemidRCA[n=1]); onewiththree-vesseldisease(LAD, 90%;LCx,80%;andCTOoftheRCA) Dataareexpressedasnumber(%)unlessotherwiseindicated.CAD:coronaryarterydisease;CMR:cardiacmagneticresonanceimaging;CTO:chronictotalocclusion;IDCM:ischaemic cardiomyopathyLAD:leftanteriordescendingartery;LCx:leftcircumflexartery;LGE:lategadoliniumenhancement;LM:leftmain coronaryartery;LVEF: leftventricularejection fraction;NA: not available;NIDCM: non-ischaemicdilated cardiomyopathy; RCA:right coronary artery; st-LGE: subendocardialor transmural late gadoliniumenhancement; TTE: transthoracicechocardiography.
694
A.
Manchuelle
et
al.
Table4 Descriptionofthe11studiesincludedinthemeta-analysis.
Study Design Periodof
inclusion Consecutive patients Main inclusion criteria Mainexclusion criteria Techniqueto assessLGE Techniqueto assessunderlying CAD Definitionof obstructive CAD Intervalbetween CADevaluation andCMR McCrohonetal. (2003) Prospective registry NA Yes Clinical presentationof HF,documented LVdilationand dysfunctionby TTEor radionucleotide imaging Suspected infiltrativeheart disease, hypertrophic cardiomyopathy, previous revascu-larization, significantvalve disease,history ofmyocarditis Assessed blindly CAinall patients, assessedblind byasingle cardiologist >50% stenosisof any epicardial vessel 2.2yearsin NIDCMvs 3.4yearsin IDCM Casoloetal. (2006) Retrospective study NA Yes Clinical symptoms, LVEF<40%byTTE andLVdilatation byTTEwith volume>2SDsof thesex/body surfacearea Severe congestive symptoms, previous revascu-larization, significant valvulardisease, hypertrophic cardiomyopathy, infiltrative cardiomyopathy, myocarditis Two operators, blindedto clinical data CAinall patients ≥75% stenosisin atleastone major epicardial vessel Maximum 30days Sorianoetal. (2007) Prospective registry
NA Yes Clinicalevidence
ofHF,LV dysfunction documentedby TTE<50% ACSinprevious3 months, secondarycauses ofHF,including valvedisease, constrictive pericarditis, hypertrophic cardiomyopathy, restrictive cardiomyopathy, myocarditis Two physicians blindedto CAdata CAinall patients, assessedblind byasingle expert ≥50% stenosisof any epicardial vessel 5months
CMR and HF aetiology 695 Table4(Continued)
Study Design Periodof
inclusion Consecutive patients Main inclusion criteria Mainexclusion criteria Techniqueto assessLGE Techniqueto assessunderlying CAD Definitionof obstructive CAD Intervalbetween CADevaluation andCMR Schietingeretal. (2007) Prospective registry NA NA New-onsetHF andLVsystolic dysfunction, symptom duration<3 months Age<18years, knownCAD, previouspositive stresstest, previousACS, previous revascu-larization, valvularheart disease Onereader blindedto allclinical andCA data CAinall patients >50% stenosisof any epicardial vessel 14days LePolainde Warouxetal. (2008) Prospective registry NA Yes LVEF<50%, referredforHF aetiology Previously established diagnosisofLVSD, haemodynamic instability,atrial fibrillation Onereader blindedto allclinical andCA data CAinall patients >50% stenosisof any epicardial vesselwith diame-ter>1.5mm Maximum1 month Valle-Munoz etal.(2009) Prospective registry
NA Yes Acutenew-onset
HFwithLVSD (LVEF<40%and increased LVEDD>95th percentileon TTE),withno previoushistory ofCAD,noQ wavesonECG andnoclinical dataattimeof diagnosisto suggestCAD Clinicaldata suggesting hypertrophic cardiomyopathy, infiltrativeheart diseaseor myocarditis Two inde-pendent observers; discrepan-cies resolvedby consensus CAperformed byone cardiologist blindedto CMRresults ≥70% stenosisof any epicardial vessel NA
696 A. Manchuelle et al. Table4(Continued)
Study Design Periodof
inclusion Consecutive patients Main inclusion criteria Mainexclusion criteria Techniqueto assessLGE Techniqueto assessunderlying CAD Definitionof obstructive CAD Intervalbetween CADevaluation andCMR Krittayaphong etal.(2011) Prospective registry NA NA Age>30years, historyofHF within6months, LVEF<50%on TTE,CMRor ventriculogram Clinically unstable,history of revasculariza-tion,HFfrom valvularor pericardial causes Experienced cardiologist unawareof CAresults CAinall patients ≥50% stenosisof any epicardial vessel Maximum1 year
Gaoetal.(2012) Prospective registry
NA Yes LVEF ≤35%on
TTE,stablefor3 monthsunder maximal tolerated therapies, referredforICD implantation - Assessed blindbya single expert CAor computed tomography angiography ≥70% stenosisof any epicardial vessel NA DiBellaetal. (2016) Prospective registry June2007 toJanuary 2013 Yes Newly-diagnosed LVdysfunction (LVEF<45%by ambulatoryTTE evaluation)and NYHA≤2 Chestpain, historyofCAD, historyof secondarycauses ofHF(primary valvedisease, constrictive pericarditis, hypertrophic cardiomyopathy, restrictive cardiomyopathy, myocarditis), cardiac hospitalization, atrialfibrillation Consensus ofthree CMRexpert cardiolo-gists CAinall patients ≥50% steno-sisintheLM and/or≥70% inanyother epicardial vessel NA
CMR and HF aetiology 697 Table4(Continued)
Study Design Periodof
inclusion Consecutive patients Main inclusion criteria Mainexclusion criteria Techniqueto assessLGE Techniqueto assessunderlying CAD Definitionof obstructive CAD Intervalbetween CADevaluation andCMR Thompsonatal. (2017) Retrospective study 2006to April2013 NA LVEF<50%or LVEDV≥97mL/m2 onCMRor previousLV dysfunctionon TTE Historyof revascularization Assessed indepen-dentlyof CA Assessed independently ofCMR ≥50% steno-sisintheLM and/or≥70% inanyother epicardial vessel 42days Manchuelleetal. (2018) Retrospective study Feb2005to Nov2016 Yes New-onsetHF withLVEF ≤35% measuredbyTTE ANDnoclinical, electricalor biological evidenceofCAD HistoryofCADor presenceof typicalchest pain, pathologicalQ wavesonECG, troponin elevation Two readers blindedto clinical variables andCA results; consensus withathird if discrepancy CAinall patients;blind reviewofCA bytwo experienced interventional cardiologists; consensus withathirdif discrepancy ≥50% stenosisin any epicardial coronary arterywith diame-ter≥2mm 2days
ACS:acute coronarysyndrome;CA:coronaryangiogram;CAD:coronaryarterydisease; CMR:cardiacmagnetic resonanceimaging; ECG:electrocardiogram;HF: heartfailure;ICD: implantablecardioverterdefibrillator;IDCM:ischaemiccardiomyopathy;LGE:lategadoliniumenhancement;LM:leftmaincoronaryartery;LV:leftventricular;LVEF:leftventricular ejectionfraction;LVEDD;leftventricularend-diastolicdiameter;LVEDV;leftventricularend-diastolicvolume;LVSD:left ventricularsystolicdysfunction;NA:notavailable;NIDCM: non-ischaemicdilatedcardiomyopathy;NYHA:NewYorkHeartAssociation;SD:standarddeviation;TTE:transthoracicechocardiography.
698 A.Manchuelleetal.
TableA.1showstheoverallqualityoftheincludedstudies,
accordingtoQUADAS-2recommendations[17].
Diagnostic
accuracy
of
no
st-LGE
AsshowninTable2,55(falsenegative)patientspresented nost-LGEonCMR, butsignificantCAD;inversely,75 (false positive) patients presented st-LGE on CMR and no CAD. The diagnostic performance of the presence of st-LGE is
summarized in Fig.3, withpooledresults.Sensitivity and specificity were 87% (95% CI 0.80—0.92) and 93% (95% CI 0.89—0.96), respectively. PLR and NLR were 12.91 (95% CI7.70—21.64) and0.14(95% CI0.09—0.22),respectively. According to the Fagan diagram, and using a pre-test probabilityofCAD(prevalenceofthediseaseinthetested population) of25%, thepost-testprobabilityofCAD when st-LGE was present on CMR was 81%, and the post-test probability of CAD when no st-LGE was found on CMR
Figure3. Diagnosticaccuracy ofthe presence of subendocardialor transmural late gadoliniumenhancement on cardiacmagnetic resonanceimagingtodetectcoronaryarterydisease.CI:confidenceinterval;NLR:negativelikelihoodratio;PLR:positivelikelihoodratio.
CMRandHFaetiology 699 was4% (Fig.A.1). When reported in original studies, the
description of theunderlying CAD in the 55patients with significantCADbutnost-LGEonCMRisgiveninTable3.
Discussion
In patients with new-onset systolic HF, CAD is known to be a leading cause, and may have important therapeutic and prognosticimplications [1,19]. In some cases, angina togetherwithelectrocardiogramsigns(Qwaves) makethe diagnosisofCADverylikely;CAisthusrecommended,with theobjectivesofadaptingmedicaltreatmentand identify-ingpatientssuitablefor coronaryarteryrevascularization, both of which may favour the recovery of myocardium contractile function affected by hibernation or stunning
[20,21]andimprovethepatient’scondition andoutcomes
[22].
To date, guidelines propose performing CA in patients with systolic HF in case of angina or when a non-invasive stress test is positive for ischaemia/viability in asymptomaticpatients[1].However,inpractice,the inter-pretation of a non-invasive stress test can be highly challenging in suchpatients withdepressed left ventricu-lar systolicfunction and a remodelledleftventricle [23]. BecausetheaetiologyofsystolicHFhasbeenshowntobe CADinabout 30%ofangina-freepatientswithnoprevious coronaryevent,severalteamsroutinelycontinuetoperform CA,whichisconsideredtobethegoldstandardforassessing underlyingCADinthisspecificsubset[24].
CA is,however, an invasivetechniqueand mayleadto complications—althoughthesearerarewhenno percuta-neouscoronary interventionis performed (<1%in current practice)[25,26].Therefore,severalauthorshaveproposed alternativestrategies forCADdetectionin thesepatients, andCMRhasbeenshowntobeaninterestingtechniquein thiscontext.Inaddition,CMRalsoprovidesuseful informa-tion about cardiac morphology and function. The present study is the largest in the field; it included 232 patients withnew-onsetsystolicHFofunknownaetiology,who under-wentbothCAandCMRevaluationatamedianintervalof2 days,whichistheshortesteverreported.Inprevious liter-ature,thisdelayoftenlastedseveralmonthsoryears,and sometimeswasnotevenavailable[8,10].Inourstudy,the presenceofst-LGEonCMRhadasensitivityof69%,a speci-ficityof92%,aPLRof8.47andanNLRof0.33todetectthe presenceofsignificantunderlyingCAD.
Importantly, and as in previous studies, the definition weusedforsignificantCADmayhaveaffectedourresults; significant CAD was defined, as in most previous litera-ture focusingon CAD [27],as thepresence of a coronary arterystenosis≥50%inanyepicardialvesselwitha diame-terof>2mm.Ourobjectiveherewastonotunderestimate the presenceof underlying CAD by choosingtoo stringent a definition. Of note, all CAs were assessed blind by two experiencedinterventionalcardiologists,andconsensuswas reached witha third in case of discrepancies. Among the 15 patients identified as having no st-LGE but significant CAD in our study, 11 had single-vessel disease (including twowithseverenarrowing[>80%])andfourhadmultivessel CAD.The presenceofasinglemildand/or distalcoronary arterystenosisprobablycannotsolelyexplaintheseverity
andextentoftheleftventriculardysfunctioninsomecases
[21].Indeed,assuggestedbySorianoetal.[10],who pre-viouslyreportedacorrelationbetweentheextentofst-LGE andastandardizeddefinitionofischaemiccardiomyopathy (historyofmyocardialinfarctionand/or coronary revascu-larization;orstenosis≥75%intheleftmaincoronaryartery and/or in the anteriordescending coronary artery before thefirstdiagonalbranch;ortwoormorestenoses≥75%in epicardial coronaryarteries) [19], it could be speculated thatthiswasa fortuitousassociation insomecases. How-ever, beyond the therapeutic and prognostic implications of the presence of a ‘‘real’’ ischaemic cardiomyopathy, we believe that the presence of any CAD may alsocarry relevant individual information for patients with systolic HF (medical treatment, follow-up, prognostic evaluation, etc.).
Todefinitivelyassesswhethertheabsenceofst-LGEcan ruleoutsignificantCAD,wealsoperformedacomprehensive meta-analysisof the previous literature, which reported, overall, veryconsistent results with ourstudy (sensitivity 69vs 87,specificity 92 vs93, PLR8.47 vs 12.9,NLR 0.33 vs0.14).ThedefinitionusedforsignificantobstructiveCAD variedacrossthe11included studies,buttheoneusedin ourstudy wasthe most commonly used(Table 4)[3—12]. Accordingtotheresultsofthismeta-analysis,thepresence ofst-LGEonCMR hadasensitivityof 87%,a specificityof 93%, a PLR of 12.91 and an NLR of 0.14 to detect CAD in patients withsystolic HFof unknown aetiology.Of the 1227includedpatients,55withnost-LGEhad,infact, sig-nificant CAD. PLR (‘‘good at ruling in the disease’’) and NLR (‘‘good at ruling out the disease’’) describethe dis-criminatorypropertiesofpositiveandnegativetestresults, respectively (i.e. the presence or absence of st-LGE). Of note, both likelihood ratios are roughly independent of prevalence rates, and state how many times more likely particulartest resultsareinpatients withdisease thanin thosewithout disease (i.e. CAD). There is consensusthat aPLR>10andanNLR<0.1providehighlyconvincing diag-nosticevidence,whereasaPLR>5andanNLR<0.2provide strongdiagnosticevidence[28].Whenappliedtoourresults, CMRlooksusefulforexcludingsignificantCADinmostcases (NLR 0.14). Interestingly, some authors have additionally suggested that coupling CMR to a stress test or to mag-neticresonancecoronaryangiographymayfurtherimprove itsdiagnosticaccuracyinthiscontext[13].Inthesameway, couplingCMRtoacoronarycomputedtomographyscanmay alsoprovideusefulinformation,andmayoffer,inourview, thebestnon-invasivestrategy[7].
Finally, it should be emphasized that LGE might be related to numerous causes other than CAD, and that LGE discovery on CMR may also carry relevant diagnos-tic(sarcoidosis,inflammatorydisease,etc.)andprognostic informationoutsidethecontextofCAD.Asspecifiedinour Methodssection,wefocusedonst-LGE,whichishighly spe-cificformyocardialinfarctionscar.
Ourstudypopulationbelongstoanobservationalcohort of patients with new-onset HF. Nevertheless, it is the largestseriesincludingpatientswhounderwentboth CMR andCA.Whenfocusingonourmeta-analysis,apublication bias could not be ruled out, as only small-scale studies havefocused onthistopicin thepast. Therefore,studies withlowsensitivity and/or specificity maynot have been
700 A.Manchuelleetal. submittedbyinvestigatorsoracceptedbyeditorsforfutility
reasons.However,Fig.A.2isreassuringregardingthisissue. Thepresenceofst-LGEonCMR hadasensitivityof87% andaspecificityof93%todetectthepresenceofCADina selectedpopulationofpatientswithnew-onsetHFwithLVEF ≤35%andnoclinicaland/orelectricalevidenceofCAD.Our results therefore suggest that CMR is a rathergood non-invasivealternative tothesystematic useof CAin sucha population.However,CMRwasunabletodetectsignificant CAD in a few cases, and couplingCMR to magnetic reso-nanceangiographyortoacoronarycomputedtomography scanmayfurtherimprovediagnosticperformance.Ourdata andthecost-effectivenessofthisapproachshould,however, beconfirmedinalargercohortofpatients.
Funding
Thisresearchdidnotreceiveanyspecificgrantfromfunding agenciesinthepublic,commercialornot-for-profitsectors.
Appendix
A.
Supplementary
data
Supplementary data associated with this article can be found, in the online version, at https://doi.org/10.
1016/j.acvd.2018.04.004.
Disclosure
of
interest
Theauthorsdeclarethattheyhavenocompetinginterest.
References
[1]PonikowskiP,VoorsAA,AnkerSD,etal.2016ESCGuidelines for thediagnosis and treatmentofacute and chronic heart failure: The Task Forcefor the diagnosis and treatmentof acute and chronic heart failure of theEuropean Societyof Cardiology(ESC).Developedwiththespecialcontributionof theHeart FailureAssociation (HFA)oftheESC.EurHeart J 2016;37:2129—200.
[2]AljizeeriA,SulaimanA,AlhulaimiN,AlsaileekA,Al-MallahMH. Cardiacmagneticresonanceimaginginheartfailure:wherethe alphabetbegins!HeartFailRev2017;22:385—99.
[3]Casolo G, Minneci S, Manta R, et al. Identification of the ischemicetiologyofheartfailurebycardiovascularmagnetic resonance imaging: diagnostic accuracy of late gadolinium enhancement.AmHeartJ2006;151:101—8.
[4]Di Bella G, Pingitore A, Piaggi P, et al. Usefulness of late gadoliniumenhancementMRIcombinedwithstressimagingin predictivesignificantcoronarystenosisinnew-diagnosedleft ventriculardysfunction.IntJCardiol2016;224:337—42. [5]GaoP,YeeR, GulaL,etal. Predictionofarrhythmicevents
in ischemic and dilated cardiomyopathy patients referred for implantable cardiac defibrillator: evaluation ofmultiple scar quantification measures for late gadolinium enhance-ment magnetic resonance imaging. Circ Cardiovasc Imaging 2012;5:448—56.
[6]KrittayaphongR,BoonyasirinantT,SaiviroonpornP, Udompun-turakS.Lategadoliniumenhancementfromcardiacmagnetic resonanceinischemicandnon-ischemiccardiomyopathy.JMed AssocThai2011;94(Suppl1):S33—8.
[7]le Polain de Waroux JB, Pouleur AC, Goffinet C, Pas-quet A, Vanoverschelde JL, Gerber BL. Combined coronary and late-enhanced multidetector-computed tomography for delineation of the etiology of left ventricular dysfunction: comparisonwithcoronaryangiographyandcontrast-enhanced cardiac magnetic resonance imaging. Eur Heart J 2008;29: 2544—51.
[8]McCrohon JA,Moon JC, PrasadSK, et al. Differentiation of heartfailurerelatedtodilatedcardiomyopathyandcoronary arterydiseaseusinggadolinium-enhancedcardiovascular mag-neticresonance.Circulation2003;108:54—9.
[9]SchietingerBJ,VorosS,IsbellDC,MeyerCH,ChristopherJM, KramerCM.Canlategadoliniumenhancementby cardiovascu-larmagneticresonanceidentifycoronaryarterydiseaseasthe etiologyofnewonsetcongestiveheartfailure?IntJCardiovasc Imaging2007;23:595—602.
[10]Soriano CJ, Ridocci F, Estornell J, et al. Late gadolinium-enhanced cardiovascular magnetic resonance identifies patients with standardized definition of ischemic car-diomyopathy: a single centre experience. Int J Cardiol 2007;116:167—73.
[11]ThompsonAC,CrilleyJG,WilsonDW,HunginAP,FuatA,Murphy JJ.Reliableexclusionofprognosticallysignificantcoronary dis-easeinleftventriculardysfunctionbycardiacMRI.ClinRadiol 2017;72:159—64.
[12]Valle-Munoz A, Estornell-Erill J, Soriano-Navarro CJ, et al. Late gadolinium enhancement-cardiovascular magnetic res-onance identifies coronary artery disease as the aetiol-ogy of left ventricular dysfunction in acute new-onset congestive heart failure. Eur J Echocardiogr 2009;10: 968—74.
[13]Assomull RG, Shakespeare C, Kalra PR, et al. Role of car-diovascularmagnetic resonance asa gatekeeper toinvasive coronaryangiographyinpatientspresentingwithheartfailure ofunknownetiology.Circulation2011;124:1351—60.
[14]WonE,Donnino R,SrichaiMB,etal.Diagnosticaccuracy of cardiacmagneticresonanceimagingintheevaluationofnewly diagnosedheartfailurewithreducedleftventricularejection fraction.AmJCardiol2015;116:1082—7.
[15]DiazRA,Nihoyannopoulos P,Athanassopoulos G,Oakley CM. Usefulnessof echocardiographytodifferentiatedilated car-diomyopathyfromcoronary-inducedcongestiveheartfailure. AmJCardiol1991;68:1224—7.
[16]SatohH,SanoM,SuwaK,etal.Distributionoflategadolinium enhancement in various types of cardiomyopathies: signifi-canceindifferentialdiagnosis,clinicalfeaturesandprognosis. WorldJCardiol2014;6:585—601.
[17]Whiting PF, Rutjes AW, Westwood ME, et al. QUADAS-2: a revisedtoolforthequalityassessmentofdiagnosticaccuracy studies.AnnInternMed2011;155:529—36.
[18]Moher D, Cook DJ, Eastwood S, Olkin I, Rennie D, Stroup DF.Improvingthequalityofreportsofmeta-analysesof ran-domisedcontrolledtrials:theQUOROMstatement.Qualityof reportingofmeta-analyses.Lancet1999;354:1896—900. [19]FelkerGM,ShawLK,O’ConnorCM.Astandardizeddefinition
ofischemiccardiomyopathyforuseinclinicalresearch.JAm CollCardiol2002;39:210—8.
[20]WijnsW,VatnerSF,CamiciPG.Hibernatingmyocardium.NEngl JMed1998;339:173—81.
[21]Elsasser A, Schlepper M, Klovekorn WP, et al. Hibernating myocardium:anincompleteadaptationtoischemia. Circula-tion1997;96:2920—31.
[22]CarsonP,WertheimerJ,MillerA,etal.TheSTICHtrial(Surgical TreatmentforIschemicHeartFailure):mode-of-deathresults. JACCHeartFail2013;1:400—8.
[23]Sicari R, Nihoyannopoulos P, Evangelista A, et al. Stress EchocardiographyExpertConsensusStatement–Executive
Sum-CMRandHFaetiology 701 mary: European Association of Echocardiography (EAE) (a
registeredbranchoftheESC).EurHeartJ2009;30:278—89. [24] SilvaF,BorgesT,RibeiroA,etal.Heartfailurewithreduced
ejectionfraction:shouldwesubmitpatientswithoutanginato coronaryangiography?IntJCardiol2015;190:131—2. [25] LimMJ,WhiteCJ.Coronaryangiographyisthegoldstandard
forpatientswithsignificantleftventriculardysfunction.Prog CardiovascDis2013;55:504—8.
[26] WestR,EllisG,BrooksN,JointAuditCommitteeoftheBritish Cardiac S, Royal College of Physicians of L. Complications of diagnostic cardiac catheterisation: results from a
confi-dential inquiry into cardiac catheter complications. Heart 2006;92:810—4.
[27]Lemesle G, Tricot O, Meurice T, et al. Incident myocar-dialinfarctionand verylatestentthrombosis inoutpatients with stable coronary artery disease. J Am Coll Cardiol 2017;69:2149—56.
[28]JaeschkeR,GuyattGH,SackettDL.Users’guidestothe medi-calliterature.III.Howtouseanarticleaboutadiagnostictest. B.Whataretheresultsandwilltheyhelpmeincaringformy patients?TheEvidence-BasedMedicineWorkingGroup.JAMA 1994;271:703—7.

![Table A.1 shows the overall quality of the included studies, according to QUADAS-2 recommendations [17].](https://thumb-eu.123doks.com/thumbv2/123doknet/5471597.129910/13.918.114.817.304.1096/table-overall-quality-included-studies-according-quadas-recommendations.webp)
