Importance of suppression and mitigation measures in managing COVID-19 outbreaks
Texte intégral
Figure

Documents relatifs
• As noted above, for countries experiencing community transmission, there is little rationale for more stringent measures imposed on travellers arriving from countries with lower
Figure 2: The trend of COVID-19 confirmed cases and recovered cases in Ukraine based on COVID-19 and population datasets.. We assume that morbidity by novel coronavirus infection
We analyze an epidemic model on a network consisting of susceptible- infected-recovered equations at the nodes coupled by diffusion using a graph Laplacian.. We introduce an
The fraction of reported cases, from date τ 3 to date τ f , the fraction of reported cases f was assumed increase linearly to reach the value 200% of its initial one and the fraction
COMOKIT combines models of person-to-person and environmental transmission, a model of individual epidemiological status evolution, an agenda-based 1-h time step model of
[5] studied a SIRS model epidemic with nonlinear incidence rate and provided analytic results regarding the invariant density of the solution.. In addition, Rudnicki [33] studied
The model was successfully applied to total cases for the completed COVID-19 epidemic in China (January to April 2020) – and to numbers of reported deaths in the U.S.. Here we
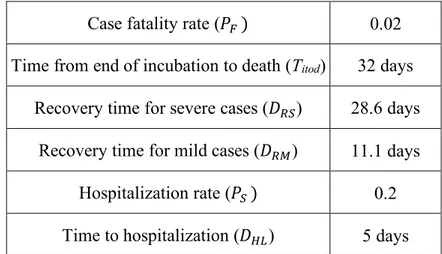
On the other hand, one needs additional information on the infection fatality ratio (i.e., the proportion of infected individuals who die eventually) and on the distribution of
