Biocompatibility, bone healing, and safety evaluation
in rabbits with an IlluminOss bone stabilization system
The MIT Faculty has made this article openly available.
Please share
how this access benefits you. Your story matters.
Citation
McSweeney, Amanda L. et al. "Biocompatibility, bone healing, and
safety evaluation in rabbits with an IlluminOss bone stabilization
system." Journal of Orthopaedic Research 35,10 (February 2017):
2181–2190 © 2017 Orthopaedic Research Society
As Published
http://dx.doi.org/10.1002/jor.23532
Publisher
Wiley
Version
Author's final manuscript
Citable link
https://hdl.handle.net/1721.1/122656
Terms of Use
Creative Commons Attribution-Noncommercial-Share Alike
Biocompatibility, Bone Healing, and Safety Evaluation in Rabbits
with an IlluminOss Bone Stabilization System
Amanda L. McSweeney1,*,+, Brett G. Zani1,+, Rose Baird1, James R.L. Stanley1, Alison
Hayward1, Peter M. Markham1, Gregory A. Kopia2, Elazer R. Edelman3, and Robert Rabiner4
1Concord Biomedical Sciences and Emerging Technologies, 500 Shire Way, Lexington, MA 02421 2Kopia Consulting, 61-4D Taurus Drive Hillsborough, NJ 08844
3Institute for Medical and Engineering Science, Massachusetts Institute of Technology, E25, 45 Carleton St., Cambridge, MA, 02139
4IlluminOss Medical Inc., 993 Waterman Ave., East Providence, RI 02914
Abstract
Bone healing, biocompatibility, and safety employing the IlluminOss System (IS), comprised of an inflatable balloon filled with photopolymerizable liquid monomer, was evaluated in New Zealand white rabbits. Successful bone healing and callus remodeling over 6 months was demonstrated radiologically and histologically with IS implants in fenestrated femoral cortices. Biocompatibility was demonstrated with IS implants in brushed, flushed femoral intramedullary spaces, eliciting no adverse, local or systemic responses and with similar biocompatibility to K-wires in contralateral femurs up to 1 year post-implant. Lastly simulated clinical failures demonstrated the safety of IS implants up to 1 year in the presence of liquid or polymerized polymer within the intramedullary space. Polymerized material displayed cortical bone and vasculature effects comparable to mechanical disruption of the endosteum. In the clinically unlikely scenario with no remediation or polymerization, a high dose monomer injection resulted in marked necrosis of cortical bone, as well as associated vasculature, endosteum, and bone marrow. Overall, when polymerized and hardened within bone intramedullary spaces, this light curable monomer system may provide a safe and effective method for fracture stabilization.
Graphical Abstract
*Author to whom all correspondence should be addressed: Amanda L. McSweeney, BS, RLATG, SRS, CBSET, Inc., 500 Shire
Way, Lexington, MA 02421, Phone: 781-541-5567, [email protected]. +Amanda L. McSweeney and Brett G. Zani contributed equally as first authors.
HHS Public Access
Author manuscript
J Orthop Res
. Author manuscript; available in PMC 2018 October 01.Published in final edited form as:
J Orthop Res. 2017 October ; 35(10): 2181–2190. doi:10.1002/jor.23532.
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
The IlluminOss System employs an inflatable balloon infused with a photopolymerizable liquid monomer that was utilized within the femoral intramedullary spaces of NZW rabbits and evaluated for bone healing, biocompatibility, and safety. When polymerized and hardened within bone intramedullary spaces, this system may provide a safe and effective method for fracture stabilization.
Keywords
Fracture stabilization; light-curable; intramedullary; biocompatibility; polymer
INTRODUCTION
Bone fracture stabilization with splints, casts, metal fixator plates, or intramedullary (IM) rods promote fracture healing by controlling bone movement and alignment.1 A critical balance must be attained to allow some motion to promote normal healing, but not sufficient to create instability leading to non-union.2 Each degree of invasiveness adds to assurance of fixation, but raises complications. The extramedullary periosteal application of plates, indicated where anatomic reduction and stabilization cannot be maintained with simpler techniques, provides greater fracture fixation immediately after reduction and earlier return to motion. However, plating and screw fixations are time consuming, require a greater amount of soft tissue dissection and have significant complications3 that include plate prominence which may result in pain, as well as the potential for infection and tendon adhesions, and a higher incidence of symptomatic fibrous unions or non-unions.4–5
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
Furthermore, plates are usually removed after the fracture has healed requiring additional surgery. IM rods have certain advantages over plates and screws including lower bending forces, making failure by fatigue less likely.6 Percutaneous IM fixation may be an ideal way to stabilize proximal and distal articular extension fractures.7 Current devices, however, are associated with various complications including delayed union, device displacement, and nerve impingement.3; 8–14 Additionally, IM nails typically provide no rotational stability and require additional locking screws.
A new percutaneous photodynamic balloon stabilization system, IlluminOss System (IS), has been developed involving the delivery of a non-compliant polyethylene terephthalate (PET) balloon into the medullary canal (MC) spanning the fracture site, and the infusion of a photopolymerizable liquid monomer within the balloon. Through the infusion of the
monomer, the balloon expands and fills the medullary canal, conforming to the unique geometry of a patient’s bone. Once the light source is activated, the monomer hardens and creates a stable fixation system,15 with a modulus of elasticity similar to that of bone. The implant provides the requisite amount of strength to stabilize the fracture, while the irregular shape of the implant within the canal provides rotational stability. Additional hardware (pins and screws) may then be used in any desired location to add further fracture stability. This new system has been used successfully to clinically stabilize fractures in low-load bearing bones15–16, and prior preclinical studies in sheep have demonstrated feasibility of the IS for fracture fixation in high load-bearing tibiae.17 Here we sought to gain a better understanding of the local and systemic biocompatibility, bone healing, and safety characteristics of monomeric and polymeric material of the IS in high load-bearing rabbit femurs.
MATERIALS AND METHODS
Animal Model
Studies were conducted under approved Institutional Animal Care and Use Committee (IACUC) protocols at Rhode Island Hospital, Providence, RI and Concord Biomedical Sciences and Emerging Technologies, Lexington, MA. Skeletally mature (≥26 week-old), female, New Zealand White rabbits were maintained under environmental controls consistent with the Guide for the Care and Use of Laboratory Animals and fed ad libitum commercial rabbit chow. Animals were anesthetized with ketamine (25–35 mg/kg) and medetomidine/xylazine (0.5mg/kg or 1–5mg/kg respectively) and maintained on isoflurane. Cefazolin (20–30mg/kg) was administered prior to surgery and for the subsequent 24 hours. Analgesia was provided with fentanyl (0.01mg/kg, 25mcg/hr transdermal patch) and carprofen (4mg/kg) for 3–4 days. Treatments and evaluations are summarized in Table 1. Local & Systemic Biocompatibility
A medial parapatellar incision was made over the anterior surface of the left or right knee and the patella and patellar tendon were retracted laterally exposing the intercondylar groove of the distal femoral condyle. Drill sites were created with an awl and a 4.0 mm hole was drilled and subsequently over-drilled with a 5 mm bit into the femoral IM canal from the intercondylar groove. The IM canal was cleaned with a stainless steel spiral brush and saline flushed. For local and systemic biocompatibility evaluations, the implant end of the IS was
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
inserted into the prepared left femoral canal, then filled through the use of a syringe with photo-reactive monomer. Once pressurized, 436 nm wavelength light (generated by an IS light source and delivered via a fiber optic light pipe built into the catheter) was applied for 200 seconds to polymerize the monomer. After curing, the catheter was separated from the cured implant. Following implant, the distal femur hole was filled with bone wax.
Subcutaneous soft tissues and skin were closed in layers using suture. In local
biocompatibility evaluations only, two 1.6 mm diameter titanium K-wires were cut to length, bent slightly to prevent backing out after insertion, and inserted into the right femoral IM canal via the intercondylar drill hole. After wound closure, hind limbs were radiographed, then again prior to euthanasia. Animals were euthanized at 1, 4, 12, 26 or 52 weeks postoperatively.
Femurs and blood samples were collected for analysis. Additional tissues (i.e., ipsilateral popliteal lymph node, ovaries, adrenal gland, spleen, kidney, pancreas, mesentery, heart, and sections of liver, thymus, and lungs) from all systemic biocompatibility group animals were collected and fixed in 10% formalin. Femurs were processed, embedded in Technovit 7200, sectioned, milled, and stained with hematoxylin and eosin (H&E). All tissues were
processed using standard techniques and H&E stained. Bone Healing
After similar fenestration, as described in the biocompatibility evaluations, only the right femoral IM canal was cleaned with a stainless steel spiral brush and saline flushed. A second incision was made over the lateral aspect of the thigh and the femur exposed. An integral drill guide was secured around the femoral diaphysis 40 mm proximal to the distal end of the femur to create three 1.5 mm holes through the anterolateral aspect of the diaphyseal cortex immediately adjacent to one another. These holes were joined by careful removal of the intervening bone with a small osteotome. The resulting defect was ~1.5 mm wide × 4.5 mm long, oriented perpendicular to the long axis of the femur. The IS was implanted into the prepared femoral canal, as described above. Radiographs were collected following wound closure then again prior to euthanasia. Animals were euthanized at 4, 8, 12, or 26 weeks postoperatively.
Femurs and blood samples were collected for analysis. Implanted and naïve femurs were collected and fixed in 10% formalin, then subsequently underwent µCT scanning. High-resolution (30µm isometric voxel size) volume images were generated of a ~30 mm section of the femoral diaphysis centered on the defect site using a micro-computed tomographic imaging system (µCT 40, Scanco Medical AG, Brütisellen, Ch). The scanning yielded 1024 × 1024 grayscale cross-sectional images, which were segmented via simple thresholding (Th=250) and reconstructed to yield three-dimensional volume images. Defect filling was evaluated via inspection of the slice images, as well as the rendered volume images. Femurs were processed, embedded in Technovit 7200, sectioned, milled, and H&E stained.
Device Safety
In Groups 1 and 4, the MC was approached at the hip via the third femur trochanter and a 16 g needle inserted. Marrow was aspirated with an 18 g × 3.5 inch spinal needle advanced to
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
the distal femur. Monomer or saline was administered to the MC while withdrawing the spinal needle. The residual hole in the femur was plugged with a small diameter titanium screw. Skin was closed over the wound using liquid bandage.
In Groups 2, 3, and 5 the knee joint was exposed via a parapatellar incision followed by drilling retrograde into the MC at the center of the trochlear groove of the distal femur using a 4.0 mm drill bit. The MC was cleaned with a stainless steel wire brush and flushed/ aspirated repeatedly with sterile saline. To simulate a clinical failure, Groups 2 and 3 employed a 4 × 30 mm fenestrated balloon and catheter advanced into the MC, then 5 mL of monomer was used to expand the balloon. The presence of the fenestrations allowed for leakage of infused liquid monomer into the MC. For Group 2, the delivered 5 mL was immediately withdrawn after administration, the balloon catheter removed from the femur, and the canal repeatedly cleaned with saline flushes, suction, and swabbing with sterile cotton applicators to simulate remediation. For Group 3, following monomer administration, the catheter light source was activated for a total of 400 seconds in two 200-second curing cycles to polymerize the polymer. The catheter was cut at the point of entry to the femur. For Group 5, no treatment was applied following repeated saline aspiration of the MC. Bone wax was applied in all three groups to close the hole in the femoral trochlea, deep tissues were closed with suture and the skin incision was sealed with liquid bandage. The hind limbs were wrapped with vet wrap or similar material to limit swelling. Animals were euthanized at 1, 4, 13, 26, or 52 weeks postoperatively.
Femurs and blood samples were collected for analysis. Additional tissues including the lungs, skin/subcutis of the proximal femur access site, stifle joint capsule of the distal femur access site, and tissues with macroscopic findings were collected and placed in 10% NBF. High resolution radiographs (Faxitron X-Ray Corporation®) were obtained of all fixed treated femurs prior to processing/trimming. Femurs were decalcified for histological analysis. Femurs for Groups 1, 2, 4, 5 and 6 and two randomly selected contralateral femurs from each treated group at each time point were paraffin embedded whereas Group 3 was resin embedded; all were H&E stained for qualitative analysis. Sections were taken through each femur, one each at the proximal metaphysis, proximal, mid- and distal diaphysis, and distal metaphysis. Treated femurs were assessed for cortical bone necrosis, cortical vascular necrosis, endosteum loss, endosteum necrosis, inflammation and new bone formation. Histopathological scoring of parameters reflecting the degree and extent of the host response/repair process to the treatment included but were not limited to inflammation, necrosis, and vascularity. All lung lobes were systematically sampled, processed, and H&E stained and assessed to evaluate the effects of potential embolization of liberated adipose/fat emboli or free, unpolymerized liquid monomer.
Statistical Analysis
Data were reported as means ± standard deviations (SD). Statistical tests of continuous variables were conducted using statistical functions in SigmaPlot 11.0 (Systat Software, Inc., San Jose, CA) and a p-value ≤ 0.05 was considered significant. Clinical pathology and body weight changes from baseline were analyzed using a Kruskal-Wallis test (using a Monte Carlo approximation).
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
Summary of data for histologic parameters are presented as scoring results per recovery interval in a descriptive statistics format (mean and standard deviation scores) to allow qualitative comparisons between groups without statistical analysis. Histopathologic scoring of parameters reflecting the degree and extent of the host response/repair process to the treatment included but were not limited to inflammation, necrosis and vascularity. For biocompatibility and bone healing evaluations, a severity score was employed based upon the scale of “1” = minimal, “2” = mild, “3” = moderate and “4”= marked. For safety evaluations, findings were graded as follows: 0= Absent; 1 = Minimal feature/presence in the tissue; 2 = Notable (mild to moderate) feature/presence in the tissue; 3 = Prominent to overwhelming (marked/severe) feature/presence in the tissue.
RESULTS
Local & Systemic Biocompatibility
Implanted IS and K-wires did not adversely affect hematological, biochemical, or coagulation parameters (Tables 2 and S1). Statistical differences were observed between several parameters; however, these were not considered clinically significant as values were within the normal reference ranges for rabbits or were considered due to experimental procedure.
Gross necropsy findings were unremarkable and there were no systemic pathological changes noted on any harvested organ. Radiographic inspection showed K-wires retained in femurs for local biocompatibility and the IS retained in femurs in local and systemic biocompatibility evaluations (Fig. 1), as evidenced by the small radiopaque balloon-tip marker centered in the proximal MC, revealing no evidence of device migration. Histologically at 1 and 4 weeks, K-wires induced minimal increase in remodeling of the inner margin in cortical bone, with minimal to mild inflammation in the medulla, while the IS was tightly apposed to the endosteal surface of cortical bone with minimal to mild mesenchymal reaction between the implant and cortical bone and minimal medullar
inflammation. At 12 weeks, both K-wires and IS induced minimal increases in lamellar bone along the junction of cortical bone and bone marrow. In femoral medulla, there was minimal increase in fibrous connective tissue along the bone marrow-device interface for both devices. At 26 weeks, K-wires and IS induced a minimal increase in fibrous connective tissue, forming a narrow, discontinuous band along the device. At 52 weeks, K-wires induced minimal increases in mature lamellar bone, extending from the inner cortical surface around the device and located within the medulla. The IS was tightly apposed to the endosteal surface of cortical bone (Fig. 2). Neither implant was associated with a significant tissue reaction.
Bone Healing
Implanted IS did not adversely affect hematological, biochemical, or coagulation parameters (Tables 3 and S2). Statistical differences were observed between several parameters; however, these were not considered clinically significant as the values were within the normal reference ranges for the species or were considered due to experimental procedure.
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
Radiographs revealed the IS retained in femurs, as evidenced by the small radiopaque balloon-tip marker centered in the proximal medullary canal (Fig. 3A, B). Gross necropsy findings were unremarkable. The mid-diaphyseal cortical defect was radiographically visible post-operatively and less visible at subsequent time points, suggesting new bone was filling the defect. Gross inspection of explanted bones revealed that the defects healed rapidly, with new bone filling most of the defects by 4 weeks. By 26 weeks new bone completely filled all defects demonstrating progressive callus remodeling.
Histologic evaluation revealed the IS implant tightly apposed to the endosteal surface of cortical bone. At 26 weeks the fracture site consisted largely of normal remodeled lamellar bone. A slight alteration in the orientation of the lamellar bone, consistent in size, location, and shape of the defect was present, consistent with complete healing of the cortical bone (Fig. 3C–F).
Consistent with visual assessments, µCT imaging demonstrated most cortical bone defects were completely bridged with woven bone by 4 weeks, which progressively remodeled through week 26 (Fig. 4). Progressive formation of a periosteal neocortex, and increasing porosity of the original cortical bone, both of which are part of the normal healing and remodeling process was also observed.
Device Safety
There was no radiographic evidence of fractures or calluses for any treated femurs. At 1, 4, 13, 26, and 52 weeks there were variable increases in radiopacity of treated femurs
compared to contralateral controls, which was associated with the degree of bone apposition in treated femurs (S-Fig. 1). Regardless of treatment, variable necrosis of diaphyseal cortical bone was the major finding. However, for treatments that exposed the MC to liquid
monomer and were then immediately remediated via surgical cleaning (Group 2) or
monomer polymerization by exposure to the light source (Group 3), the results (i.e., minimal to mild/moderate cortical necrosis) were comparable to sham procedures (Group 5) at all time points (Fig. 5). Mechanical disruption of vascular endosteum associated with preparation of the MC prior to deployment of an IM fixator was interpreted as the primary cause of cortical necrosis, as previously reported (see discussion), and not transient contact of the MC with monomer.
Unlike Group 2 and 5 treatments, direct monomer injection without remediation (Group 1) resulted in marked cortical necrosis (S-Fig. 2A) as well as associated vasculature,
endosteum, and bone marrow. In addition, unremediated monomer resulted in the presence of minimal to mild intravascular vacuoles in lungs with or without inflammation/infarction (S-Fig. 2B) and resulted in increased primary periosteal bone apposition compared to sham saline injection (Group 4). Regardless of treatment group, including shams, areas of necrotic cortical bone persisted through 52 weeks with evidence of varying degrees of active
remodeling and/or new bone apposition (Fig. 6).
The relative amount of hematopoietic cellular elements populating the residual medullary adipose tissue increased over time, even adjacent to areas of steatitis in the case of Group 1, and was interpreted to be acceptable and comparable among Groups 2–5 by Day 90, and in
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
Group 1 by Day 180. Although the medullary space was decreased in Group 3 due to the presence of the balloon-implant, marrow tissue was occasionally present and exhibited normal hematopoietic cellularity.
There was no evidence of pulmonary inflammation/infarction at any time point in Groups 2– 5 (except for very minimal evidence in Group 3 at 4 weeks) and only rare, intravascular vacuoles at 1 week with none at any other time point (Table S3). Additionally, results for clinical failure scenarios (Group 2 and Group 3) were comparable at all time points, providing evidence that mechanical disruption of endosteum was the common denominator across all three treatment groups. Conversely, injection of free monomer into MC without remediation or polymerization (Group 1) resulted in greater incidence of intravascular vacuoles relative to all other groups with minimal to mild vacuole-associated pulmonary inflammation/infarction (Table S3). However, this effect was mostly limited to 1 week and generally ameliorated by 4 weeks.
Though the exact mechanism observed in bone or lung with free monomer is uncertain, neither the presence of free monomer nor any treatment was found to impede new bone growth (Fig. 7). Apposition of new bone appeared to be the primary response, thereby providing support to compromised femoral cortices while allowing sufficient time for resorption and remodeling of necrotic cortical bone.
DISCUSSION
The percutaneous IS conforms to the unique geometry of a MC when filled with a photopolymerizable liquid monomer, then cured with visible light to form a hardened polymeric implant to optimize stable fixation. Clinical studies using the IS have been successful in low load-bearing bones, such as phalanges, metacarpal, radius, ulna, clavicle, fibula, and humerus.15–16 Prior preclinical studies in sheep have demonstrated feasibility of the IS for fracture fixation in high load-bearing tibiae.17 The goals of these studies were to gain a better understanding of the local and systemic biocompatibility, bone healing, and safety characteristics of the monomeric and polymeric material used in the IS in high load-bearing rabbit femurs.
Local biocompatibility evaluations comparing IS to K-wire implants showed no significant tissue or biochemical reaction associated with either implant, while the IS exhibited systemic biocompatibility with no adverse responses biochemically or in abdominal and thoracic organ tissues over the course of a year. Evaluation of bone healing, after creation of mid-diaphyseal transverse defects, showed the IS was well tolerated in an environment of active bone healing. Since the IS requires IM reaming for implantation, the effects of reaming on bone healing need to be taken into consideration. Reaming of the IM canal is associated with various physiologic effects, such as altering IM pressure and medullary blood flow/supply, fat embolization, autografting, thermal energy generation, release of inflammatory mediators, and in some cases improving fracture healing.18–21 Given the abundant new bone formation and almost complete defect filling by 4 weeks
post-operatively, the data indicate the IS did not adversely impact bone healing. In addition, there was no evidence of local or systemic device-related pathology.
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
For safety evaluations, the use of intentionally fenestrated balloons to deliver monomer to the MCs of rabbit femurs was deemed a suitable pre-clinical model for the potential clinical scenario of liquid monomer leakage during infusion. The monomer is composed of
biocompatible monomers and photo initiators in a proprietary, multifunctional methacrylate that forms a thermoset material. During the curing process this material becomes a cross-linked polymer that permanently retains strength and shape. In the current study, evidence of monomer leakage, immediate remediation procedures (i.e., fenestrated balloon removal with saline lavage/medullary cavity swabbing) or polymerization of monomer resulted in tissue responses comparable to saline lavage/medullary cleaning of sham controls (e.g., minimal to mild/moderate cortical bone necrosis, etc…). Other than rare, focal areas of minimal inflammation associated with leaked monomer, all other adverse effects appeared related to disruption of MC contents (i.e., bone marrow, endosteum and endosteal cortical blood supply) secondary to efforts for balloon deployment or post-leakage remediation. As clinical deployment of the IS requires surgical access to the MC, it was important to understand the impact on cortical bone. Cortical bone necrosis radiating outward from the endosteal surface is a common sequela to surgical manipulation of the MC in long bones (i.e., fracture repair). This pathophysiology has been well discussed in the literature and purported to involve multiple mechanisms including: physical disruption of endosteum and its blood supply18; 22; thermal injury to tissue elements associated with cavity clearing (e.g., irrigation/aspiration, “reaming”, etc.)23; exothermic polymerization of surgical resins (e.g., polymethylmethacrylate or PMMA)18; toxicity to tissue elements related to release of bone resin compounds (e.g., PMMA) or occlusion of cortical (i.e., Haversian) vasculature by intravasated marrow or adipose associated with increased IM pressure related to these procedures.24–26
Similar to other devices requiring surgical manipulation of the MC, cortical bone necrosis was noted. Regardless of treatment group, including shams, the relative amount of necrotic cortical bone created at the initial surgical manipulation persisted throughout with evidence of varying degrees of active remodeling and/or new bone apposition. Generally, early periosteal and/or endosteal apposition of new bone appeared to be the primary response, thereby providing support to compromised femoral cortices while allowing sufficient time for necrotic cortical bone resorption/remodeling. However, as cortical necrosis is an expected result following surgical manipulation/preparation of the MC of long bones, the presence of the IS did not appear to preclude the ability of bone to heal as evidenced by periosteal and/or endosteal apposition of new bone and active, progressive remodeling of necrotic cortical bone.
Less clinically relevant was infusion of liquid monomer, without polymerization or remediation procedures. In the clinic, if the liquid monomer does not cure (uncured monomer displays as white and cured polymer displays as black on an MRI scan) after exposure to visible light, then curing can be attempted again or the monomer can be aspirated through the catheter and replaced. Relative to all other groups, monomer solution alone resulted in increased adverse effects observed in bone, such as marked necrosis of cortical bone/vasculature, endosteum, and bone marrow, as well as the presence of
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
intravascular vacuoles in lungs with inflammation and infarction, which was only rarely observed or absent in other groups.
Proliferation of new bone and/or remodeling of pre-existing cortical bone are other expected sequelae to surgical manipulation of the MC of long bones when introducing various IM fixation devices. The presence and location of new bone apposition (i.e., periosteal versus endosteal) and remodeling of existing cortical bone was used to assess the ability of diaphyseal cortical bone to respond to insults (i.e., necrosis) over time. The presence of the IS did not hinder growth of new bone. By 90 days, removal of necrotic cortical bone with new osteonal compact bone, although minimal, was observed regardless of treatment group, including the group receiving monomer without any remediation. Trabecular bone formation was also noted in treatment groups where bone marrow was removed from the MC, although this was somewhat less in the group receiving monomer without remediation. Over time, the MC was associated with a general filling by a mesenchymal/fibrous tissue. This filling was relatively decreased in the monomer without remediation group.
Pulmonary inflammation/infarction is a potential adverse response associated with surgical manipulation of long bones, primarily associated with liberation and embolization of adipose tissue or liquefied (i.e., “free”) fat, secondary to increased IM pressure, during disruption/removal of bone marrow necessary for implantation of IM fixation
devices.24; 27–28 In addition, rare embolization of liquid phase bone resins (e.g., PMMA) to the lungs have been reported.29–30 As such, rabbit lungs were assessed to evaluate the effects of potential embolization of liberated adipose/fat emboli or free, unpolymerized liquid monomer. Injection of free monomer without remediation notably increased the incidence of intravascular vacuoles and areas of pulmonary inflammation and infarction relative to all other groups. The exact nature and pathophysiology of these changes is uncertain since in the absence of physical manipulation of marrow with concomitant increased IM pressure, the liberation of intact adipocytes seems less likely in animals receiving only liquid monomer. Alternatively, vacuoles could represent droplets of embolized liquid monomer or embolized “free” fat, which may have been liberated following the mass necrosis of bone marrow adipocytes or secondary to toxic or lipolytic effects, which have been associated with non-polymerized monomers/polymers.26; 31
Direct monomer injection was an attempt to examine tissue responses to the monomer alone and as such represents an unlikely clinical situation. The monomer dose delivered to the femoral MC of Group 1 rabbits was four times greater than theoretically possible for a balloon leak of monomer in humans. The effects observed with monomer alone appeared to be consistent with adverse effects associated with polymethyl methacrylate (PMMA), widely used as a bone cement. Though in comparison to PMMA, the exothermic response of the IS material during curing is relatively low with in vitro core temperatures of ~62 °C versus ~77 °C for PMMA.25; 32–33 Regardless, the release of liquid monomer without remediation is an extremely unlikely clinical event and thus would not pose an impediment to the use of the IS.
The monomer used in the IS was generally safe when administered in rabbit femurs. The observed adverse effects were similar to those seen with other current MC devices applied in
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
bone fracture stabilization or bone healing. Overall, when polymerized and hardened within bone IM spaces, this light curable monomer system may provide a biocompatible, safe, and effective method for fracture stabilization and bone healing.
Supplementary Material
Refer to Web version on PubMed Central for supplementary material.
Acknowledgments
The authors thank Rami Tzafriri (CBSET) for reviewing the manuscript. Robert Rabiner is Chief Technical Officer and a member of the board of directors for IlluminOss Medical, Inc. This study was supported in part by National Institutes of Health grant (R01 GM-49039) to Dr. Edelman.
REFERENCES
1. Perren SM. Physical and biological aspects of fracture healing with special reference to internal fixation. Clin Orthop Relat Res. 1979:175–196.
2. Chao EY, Inoue N, Elias JJ, et al. Enhancement of fracture healing by mechanical and surgical intervention. Clin Orthop Relat Res. 1998:S163–S178. [PubMed: 9917637]
3. Singisetti K, Ambedkar M. Nailing versus plating in humerus shaft fractures: a prospective comparative study. Int Orthop. 2009; 34:571–576. [PubMed: 19506868]
4. Aksu N, Gogus A, Kara AN, et al. Complications encountered in proximal humerus fractures treated with locking plate fixation. Acta Orthop Traumatol Turc. 2010; 44:89–96. [PubMed: 20676009] 5. Gorschewsky O, Puetz A, Klakow A, et al. The treatment of proximal humeral fractures with
intramedullary titanium helix wire by 97 patients. Arch Orthop Trauma Surg. 2005; 125:670–675. [PubMed: 16217672]
6. Bucholz, RWHJ., Court-Brown, CM., Tornetta, P., McQueen, MM., Ricci, WM. Rockwood and Green’s Fractures in Adults. 7. Pennsylvania: Lippincott Williams & Wilkins; 2010.
7. Fuchtmeier B, Brockner S, Hente R, et al. The treatment of dislocated humeral head fractures with a new proximal intramedullary nail system. Int Orthop. 2008; 32:759–765. [PubMed: 17598111] 8. Changulani M, Jain UK, Keswani T. Comparison of the use of the humerus intramedullary nail and
dynamic compression plate for the management of diaphyseal fractures of the humerus. A randomised controlled study. Int Orthop. 2007; 31:391–395. [PubMed: 16900354]
9. Koike Y, Komatsuda T, Sato K. Internal fixation of proximal humeral fractures with a Polarus humeral nail. J Orthop Traumatol. 2008; 9:135–139. [PubMed: 19384609]
10. McCormack RG, Brien D, Buckley RE, et al. Fixation of fractures of the shaft of the humerus by dynamic compression plate or intramedullary nail. A prospective, randomised trial. J Bone Joint Surg Br. 2000; 82:336–339. [PubMed: 10813165]
11. Taljanovic MS, Jones MD, Ruth JT, et al. Fracture fixation. Radiographics. 2003; 23:1569–1590. [PubMed: 14615566]
12. Miller NC, Askew AE. Tibia fractures. An overview of evaluation and treatment. Orthop Nurs. 2007; 26:216–223. quiz 224–215. [PubMed: 17882096]
13. Strecker W, Suger G, Kinzl L. [Local complications of intramedullary nailing]. Orthopade. 1996; 25:274–291. [PubMed: 8766665]
14. Bostman O, Varjonen L, Vainionpaa S, et al. Incidence of local complications after intramedullary nailing and after plate fixation of femoral shaft fractures. J Trauma. 1989; 29:639–645. [PubMed: 2724381]
15. Heck S, Gicki S, Rabiner B, et al. Initial clinical experiences with a photodynamic polymer (IlluminOss). Med Review: Journal for Medical Continuing Education Conferences (German). 2012:15–16.
16. Hagenaars T, Van Oijen GW, Roerdink WH, et al. Functional recovery after treatment of extra-articular distal radius fractures in the elderly using the IlluminOss(R) System (IO-Wrist); a
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
multicenter prospective observational study. BMC Musculoskelet Disord. 2016; 17:235. [PubMed: 27233355]
17. Zani BG, Baird R, Stanley JR, et al. Evaluation of an intramedullary bone stabilization system using a light-curable monomer in sheep. J Biomed Mater Res B Appl Biomater. 2016; 104:291– 299. [PubMed: 25772144]
18. Pape HC, Giannoudis P. The biological and physiological effects of intramedullary reaming. J Bone Joint Surg Br. 2007; 89:1421–1426. [PubMed: 17998175]
19. Giannoudis PV, Smith RM, Bellamy MC, et al. Stimulation of the inflammatory system by reamed and unreamed nailing of femoral fractures. An analysis of the second hit. J Bone Joint Surg Br. 1999; 81:356–361. [PubMed: 10204951]
20. Blachut PA, O’Brien PJ, Meek RN, et al. Interlocking intramedullary nailing with and without reaming for the treatment of closed fractures of the tibial shaft. A prospective, randomized study. J Bone Joint Surg Am. 1997; 79:640–646. [PubMed: 9160935]
21. Morley JR, Smith RM, Pape HC, et al. Stimulation of the local femoral inflammatory response to fracture and intramedullary reaming: a preliminary study of the source of the second hit phenomenon. J Bone Joint Surg Br. 2008; 90:393–399. [PubMed: 18310768]
22. Brumback RJ, Virkus WW. Intramedullary nailing of the femur: reamed versus nonreamed. J Am Acad Orthop Surg. 2000; 8:83–90. [PubMed: 10799093]
23. Leunig M, Hertel R. Thermal necrosis after tibial reaming for intramedullary nail fixation. A report of three cases. J Bone Joint Surg Br. 1996; 78:584–587. [PubMed: 8682825]
24. Schult M, Frerichmann U, Schiedel F, et al. Pathophysiology of fat embolism after intramedullary reaming. Eur J Trauma. 2003; 29:68–73.
25. Portigliatti Barbos M, Bacchini B, Balbo C, et al. Reaction of bone to methacrylate: interface remodelling. Acta Orthop Belg. 1991; 57:247–253.
26. Kedjarune U, Charoenworaluk N, Koontongkaew S. Release of methyl methacrylate from heat-cured and autopolymerized resins: cytotoxicity testing related to residual monomer. Aust Dent J. 1999; 44:25–30. [PubMed: 10217017]
27. Lindwer J, Van Den Hooff A. The influence of acrylic cement on the femur of the dog. A histological study. Acta Orthop Scand. 1975; 46:657–671. [PubMed: 1180027]
28. Padovani B, Kasriel O, Brunner P, et al. Pulmonary embolism caused by acrylic cement: a rare complication of percutaneous vertebroplasty. AJNR Am J Neuroradiol. 1999; 20:375–377. [PubMed: 10219399]
29. Tozzi P, Abdelmoumene Y, Corno AF, et al. Management of pulmonary embolism during acrylic vertebroplasty. Ann Thorac Surg. 2002; 74:1706–1708. [PubMed: 12440642]
30. Yoo KY, Jeong SW, Yoon W, et al. Acute respiratory distress syndrome associated with pulmonary cement embolism following percutaneous vertebroplasty with polymethylmethacrylate. Spine (Phila Pa 1976). 2004; 29:E294–E297. [PubMed: 15247590]
31. Willert HG, Ludwig J, Semlitsch M. Reaction of bone to methacrylate after hip arthroplasty: a long-term gross, light microscopic, and scanning electron microscopic study. J Bone Joint Surg Am. 1974; 56:1368–1382. [PubMed: 4433360]
32. Kuehn KD, Ege W, Gopp U. Acrylic bone cements: composition and properties. Orthop Clin North Am. 2005; 36:17–28. [PubMed: 15542119]
33. Lai PL, Chen LH, Chen WJ, et al. Chemical and physical properties of bone cement for vertebroplasty. Biomed J. 2013; 36:162–167. [PubMed: 23989310]
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
Figure 1.
Local and systemic biocompatibility evaluation of K-wires and IS. (A) Local
biocompatibility radiographs, from post-surgery to 52 weeks, demonstrated the presence of both K-wires retained in right femurs and the IS balloon retained in left femurs, as evidenced by the presence of the small radiopaque balloon-tip marker in the proximal medullary canal. (B) Systemic biocompatibility radiographs, from post-surgery to 52 weeks, revealed the presence of the IS balloon retained in left femurs, with no observation of device migration, as evidenced by the presence of the small radiopaque balloon-tip marker centered in the proximal medullary canal.
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
Figure 2.
Histologic evaluation of local biocompatibility with K-wires and IS. (A, B) Low and high magnification of naïve untreated femur. (C, D) Low and high magnification of K-wire treated femur at 1 week. (E, F) Low and high magnification of IS treated femur at 1 Week demonstrating close apposition with the cortical bone. (G, H) Low and high magnification of IS treated femur at 52 weeks demonstrating close apposition with the cortical bone. Neither K-wires or IS were associated with a significant tissue reaction.
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
Figure 3.
Histologic evaluation of bone healing. (A, B) Comparison of acute post-operative (top images) and corresponding post-sacrifice radiographs (bottom images) demonstrating IS presence in the right femur (evidenced by small radiographic balloon-tip marker centered in proximal medullary canal). The mid-diaphyseal cortical defect (white arrows) was clearly visible on Day 0, less so at 4 weeks, and largely indistinguishable at 26 weeks, indicating defect filling with new bone. (C, D) Low and high magnification of right femur at 4 weeks post-defect creation. A wedge of new bone in the cortex is highlighted by white brackets,
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
note the adjacent cortical bone composed of dense, compact osteoid (mature lamellar bone). The new bone is composed of less densely compacted osteoid and greater numbers of osteoblasts/osteoclasts within the matrix. (E, F) Low and high magnification of right femur at 26 weeks post-defect creation. A wedge of new bone in the cortex is highlighted by white brackets, note the healed defect is composed of mature lamellar bone. At both 4 and 26 weeks, the IS lies in close apposition with the cortical bone on the inner surface of the cortex.
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
Figure 4.
µCT evaluation of bone healing; the first column depicts the rendered view of the bone while the remaining columns demonstrate 3 longitudinal slices. Cortical bone defects (yellow brackets) were largely filled with new bone by 4 weeks, which progressively remodeled through 26 weeks. The defects at 4 weeks were in general bridged with woven bone and were completely bridged at 8, 12, and 26 weeks. The images also revealed progressive formation of a periosteal neocortex, and increasing porosity of original cortical bone, both of which are part of the normal healing and remodeling process.
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
Figure 5.
Rabbit cortical bone from safety groups. (A, B) Histologic images of Group 2 femur at Day 30. Note filling of medullary cavity by mesenchymal tissue with trabecular bone formation (black asterisk) and absence of bone marrow elements. (C) Histologic image of Group 3 femur at Day 30. Note central cleared area (black asterisk) consistent with presence of polymerized monomer/balloon (removed during processing). (D) At higher magnification, note monomer filled balloon (black arrows, artifactual folded) with an associated thin fibrous capsule (bracket) and trabecular bone formation (black asterisk) in adjacent bone marrow. (E) Histologic image of Group 5 femur at Day 30. Note filling of medullary cavity by mesenchymal tissue with trabecular bone formation (black asterisk) and absence of bone marrow elements. (F) At higher magnification, note apposition of new periosteal bone (bracket).
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
Figure 6.
Mean trend of diaphyseal cortical bone necrosis in femur from safety groups. Compared to other groups, direct monomer injection via needle without remediation (Group 1) resulted in marked cortical necrosis. Regardless of treatment group, including shams, areas of necrotic cortical bone persisted through 52 weeks with evidence of varying degrees of active remodeling and/or new bone apposition.
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
Figure 7.
Mean trend of new cortical growth and medullary trabecular bone in femur from safety groups. (A) Remodeling of necrotic cortical bone was present in all treated groups at 30 days. By 180 days, remodeling was minimal to mild, regardless of treatment, and generally increased as a function of time, then leveled off by 365 days. (B) Presence of trabecular bone formation in medullary cavity was variable (minimal to mild) and decreased in magnitude after 30 days, regardless of treatment.
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
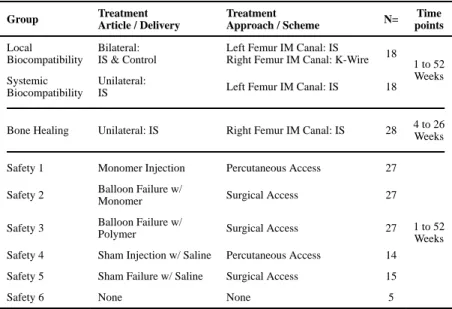
Table 1 Treatment and Evaluation MatrixGroup Treatment Article / Delivery Treatment Approach / Scheme N= Time points Local Biocompatibility Bilateral: IS & Control
Left Femur IM Canal: IS
Right Femur IM Canal: K-Wire 18 1 to 52
Weeks Systemic
Biocompatibility
Unilateral:
IS Left Femur IM Canal: IS 18
Bone Healing Unilateral: IS Right Femur IM Canal: IS 28 4 to 26
Weeks
Safety 1 Monomer Injection Percutaneous Access 27
1 to 52 Weeks
Safety 2 Balloon Failure w/
Monomer Surgical Access 27
Safety 3 Balloon Failure w/
Polymer Surgical Access 27
Safety 4 Sham Injection w/ Saline Percutaneous Access 14
Safety 5 Sham Failure w/ Saline Surgical Access 15
Safety 6 None None 5
Animals were randomly assigned to experimental groups based on the identification number for each animal. Total number of animals allocated per group was determined in order provide a meaningful qualitative and statistical evaluations of each treatment.
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
Table 2Hematology Clinical Chemistry Changes from Baseline for Biocompatibility Evaluations
Analysis Week 4 (n=5) Week 52 (n=10) P-Value
Weight (kg) −0.07 +/− 0.16 0.32 +/− 0.67 0.0007 WBC (th/mm3) −0.30 +/− 0.80 −2.41 +/− 2.20 0.0788 RBC (mi/mm3) −0.05 +/− 0.22 −0.04 +/− 0.78 0.9626 Reticulocytes (%) −0.74 +/− 1.31 −0.25 +/− 1.04 0.0197 Platelets (mm3) 3.20 +/− 47.64 106.33 +/− 83.80 0.1777 HGB (g/Dl) −0.36 +/− 0.42 −0.12 +/− 1.55 0.7565 HCT (%) −0.94 +/− 1.30 −1.38 +/− 5.24 0.7018 ALBUMIN −0.24 +/− 0.18 −0.56 +/− 1.29 0.0080 TOTAL PROTEIN −0.46 +/− 0.22 −0.80 +/− 1.75 0.0462 TOTAL BILIRUBIN 0.02 +/− 0.04 −0.02 +/− 0.06 0.8522 BUN −3.00 +/− 4.06 −1.78 +/− 2.49 0.0650 CREATININE −0.12 +/− 0.08 0.15 +/− 0.23 0.0187 GLUCOSE −4.20 +/− 26.56 15.90 +/− 57.91 0.8067 CALCIUM 0.22 +/− 0.19 −0.11 +/− 0.66 0.0092 PHOSPHOROUS −0.24 +/− 0.75 −1.07 +/− 1.55 0.1341 BICARBONATE 1.20 +/− 2.59 5.40 +/− 7.99 0.0441 CHLORIDE 0.00 +/− 1.58 6.80 +/− 5.33 0.0032 POTASSIUM −0.72 +/− 0.77 −3.71 +/− 7.84 0.0017 SODIUM 0.20 +/− 1.64 6.40 +/− 9.08 0.0007
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
A
uthor Man
uscr
ipt
Table 3Hematology and Clinical Chemistry Changes from Baseline for Bone Healing Evaluations.
Analysis Week 4 (n=6) Week 26 (n=8) P-Value
Weight (kg) 0.02 +/− 0.20 0.61 +/− 0.26 0.0272 WBC (th/mm3) −0.93 +/− 2.71 −0.99 +/− 1.47 0.1325 RBC (mi/mm3) −0.01 +/− 0.88 −0.46 +/− 0.25 0.0027 Reticulocytes (%) 2.08 +/− 1.48 0.35 +/− 1.22 0.0302 Platelets (mm3) 62.50 +/− 164.76 14.86 +/− 39.50 0.1074 HGB (g/dL −0.38 +/− 1.61 −0.58 +/− 0.49 0.0928 HCT (%) 0.07 +/− 5.82 −2.94 +/− 1.92 0.0055 ALBUMIN 0.02 +/− 0.17 −0.24 +/− 0.25 0.0018 TOTAL PROTEIN −0.08 +/− 0.21 −0.16 +/− 0.18 0.0221 TOTAL BILIRUBIN −0.02 +/− 0.04 −0.06 +/− 0.07 <.0001 BUN −1.50 +/− 3.62 −0.75 +/− 2.55 0.0285 CREATININE −0.43 +/− 0.12 0.08 +/− 0.16 0.0014 GLUCOSE 13.33 +/− 39.68 37.75 +/− 41.43 0.1118 CALCIUM −0.07 +/− 0.55 −0.22 +/− 0.47 0.3976 PHOSPHOROUS −0.10 +/− 0.91 −1.55 +/− 1.32 0.1318 BICARBONATE 0.67 +/− 1.37 2.38 +/− 3.07 0.0496 CHLORIDE 2.50 +/− 2.59 6.63 +/− 2.77 0.0019 POTASSIUM −0.03 +/− 0.54 −1.18 +/− 0.84 0.0008 SODIUM 0.33 +/− 2.73 3.75 +/− 1.75 0.0029