Reply to the Letter to the Editor on ‘Severe hepatic sinusoidal obstruction and oxaliplatin-based chemotherapy in patients with metastatic colorectal cancer: a real entity?', by M. Sebagh, M. Plasse, F. Lévi 16: 331)
2
0
0
Texte intégral
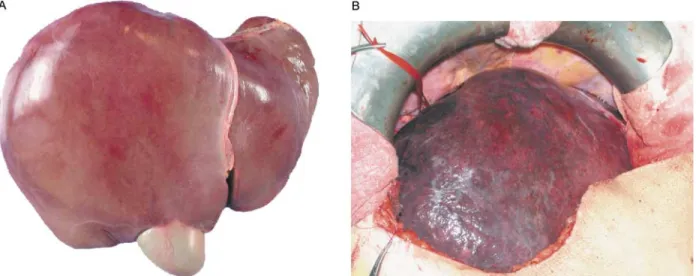
Figure
Documents relatifs
