Current roles for allogeneic hematopoietic cell transplantation following nonmyeloablative or reduced-intensity conditioning.
Texte intégral
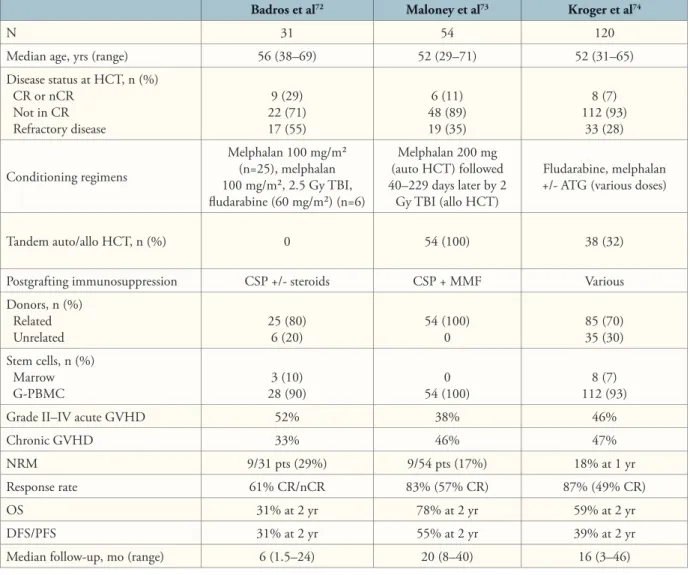
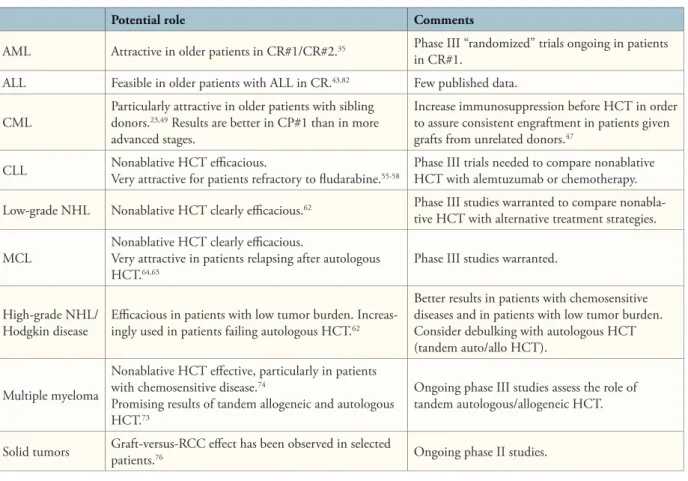
Figure
Documents relatifs
Cassandre Leymarie. Les médiations militantes au sein d’un groupe Facebook : étude de l’organisation d’une action collective entre matérialité de l’objet technique et
This result is in line with those of Werner-Seidler & Moulds (2012). Even if memories mainly concerned relationships in both groups, depressed patients also recalled
Sidorov, Unique representations of real numbers in non-integer bases, Math. Solomyak, Multifractal structure of Bernoulli
L’objectif du cadre théorique de la communauté d’apprentissage est de guider le développement de pédagogies adaptées à la FAD et à l’enseignement hybride, surtout dans
Management variables in function of revenue in intensification groups - Creation of intensification index - Constant farms regarding intensification kept 4 groups of level of
En nous appuyant sur les entretiens mêmes des parents, au moyen d’une analyse qualitative, nous avons tenté d’approcher au plus près le vécu des parents des troubles de leur
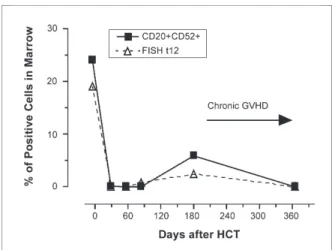
to disappear on satellite images can be calculated as >200 days. The maximum lifetime of such patches on satellite images is
J’adresse mes remerciements aux personnes qui m’ont aidée dans la réalisation du présent mémoire. Je tiens tout d’abord à remercier tout particulièrement ma directrice
