Developing and evaluating a smartphone
application for tuberculosis amongst private sector
academic clinicians in India
Mémoire
Tripti Pande
Maîtrise en Santé Communautaire – Santé mondiale
Maître ès sciences (M. Sc.)
Québec, Canada
Developing and evaluating a smartphone
application for tuberculosis amongst private sector
academic clinicians in India
Mémoire
Tripti Pande
Sous la direction de :
Résumé
Contexte : La tuberculose est la première cause de mortalité au monde et parmi les 10,4
millions de cas de tuberculose par année, 2,8 millions proviennent de l’Inde. De ce fait, il est considéré comme le pays ayant le plus haut taux d’incidence de la tuberculose au monde. Une manque de qualité des soins est une cause majeure pour l’épidémie de la tuberculose en Inde. Le secteur privé, qui n’est pas réglementé, prend soin de 50% des patients ayant la tuberculose. Des études précédentes indiquent le mauvais diagnostic ou le mauvais traitement comme des facteurs qui sont présents dans le secteur privé. Ce secteur comprend plusieurs types de médecins, dont ceux qui ont un diplôme en médecine et ceux qui n’ont pas de diplôme en médecine mais pratiquent la médicine. Une amélioration dans l’éducation des cliniciens utilisant les technologies mobiles, dont les applications mobiles, pourrait être une solution pour améliorer et assurer la qualité des soins des patients ayant la tuberculose. Toutefois, il existe peu d’études sur les technologies mobiles pour la tuberculose en Inde.
Objectifs : Ce mémoire vise à évaluer l’expérience de l’usager et l’acceptabilité d’une
application mobile (LearnTB) parmi les cliniciens académiques du secteur privé en Inde.
Méthodes: L’étude a utilisé une approche à deux étapes. Cinq cliniciens (étape 1) et 101
cliniciens (étape 2) ont été contactés à Kasturba Hospital Manipal, Manipal, Inde entre février et mars 2017. L’expérience des participants était évaluée par le System Usability Scale. L’acceptabilité était évaluée par un questionnaire adopté du Technology Assessment Model. Les résultats étaient analysés à l’aide des statistiques descriptives, la régression linéaire multiple ainsi que la régression logistique.
Résultats : Des taux de réponse de 100% et 99% ont été obtenus pour la première et
deuxième partie respectivement. L’expérience de l’usager était vraiment positive. En ce qui concerne l’acceptabilité, une analyse de cheminement a confirmé la relation directe entre l’utilité perçue et l’intention d’utilisation, et la relation indirecte entre la facilité d’utilisation perçue et l’intention d’utilisation. La régression logistique a permis de cibler les items qui influencent fortement l’intention d’utilisation.
Conclusion : L’expérience de l’usager pour LearnTB était vraiment positive, et l’utilité
perçue a le plus grand impact sur l’intention d’utilisation (acceptabilité). Cette étude permet d’avoir une analyse préliminaire de l’acceptabilité des cliniciens concernant les technologies
mobiles pour la tuberculose en Inde. D’autres recherches dans ce domaine sont requises afin d’assurer l’implantation optimale de ces technologies.
Abstract
Background: Tuberculosis (TB) is the leading infectious killer, and India accounts for 2.8
of the 10.4 million TB cases that occur each year, making it the highest TB burden country worldwide. Poor quality of TB care is a major driver of the epidemic in India. India’s large private, unregulated health sector manages over 50% of the TB patients, with studies showing suboptimal diagnosis and treatment in the private sector. This sector comprises of health professionals who are medically trained, and those who are not medically trained but are practicing medicine. Better education of doctors using mobile health (mHealth) applications is a possible solution. However, little is known about mHealth around TB in India.
Objective: This masters thesis aimed to evaluate the user experience and acceptability of a
smartphone application for TB (LearnTB) amongst private sector academic clinicians in India.
Methods: This study adopted a two part approach. Five clinicians (part 1) and 101 clinicians
(part 2) were contacted at Kasturba Hospital Manipal, Manipal, India between February and March 2017. The user experience of participants (part 1) was evaluated based on the System Usability Scale (SUS). Acceptability (part 2) was evaluated based on the Technology Acceptance Model (TAM). Data were analyzed using descriptive statistics, multiple linear regression as well as logistic regression analysis.
Results: Response rates of 100% and 99% were achieved for part 1 and part 2, respectively.
User experience was very positive. Regarding acceptability, a path analysis confirmed the direct relationship between perceived usefulness and intention to use, and the indirect relationship between perceived ease of use and intention to use. Logistic regression analysis helped target items strongly influencing intention to use.
Conclusion: The user experience with LearnTB was very positive, and perceived usefulness
has the highest impact on intention to use (acceptability). This study provides a preliminary analysis of mHealth interventions for TB in India, and emphasizes the need for future research in this domain.
TABLE OF CONTENTS
Résumé ... iii
Abstract ... v
List of Tables ... viii
List of Figures ... ix
Abbreviations ... x
Acknowledgement ... xi
Avant – propos ... xii
CHAPTER 1 Introduction ... 1
CHAPTER 2 Context ... 5
2.1 General information: Tuberculosis ... 5
2.2 General epidemiology of TB ... 6
2.3 Revised National TB Control Programme (RNTCP) ... 7
2.4 Health portrait of India ... 7
2.4.1 Geographic, demographic and economic context ... 7
2.4.2 Health systems: the increasing gap ... 9
2.5 General information: mHealth ... 10
CHAPTER 3 Theoretical Framework ... 12
CHAPTER 4 Literature review ... 17
4.1 User experience: the importance of usability studies ... 17
4.2 Development of mHealth strategies ... 18
4.3 Acceptability of mHealth interventions ... 19
4.4 Factors influencing adoption of mHealth interventions ... 21
4.5 Knowledge gap & justification ... 22
CHAPTER 5 Research Question and Objectives ... 25
5.1 Question ... 25
5.2 Objectives ... 25
5.3 Hypothesis ... 25
CHAPTER 6 Mobile application ... 26
CHAPTER 7 Methodology ... 29
7.1 Study design ... 29
7.2 Study setting ... 29
7.3 Study population & recruitment ... 30
9.3 Contribution to public health ... 76
CHAPTER 10 Conclusion ... 78
CHAPTER 11 References ... 79
Appendix A : Proof of submission ... 84
Appendix B : Search strategy ... 85
Appendix C : SUS questionnaire ... 86
Appendix D : Tasks for user experience (part 1) ... 88
Appendix E : TAM questionnaire ... 89
List of Tables
Table 1 : Part 1 – Sociodemographic characteristics (n=5) ... 66
Table 2 : Variables and items present in TAM questionnaire (n=100) ... 66
Table 3 : Part 2 – sociodemographic characteristics (n=100) ... 68
Table 4 : Pearson’s correlation coefficients between variables (n=99) ... 69
List of Figures
Figure 1 : Political map of India (source : www.worldmaps.org) ... 8
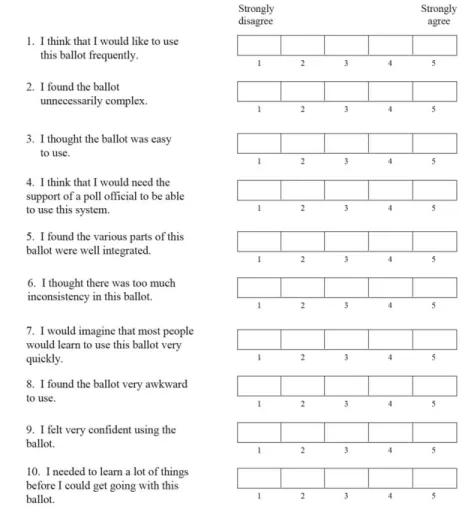
Figure 2: Original 10 statement SUS questionnaire developed by J. Brooke in 1996 ... 13
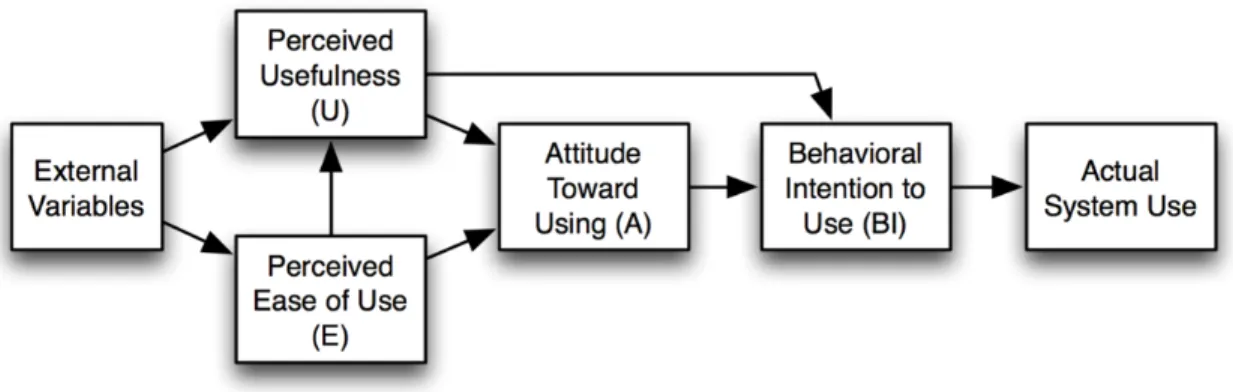
Figure 3: Original Technology Assessment Model (TAM) by Davis 1989 ... 15
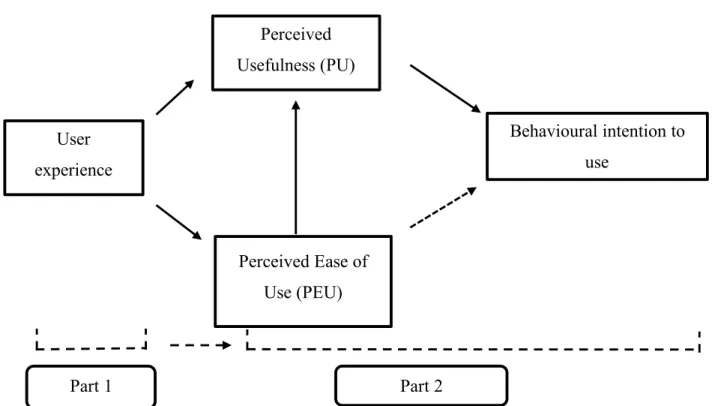
Figure 4: Adapted version of TAM including user experience ... 16
Figure 5: LearnTB application – home page ... 27
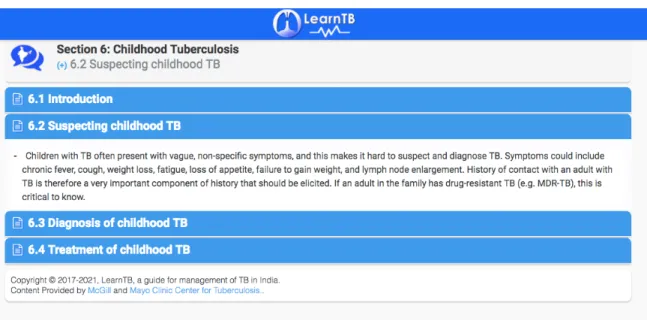
Figure 6: LearnTB application – subsections present in Section 6 “Childhood tuberculosis” ... 27
Figure 7: LearnTB application – figure of chest x-ray in Section 4 “Role of chest x-rays in the management of tuberculosis” ... 28
Abbreviations
BCE: Before common era CE: Common era
CÉRUL: Comité d’éthiques de la recherché avec des êtres humains de l’Université Laval DOI: Diffusion of innovation theory
DOTS: Directly observed treatment short course eHealth: Electronic health
GDP: Gross domestic product HBC: High TB burden country IU: Intention to use
LMIC: Low and middle income country
MBBS: Bachelor of medicine and bachelor of surgery MDR-TB: Multi-drug resistant tuberculosis
mHealth: Mobile health
MUEC : Manipal University ethics committee NAATS: Nucleic acid amplification tests NTP: National tuberculosis program PDA: Personal digital assistants PEU: Perceived ease of use PTB: Pulmonary tuberculosis PU: Perceived usefulness
RNTCP: Revised national tuberculosis control program SMS: Short messaging service
SUS: System usability scale
TAM: Technology assessment model TB : Tuberculosis
Acknowledgement
This thesis project has been brought to its stage today through the TMA Pai Endowment Fund, and the help and support of many key people. Firstly, I would like to thank my supervisor Dr. Marie Pierre Gagnon for her constant support and reassurance throughout the whole entire thesis process. From the day that we had met to discuss my thesis project, you did not cease to help me in any way possible. Your confidence and continuous drive to make me reach my goals has brought me to the stage I am at today; submitting my masters thesis, thank you! I would also like to thank my co-supervisor Dr. Madhukar Pai for his constant push to allow me to reach the heights I did with this thesis project. Your constant encouragement has helped me create new opportunities and achieve the goals I had planned for this thesis project, thank you!
I am grateful to Dr. Zelalem Temesgen and Mr. Al Seyoum for their countless hours allowing the prototype version of the LearnTB application be ready for demonstration in India. I would also like to thank Dr. Kavitha Saravu for being an amazing field supervisor in Manipal. The way you flawlessly integrated me into the hospital environment since the first day I reached India definitely eased the data collection process and helped me reach my sample size goal. Also, a special thank you to Dr. Deekthish Mahadev for your dedication to helping me achieve my target sample size, as well as Dr. Shipra Rai and Dr. Raghavendra Rao for their efforts in participant recruitment.
Thank you to all my friends and colleagues in Manipal for your immense hospitality and easing my stay in India. Many thanks to all the interns, post graduate residents, junior faculty, senior faculty and staff of Kasturba Hospital Manipal for participating in this research study. As I submit this thesis, I would like to thank my family for their immense encouragement during my masters degree. We have gone through it together, and thank you for always being there. Thank you to all my friends who have supported me and shown me the positive side of the situation throughout these two years- special thank you to Johanne and Priscille! Finally, thank you to all my professors for your support and mentorship throughout my academic career, it has helped me reach where I am today. Thank you everyone!
Avant – propos
This masters thesis comprises of one original article titled “Evaluating clinicians’ user
experience and acceptability of LearnTB, a smartphone application for tuberculosis in India”. The primary author of this article is Tripti Pande, and the co-authors include her
thesis supervisor Dr. Marie-Pierre Gagnon, co-supervisor Dr. Madhukar Pai, followed by Dr. Kavitha Saravu, Dr. Zelalem Temesgen, Mr. Al Seyoum, Dr. Shipra Rai, Dr. Raghavendra Rao, Dr. Deekshith Mahadev. Tripti Pande, author of the article and this thesis, designed and conducted the study as well as wrote the manuscript. Drs. Marie-Pierre Gagnon and Madhukar Pai helped design the study and edit the manuscript. Dr. Kavitha Saravu provided field supervision at Kasturba Hospital Manipal, Drs Shipra Rai, Raghavendra Rao and Deekshith Mahadev helped in participant recruitment and data collected at Kasturba Hospital Manipal. Dr. Zelalem Temesgen and Mr. Al Seyoum helped in the development of the
LearnTB application. All co-authors helped finalize the manuscript for submission.
The article has been inserted into Chapter 8 – Manuscript, of this thesis project. A detailed introduction, context and methods section has been presented prior to the article, to help readers understand the need for such a research study. The article presents similar sections, however does not contain as much detail. By presenting a pre-lude to the manuscript, the author hopes that all readers will understand the scientific and social justification for such a research study.
The article was submitted to the mHealth journal on May 9th, 2017 and accepted without revisions on June 27th, 2017 (DOI: 0.21037/mhealth.2017.07.01). The proof of submission is presented in Appendix A.
CHAPTER 1 Introduction
Tuberculosis (TB), caused by Mycobacterium tuberculosis, is an airborne infectious disease known to be the leading infectious disease killer in the world (1). In 2015, the World Health Organization (WHO) reported 10.4 million new cases of TB causing 1.8 million deaths worldwide (2). Furthermore, there is a gap of 4.3 million between incident and notified cases of TB. India, Indonesia and Nigeria account of 50% of this gap (2). There are 30 high TB burden countries in the world (HBCs), composed largely of low- and middle- income countries (LMICs) (3), where India is the highest TB burden country, accounting for 27% (2.8 million) of the world’s TB cases, and 29% of the 1.8 million TB deaths (2).
The End TB strategy, previously proposed by the WHO, had three milestones for 2020 to end TB burden worldwide: 35% reduction in TB deaths, 20% reduction of TB incidence rate and 0% of TB affected families should face catastrophic costs due to treatment (3). These numbers have since been revised to 95%, 90% and 0% respectively for 2035. The current rate of decline of TB is 1.5% (3). To achieve the End TB strategy goals, this rate must increase to 4-5% per year (2).
Scientific studies had previously underestimated the TB incidence rate, due to insufficient data provided by countries (4). India has increased its case notification rate by 34% between 2013 and 2015, allowing an improved estimation of the world wide TB burden (2). Research continues to highlight the constant neglect and mismanagement of TB patients within India’s two prominent health care sectors, the public and private sector, causing the high burden of disease (5, 6).
The public sector is regulated by the Indian government, whereas the private sector is not (7). Over the past 20 years, the private sector has grown from managing 5-10% of the general patient population to 82% (5). Moreover, this sector manages 50% of India’s TB cases and studies have reported patients prefer private clinics as opposed to public clinics. The private sector lacks regulation regarding diagnostic and prescribing practices (8) due to its
“for-profit” nature and the high heterogeneity amongst health care professionals. There are qualified formal doctors, as well as unqualified/informal providers and practitioners of alternative medicine. Nevertheless, patients prefer private sector clinics as they are of closer proximity to vulnerable populations residing in remote rural areas, and there is minimal wait time (8). Studies have shown the increased need to implicate the private sector, especially health care professionals, in TB control interventions throughout India (9). The implication of NIKSHAY, an electronic TB case notification system, has significantly increased the case notification rates in India, due to its presence in the private sector. Between 2013 and 2015 NIKSHAY increased India’s case notification by 34%, which is the largest TB case notification increase worldwide (4). The latter emphasizes the potential of the new era digital technologies in health, especially in the Indian context.
Mobile health (mHealth) is defined as the delivery of health care services and information through the internet and telecommunication technologies (10). It has the potential to play a vital role in delivering health care to remote populations lacking human resources, through the use of mobile phones (10). India is the second highest mobile phone consumer due to its low cost handsets, thus making it an excellent target for such interventions (11). Although there are numerous different types of mHealth interventions, such as personal digital assistants (PDAs), and short messaging service (SMS), mobile applications (smartphone applications) are continuing to increase their market. mHealth is largely consumer driven and previous studies have focused largely on developing mHealth interventions, and evaluating the acceptability of the intervention after diffusion. A systematic review by Iribarren et al. identified a total of 1332 mHealth applications of which 24 focused on TB (patient support, health care provider management, and awareness) (12). Very few applications had been formally studied in usability or acceptability (12). There are few studies on mHealth strategies for TB amongst health care professionals in India and to our knowledge there is no
With this perspective, this study aims to understand the user experience and acceptability of a smartphone application for tuberculosis amongst private sector clinicians in India. The private sector is targeted due to its unregulated nature. Health care professionals practicing in the private sector often do not have the resources (laboratory equipment, lab personnel financial stability) to perform proper diagnosis and treatment of TB. Studies show complicated care seeking pathways, extensive diagnostic delays (13), widespread empirical management (14) and poor adherence to established standard of care in the private sector (15). All factors are largely attributable to the high TB burden present in India today. Clinicians have been chosen as they are an educated population who are in contact with TB patients everyday. They are the target population due to their ability to assure proper diagnostic and treatment methods for TB. TB is chosen as the disease of interest, as it is the highest infectious disease killer in the world, and of highest prevalence in India.
This thesis has been separated into 10 detailed chapters to facilitate understanding. In the first two chapters, the author presents the introduction of the topic and detailed context of tuberculosis in general, mHealth in general, TB burden in India, and mHealth interventions currently in place in India. Subsequently Chapter 3 presents the theoretical frameworks adopted for this thesis project and chapter 4 provides an overview of the existing scientific literature on user experience, developing mHealth interventions, acceptability of mHealth interventions, factors influencing adoption by health professionals and highlights the existing knowledge gap. This chapter is concluded with a scientific and social justification for this thesis project. Chapter 5 presents a structured view of the research question, objectives and hypotheses. The mobile application of interest, LearnTB is presented in detail, with figures, in Chapter 6. Chapter 7 provides an indepth overview of the methodology used to conduct this thesis project, including explanation on the study design, setting, population, methods for data collection, data analysis and ethics approvals obtained. Chapter 8 presents the inserted manuscript. Chapter 9 presents a general overview of the results, highlights study strengths and limits followed by an explanation regarding the thesis’ contribution to public
health. Finally, chapter 10 presents a brief conclusion regarding future recommendations for scientific studies.
CHAPTER 2 Context
This chapter focuses on presenting the general context for both TB and mHealth. It will first explain the etiology and general epidemiology of TB, followed by a section regarding the Revised National Tuberculosis Control Program in India, an initiative assembled in 1997 to facilitate TB control in the public health sector of India. We will then elaborate on the TB burden in India and provide an overview of the two main health sectors in India, the public and private sector. The final section will elaborate on mHealth technologies and their presence around the world. It will mainly focus on providing an overview of the functionalities of mHealth and the different types of mHealth interventions existing worldwide and in India.
2.1 General information: Tuberculosis
Tuberculosis (TB) is an airborne bacterial infection caused by Mycobacterium tuberculosis. Although there are numerous forms of TB such as extra pulmonary TB, military TB, and laryngeal TB; pulmonary TB (PTB) is the most prominent form. Being an airborne disease, TB can be transmitted via cough (16), rendering it to be a highly infectious agent in confined spaces such as overpopulated health care centers and/or hospitals. There are two phases of TB, the latent phase and active phase (16). Approximately 5-10% of individuals infected with TB will progress to active TB cases during their lifetime (16). The remaining cases are known to be latent TB cases. Although the chances of a TB infection progressing from the latent TB phase to the active TB phase are quite minimal, the aggressive nature of the TB infection demands timely diagnosis and adequate treatment.
There are numerous diagnostic tests for TB such as sputum smear microscopy, rapid diagnostic tests, nucleic acid amplification tests (NAATS) as well as liquid and solid cultures (2). Most TB programs use direct sputum smears to confirm TB diagnosis, however the preferred gold standard is microbiological confirmation; liquid or solid culture (17, 18). Regarding the treatment of TB, a 6-month regimen with four first line drugs; rifampicin, isoniazid, ethambutol and pyrazinamide is prescribed (2). Due to lack of treatment adherence amongst patients, the rates of multi-drug resistant TB (MDR-TB) have progressively increased (2), thus leading to the availability of second and third line drug regimens as well.
2.2 General epidemiology of TB
Based on the annual WHO Global TB Report, there were 10.4 million new TB cases worldwide. 60% of these cases emerged from India, Indonesia, China, Nigeria, Pakistan and South Africa (2). Notified TB cases increased by 34% between 2013 and 2015 due to India’s increased case notification system, however a global 4.3 million gap remains between incident and notified cases (2). The largest proportion, 50%, of this gap is due to India, Indonesia and Nigeria. Worldwide, 49 million patients with TB were treated between 2000 and 2015, however significant gaps between diagnostic practices and treatment regimens continue to exist (2). In 2015, approximately 6.1 million TB patients had access to quality care, however 4.3 million patients did not receive proper care. This gap can be closed through better reporting, diagnosis and access to care (4).
India accounts for 27%, 2.8 million, of TB cases worldwide, thus making it the highest TB burden country in the world (4). An estimated 40% of India’s population is infected with TB, however the large majority are in the latent phase (19). TB prevalence is known as the number of active TB cases. In 2015, 1.28 million TB cases were undergoing treatment under the Revised National Tuberculosis Control Programme (RNTCP), however a rate of 111 per 100 000 cases were notified to the RNCTP (public sector) and 184 802 TB cases were notified to the private sector (19). Drug resistant TB rates have drastically increased over the years, leading India to be the country with the second highest multi drug resistant TB (MDR-TB) burden. It accounts for 16% of the estimated 480 000 new cases of MDR-TB (20). TB human immunodeficiency virus (TB-HIV) coinfection is prominent in India as TB is the most common HIV related coinfection (21). Currently, 5% of TB cases in India are co-infected with HIV (21). The TB HIV coinfection is often of higher risk to patients with latent TB disease. In India, every two people out of five (2/5) have latent TB disease, thus increasing their risk of developing TB-HIV coinfection (21). The national budget for TB is USD (United
attributed to numerous factors, including lack of governmental support, lack of management and the disparity between the health care sectors, the public and private sectors.
2.3 Revised National TB Control Programme (RNTCP)
The Revised National Tuberculosis Programme (RNCTP), launched in 1997 by the Government of India under the recommendation of the WHO, aimed to reduce numerous managerial issues such as lack of treatment adherence, non-standard treatment regimens and lack of systematic information on treatment (24). This programme also implemented the Directly Observed Treatment Short-course (DOTS) strategy encouraging patients to take the proper medication and adhere to treatment regimens. The DOTS strategy also provides basic TB diagnosis and treatment to all patients in India (24). Despite the promising nature of the RNCTP strategy, India remains the highest TB burden country in the world due to the disparities amongst the two health care sectors in India, the public and private sector. The RNTCP DOTS strategy is not highly implemented in the Indian private sector.
2.4 Health portrait of India
2.4.1 Geographic, demographic and economic context
India, officially known as the Republic of India, is the second most populated country in the world, with a population of 1.3 billion (22). It is bordered by six different countries; Pakistan, China, Nepal, Bhutan, Bangladesh and Myanmar (23). Its northern mountain range, the Himalayas, define the South Asian sub-continent from the rest of Asia. India is surrounded by bodies of water as well, the Bay of Bengal to the east and the Arabian sea to the west. It is known for its diverse religious and traditional culture. It has a vast history of colonization, starting with the Indus civilization from 2600 – 2000 Before Common Era (BCE), followed by the Muslim rule (Mughal era) in the 8th century Common Era (CE), then the Portuguese lead by Vasco de Gama in 1498 ending with the 200-year British colonization. India gained its independence on August 15th 1947, with 29 states and 6 union territories, and since has been an independent democracy (23). Since independence, India’s economy has been growing substantially, and it now hosts three of the world’s fastest growing high technology
cities; Bangalore, Chennai and Hyderabad (23). The total health expenditure is approximately 4.7% of the Gross Domestic Product (GDP)1 and the gross national income per capita is 5 international dollars (Int’l $)2 (22). Life expectancy at birth is 70 years for females and 67 years for males, which is a healthy life expectancy according to WHO standards (25). Literacy rates has increased to 72.2% (26) since 1951 (18.3%), however the gap remains large between female literacy rates, 54.2% and male literacy rates, 75.9% (27). It is visible that India has improved drastically in numerous aspects since independence and continues to do so, however the TB burden and health care system continues to remain a prominent issue.
2.4.2 Health systems: the increasing gap
There are two main health sectors in India, the government controlled public sector and the growing private sector. The public sector, as mentioned previously, is government controlled and standardized (DOTS) treatment is offered at all public hospitals and clinics (28). The RNTCP increasingly promotes universal access to quality TB diagnosis and treatment for all patients in the community (29). 90% of TB cases are confirmed via positive sputum smears in the public sector, unfortunately this is not so for the private sector (29). As mentioned previously, microbiological confirmation is the preferred international gold standard diagnostic test, however sputum smear is the most commonly used confirmatory diagnostic test (17). The unmanaged and unregulated private sector has grown over the past 20 years. It manages 82% of general patients and 50% of India’s TB population (5). The National Health Survey-3 reported 70% of households in urban areas and 63% of households in rural areas visit the private sector as their primary source of healthcare (30). It is often preferred by TB patients due to social determinants such as distance, accessibility, responsiveness, and opening hours (30). Numerous studies have shown a TB diagnosis-delay of two months, and visits to three health care providers prior to receiving a treatment regimen (31). Additionally, diagnostic techniques are not regulated in the private sector which leads to high cost of reliable diagnostic equipment, and use of unreliable tests, i.e. blood tests (29). Despite one third of the medically trained clinicians practicing in the private sector, there is a discrepancy between what is reported by practitioners and what patients adhere to (32). Furthermore, a large proportion of cases treated in the private sector are often left unreported, thus increasing concern regarding this vastly unregulated sector (28). Private practitioners often do not adhere to treatment regimens that are commissioned by the WHO, and often do not assure treatment completion (33). There is a highly heterogeous population of private practitioners, ranging from formally trained clinicians to informally trained practitioners and alternative medicine practitioners. The inconsistency of care is often due to poor knowledge of TB amongst informally trained practitioners, inaccessibility to proper training as well as inadequate supervision and re-training. In summary, the large discrepancy in management and regulation of the two health care sectors in India is apparent. The numerous lacunas in the private health sector further emphasizes the need for extensive research in this sector, and
increases the need for public private partnerships, which is advocated by numerous studies (31, 34).
2.5 General information: mHealth
Mobile health (mHealth) is defined as the delivery of health care services and information through internet and telecommunication technologies (10). It has the potential to play a vital role in delivering health care to remote populations lacking human resources, through the use of mobile phones (10). mHealth technologies are not limited to mobile phones, they also include; personal digital assistants (PDAs), PDA phones (ie. Blackberry®), smartphones (ie. iPhone), portable media players (ie. MP3s), video-game consoles (ie. Nintendo), and ultra-portable computers (ie. tablets) (35). Such technologies have been gaining popularity over the past decade, due to their low cost interventions (35). mHealth technologies allow users to overcome geographic barriers, as well as personal barriers, such as stigma and loss of privacy (11). Previous studies have shown the rapid growth of mobile communications in low income countries, thus permitting large geographical coverage (35-38). mHealth strategies aim to support health care providers through education, patient management, and support in diagnosis, as they are largely consumer centered and consumer driven (39, 40). Although there is limited evidence on the effectiveness of mHealth, a systematic review conducted by Gagnon et al. identified 33 studies evaluating adoption of mHealth interventions amongst health care professionals. Less than half the studies were conducted on physicians or medical residents and only one study was conducted in India (39).
India is the world’s second largest mobile phone consumer base, due to low cost handsets and affordable calling plans (11). There are approximately 877 million (96%) wireless subscribers in India (41). mHealth and eHealth technologies have been increasing steadily in
Report 2015 (4). Through the introduction of this eHealth platform in both the private and public sectors, the RNTCP has been able to actively engage the private sector in their TB strategies. Between 2013 and 2015, this platform has increased TB case notifications in India by 34%, the largest case notification improvement worldwide (4). The success of this eHealth strategy demonstrates the potential of other eHealth, mHealth, telemedicine or mobile technology interventions to be accepted in the Indian health care environment.
CHAPTER 3 Theoretical Framework
This chapter aims to present the two theoretical frameworks used for this study. To facilitate understanding this research study was separated into two parts; part 1 being a user experience study and part 2 being an acceptability study.
To ensure understanding of terms used in our study, the following definitions have been listed:
- Acceptability: intention to use
- Clinician: resident doctors and academic clinicians practicing at Kasturba Hospital Manipal (Manipal University)
- Mobile application: smartphone applications only - Usability: used as a proxy for user experience
PART 1:
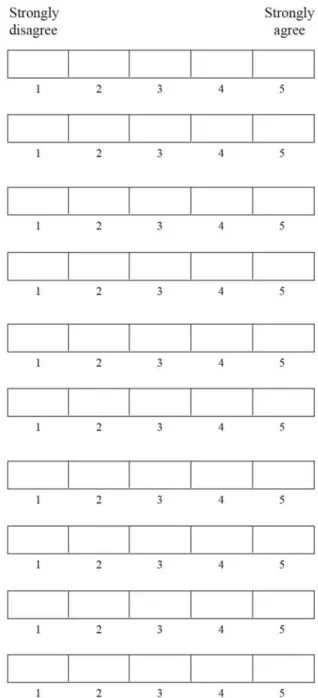
Usability has been increasingly studied by researchers to optimize usage of mobile technologies or information technologies (43). Although usability studies follow different theoretical frameworks, the most common, free, and easy to use framework is the System Usability Scale (SUS) developed by J. Brooke in 1996 (44). SUS, a Likert scale largely used in usability studies, measures user experience, the utility including the efficacy and satisfaction with which users accomplish specific tasks (45). It was created using statements insisting extreme agreement or disagreement to specific statements. A pool of 50 questions were initially used to create SUS. These questions were presented to respondents and statements soliciting extreme agreement or extreme disagreement were used in the final SUS questionnaire (46). According to Brooke et al. ambiguous questions are not good to determine a participant’s attitude towards a specific technology. Therefore, SUS is often the scale preferred by authors of usability studies (46). They assess participants’ immediate reaction to the use of a specific technology, prior to any discussion with the researcher (46). Such studies are often used to understand preliminary needs of users to improve prototype mobile technologies, or to evaluate the usability of an existing technology. A SUS usually comprises
Figure 2: Original 10 statement SUS questionnaire developed by J. Brooke in 1996
PART 2:
There are numerous theoretical frameworks which exist to examine mHealth strategies and/or interventions and their acceptability amongst users, namely the Theory of Planned Behaviour (TPB) (47), the Diffusion of Innovation Theory (DOI) (48), the Unified Theory of Acceptance and Use of Technology (UTAUT) (49). Each respective framework aims to evaluate a different aspect of user acceptability, also classified as intention to use. The TPB aims to demonstrate the attitudes and personality traits existent and influential to human behaviour. The TPB originates from the Theory of Reasoned Action (TRA), but includes the notion of behavioural control for behaviours over which humans have incomplete volitional control (47). A separate theory, the DOI, aims to take a different approach to understanding
the acceptance of a technology. The theory diverges from the norm of persuading individuals to change to a more evolutionary technique involving “reinvention” of product and behaviours to better fit the needs of the individuals (50). The diffusion of new innovations, as defined by Rogers, involves “an innovation that is communicated through certain channels over time among the members of a social system” (48). This theory emphasizes the impact time can have on the rate of acceptance of a specific innovation. It further examines a five stage innovation decision process involving knowledge, persuasion, decision, implementation, and confirmation. Adopters of the technology are also further classified into 4 categories, early adopters representing 13.5% of the study population, early majority (34%), late majority (34%) and laggards (16%) (50). Each of the categories mentioned previously differ from one another due to personality variables, as explained in the DOI. Finally, the UTAUT has four key constructs; performance expectancy, effort expectancy, social influence and facilitating conditions. This theory is largely limited to organizational contexts and bases acceptance to use a technology on the latter. Based on predictions suggested by this theory, performance expectancy, effort expectancy and social influence should encourage behavioural intention and facilitate conditions for acceptance of a technology (49).
Although all models mentioned above present numerous different factors influencing intention to use, there are nuances which render them unsuitable for our research study. Firstly, the TPB is not specific to information systems, or information technologies. Secondly, the DOI is focused on preliminary steps of the development of an innovation, in our case a mHealth intervention, which is not the main focus of our study. Finally, although the UTAUT aims to evaluate individual factors in an organizational context, it is largely focused on technical factors. The proposed theoretical framework for our study is the widely used Technology Acceptance Model (TAM).
Figure 3: Original Technology Assessment Model (TAM) by Davis 1989
The Technology Assessment Model (TAM) proposed by Davis in 1989 is considered to be influenced by the Theory of Reasoned Action (51). This framework is used to evaluate the acceptability of an information technology by users in an organizational setting. The TAM suggests that the acceptance (behavioral intention to use) of a new information technology is affected directly and indirectly by a user’s attitude towards use (A), and two internal individual beliefs; perceived usefulness (U) and perceived ease of use (E). Perceived usefulness is defined to be “the user’s subjective probability that using a specific application system will increase his or her job performance within an organizational context” (51), whereas perceived ease of use is defined as “the degree to which the prospective user expects the target system to be free of effort” (51). Behavioural intention to use measures the likelihood of a person employing the intervention, whereas attitude is related to the user’s evaluation of the desirability of employing the intervention (52). One of the advantages of the TAM is that it can be generalized amongst all populations, however one of its disadvantages is that it does not consider environmental factors such as institutional, or social factors which can influence technology acceptance. Based on the original TAM presented in Figure 3, perceived usefulness has a direct influence on behavioural intention to use, whereas perceived ease of use has an indirect influence, through attitude. Our study plans to use a modified version of TAM, eliminating the Attitude variable (Figure 4). Based on a previous study conducted by Asua et al., attitude and perceived usefulness have shown
multicollinearity, and as attitude is more generic than perceived usefulness, it was eliminated from the TAM model. For this reason, our study has also eliminated attitude from our modified TAM (53).
Figure 4: Adapted version of TAM including user experience
User experience Perceived Usefulness (PU) Perceived Ease of Use (PEU) Behavioural intention to use Part 1 Part 2
CHAPTER 4 Literature review
This chapter provides an extensive overview of existing literature in mHealth strategies worldwide as well as ones targeting TB. A review of literature was performed using a broad search strategy on three main databases; PUBMED, EMBASE and Web of Science. Additional articles were also found through the bibliographies of included articles. The search strategy is presented in Appendix B. This chapter has been divided into five sections to facilitate understanding. We have regrouped the existing studies into the first four sections; user experience, development of mHealth strategies, acceptability of mHealth interventions, and factors influencing adoption of mHealth interventions. The final section presents the knowledge gap in the existing literature as well as the scientific and social justification of this thesis topic.
4.1 User experience: the importance of usability studies
User experience studies are important influencers in mHealth intervention development, as they can potentially help increase eventual uptake and acceptability of the intervention (46, 54). Despite their high importance, few scientific studies have reported evaluation of user experience. Previous studies have indicated the usefulness of SUS to quantify user experience (54, 55). Both studies used mixed-methods by incorporating an interview following the SUS questionnaire to enable qualitative results regarding the mHealth interventions. The study conducted by Uddin et al. in Canada aimed to develop a mobile application to capture the user’s electrocardiogram and transmit it to a mobile phone, in real time (54). The authors assessed usability and task completion through both questionnaires and debriefing interviews. The authors identified the main barrier as insufficient knowledge of the application. Users took more time to complete given tasks, as they were unfamiliar with the application (54). The study conducted by Gunter et al. in the United States of America (USA) assessed the usability of the WoundCheck application, which allows patients to take a picture of their wound and send it to their health care provider from their home (55). Participants are given the application alongside a training program post – operation to assure proper understanding of the application. The authors noticed a high degree of usability of the application, as the average usability (SUS) score was 83.3, however similarly to Uddin et al. the authors noticed delays in task completion as users were not familiar with the application (55). Based on previous studies, the need for user experience is evident. A study conducted by Mourouzis et al. stated the importance of usability studies namely to assure that the
application of choice responds to a specific problem (56). The authors also suggest developing a beta version (prototype version) of the application, performing the usability study on a set of participants and then improving the application prior to dissemination to the public. Although some studies, presented below, have adopted this strategy, the two studies Uddin et al. and Gunter et al. evaluated the user experience of the final versions of their respective applications.
4.2 Development of mHealth strategies
In the context of evaluating the acceptability of mHealth strategies, certain studies aimed to understand the context to further improve their mHealth intervention prior to evaluating the acceptability of the application. A study conducted by Narasimhan et al. in India further demonstrates this notion through their iterative pilot project study design. The authors aimed to use their study to facilitate the eventual acceptance of their mHealth intervention by improving the design of the software and service over time. The authors adopted an eight-step approach to assure proper usability of their mHealth intervention. As there are numerous theoretical frameworks which can be adopted to evaluate acceptance of technologies, the authors adopted a House of Quality matrix as their framework to evaluate the “arrival to users needs” (57). Regarding the health problem studied, the authors aimed to assist in treatment adherence of TB medication amongst TB patients. Treatment adherence remains to be a large issue in LMICs such as India, as patients often refrain from taking their medication after the first two months of the six-month regime (58). Despite the positive results disseminated by the authors, a limitation of the study was noted to be an absence of ownership of mobile phones and knowledge of use amongst illiterate and elderly populations living in remote rural areas (57).
their mPneumonia application. The researchers transformed a paper-based algorithm into a step-by-step electronic questionnaire with instructions, and visual aids (i.e., pictures, videos) on an Android mobile phone based system or a tablet technology. Although this study aimed to understand the usability of the mobile based application, it did not report sufficient findings regarding the acceptability of the application, therefore rendering it unable to reduce the knowledge gap (59).
4.3 Acceptability of mHealth interventions
As mentioned in Chapter 2, section 2.5, there are numerous types of mHealth interventions such as telecommunications (SMS), and eHealth, which aim to support health care professionals or patients in various aspects such as treatment adherence, protocol compliance and education. Based on a systematic review conducted by Kallander et al. summarizing mHealth interventions focussing on community health workers in LMICs, the most common mHealth intervention used was telecommunication (SMS) (60).
Three studies conducted in India aimed to understand the acceptability of a mHealth applications amongst rural health care workers (61), community health workers (62), and the general population respectively (41). Two studies aimed to enforce protocol compliance using a mHealth intervention, through different methods (61, 62). The study conducted by Gautham et al. focused on three conditions: fever, diarrhoea and respiratory problems (61), whereas the second study conducted by Modi et al. focused on promotional maternal, newborn and child health services amongst pregnant women or new mothers (62). Additionally, both studies did not refer directly to the framework used to develop or evaluate the acceptance of the mHealth intervention. However, Modi et al. mentioned the use of a framework recommended by the Medical Research Council (United Kingdom) (62). The study conducted by DeSouza et al. aimed to understand the acceptability of health care interventions via mobile phones, specifically SMS (41). The authors performed a household study, and 99% of participants expressed interest in receiving health promotion on their mobile phones. However, a significant proportion of the participants preferred to receive information through voice calls rather than SMS (41). The authors concluded that a major
barrier was literacy levels in rural villages. SMS reminders are often in English, and patients in rural settings prefer communicating in their local languages (41). Similarly, the main limitation stated by Gautham et al. as well as Modi et al. was the lack of previous exposure to a mobile phone by the health care providers.
Contrary to the three studies mentioned above, a study conducted in Colombia aimed to investigate the potential benefits in performance of community health care workers regarding point of care clinical guidelines implemented as an interactive job aid on a mobile phone based application (63). For the purpose of this study, an interactive job aid was defined as a mobile-based application with audio-visual effects. Although the researchers provided human simulated patients to the community health workers, they found that interactive job aids on a mobile phone help reduce error rates and increase protocol compliance amongst community health workers. The researchers highlighted the main limitation of the study to be the use of human simulated patients rather than real patients as results may vary in real patients due to disparities in medical conditions (63).
Further emphasizing this point, a systematic review conducted by Iribarren et al. aimed to determine the number of TB apps, evaluate their functionality and determine if there was any testing available on the apps (12). The authors identified 1332 health applications, of which only 24 were TB related. Most applications targeting clinicians were not tested formally. There were numerous functionality problems with the applications such as incapacity to open, unavailability of files, and lack of up to date information (12). This systematic review elucidates the need for acceptability studies for mobile applications targeting TB. A systematic review conducted by Aranda-Jan et al. identified 44 studies evaluating mHealth interventions in Africa, of which four focused on staff evaluation, monitoring and guidelines’ compliance (64). The largest number of studies (n=19) assessed patient follow up and
general population (66). This emphasizes the need for studies evaluating health workers’/health professionals’ guideline compliance and health education in LMICs such as India.
4.4 Factors influencing adoption of mHealth interventions
A systematic review conducted by Gagnon et al. aimed to identify studies evaluating factors influencing the adoption of mHealth strategies amongst health care professionals (39). The review was performed on all published studies between the years 2001 and 2014. The researchers included 33 studies regarding mHealth strategies and factors influencing adoption amongst health care professionals. They identified health care professionals as nurses, physicians, residents, health workers, pharmacist and other providers (39). Overall results of the systematic review indicated more than half the studies were performed in developed countries, such as Canada, the United States of America and the United Kingdom. A few studies were performed in Asia and Africa, of which only one study was performed in India (39). All studies were largely conducted amongst health care professionals such as nurses, midwives and community health care workers. This demonstrates the lack of knowledge and studies present worldwide regarding the perspective of health care clinicians and mHealth interventions.
Upon further review of the literature, four studies were retrieved evaluating factors influencing mHealth adoption using an adapted version of the Technology Assessment Model (TAM) (67-70). This theoretical model, further elaborated in chapter 5, is most commonly used in mHealth acceptability studies. A study conducted in Germany adopted Unified Theory of Acceptance and Use of Technology (UTAUT), an advanced extension to the TAM model, as their favored theoretical framework for acceptability analysis (71). All studies evaluated different groups such as; university faculty members (68), university students (70), nursing home residents (69), and inpatient diagnostic groups (71). Although all studies used the original TAM theoretical framework to assess the acceptability of the mHealth interventions, some additional factors were added such as: job relevance, lack of learning management system availability, lack of usage experience (68), and technology
anxiety and perceived enjoyment (69). The study conducted by Alharbi et al. (Saudi Arabia) aimed specifically to evaluate the organizational context (68) and the study by Park (Korea) aimed to evaluate solely the individual context (70). Contrary to the aforementioned studies, Huang et al. (Taiwan) and Henneman et al. (Germany) aimed to test their technologies on patients, namely inpatient diagnostic groups (71) and nursing home residents (69) rather than health care professionals. Overal,l all three TAM studies concluded similar findings to those suggested by the TAM theoretical framework, where an increase in perceived usefulness increases the degree of positivity to usage, which therefore increases the behavioural intention to use (67, 68, 70).
4.5 Knowledge gap & justification
Despite the limited scientific evidence studies have demonstrated a positive uptake of mHealth technologies, namely telecommunications, applications for protocol compliance, and applications for self-evaluation, amongst their respective populations (55, 57-59, 61-63, 71). Further emphasizing this point, Florez-Arango et al. (Colombia) reported a decrease in error rates and enhanced protocol compliance amongst health care workers due to the mobile application (63). However, two main questions soliciting increased research are: the acceptance of such a mHealth technology amongst health care clinicians in India, and the implementation of an mHealth technology to increase TB knowledge.
Firstly, there is lack of knowledge in the acceptance of mHealth interventions or strategies amongst health care clinicians in India. Most studies included in the analysis focused their mHealth strategies towards health care providers/workers (59, 61-63, 67, 68) or towards patients (57, 58, 69, 71). The systematic review conducted by Gagnon et al., identified no studies evaluating an mHealth intervention amongst physicians or clinicians in a LMIC (39).
health care clinicians towards the acceptance of a mHealth intervention for TB in LMICs is evident. As indicated by Akter et al. mHealth is largely consumer driven and consumer centered (40), therefore the need for studies in this specific population (health care clinicians) in an LMIC, such as India, is highly visible. Additionally, Mouzoukis et al. have emphasized the need for usability studies assuring the mHealth intervention responds to a specific problem (56). The study has elucidated numerous steps which may lead to positive uptake of a mHealth intervention, namely: study the user, involve clinicians and health professionals, study health care landscape, and focus on core use cases (56).
Secondly, there are limited studies evaluating mHealth strategies increasing TB knowledge amongst health care clinicians. Of the studies included in this literature review, four studies observed mHealth platforms on diseases or services which were un-related to tuberculosis: maternal and child health services (62), pneumonia (59), geriatric self assessment (69) and fever, diarrhoea and respiratory problems (61). Although the Nihamsan et al. (India) study evaluated treatment adherence to TB, our mobile application aims to educate Indian private sector clinicians on TB diagnosis and treatment practices as this has been noted to be a significant problem in India requiring public health attention (13).
Thirdly, most studies did not include their reference theoretical framework. Most studies stating their reference theoretical framework used the TAM (67, 68) or a derivation, the UTAUT (71). However, these studies were conducted in developed countries (67, 68, 71) or amongst populations other than health care clinicians (68, 71). Additionally, few published studies have evaluated the user experience regarding mHealth technologies. The two studies included in this literature review evaluated user experience after having created the final version of their respective applications. As indicated in previous studies, user experience or usability studies are most fruitful when done on a beta/prototype-version of the application, prior to dissemination (46, 56). Our study aims to assess the user experience, prior to evaluating the acceptability of the mHealth intervention. As mentioned previously, mHealth strategies are often consumer driven, thus to maximize the uptake of our smartphone application, our study aims to further understand consumer needs.
Our study aims to surpass limitations presented in the previous studies, namely limited accessibility (59) and knowledge of mobile technology by study populations (54, 55, 61, 62, 69). A survey conducted in 2013 by the Heart Care Foundation of India on numerous working class professionals, reported that 31% of family physicians used smartphones, and 70% of them keep their cellphone on them constantly (72). This survey validates the knowledge of mobile phone technologies amongst health care clinicians in India.
In summary, the knowledge gap regarding mHealth strategies in India is apparent emphasizing the need for more research in this field. Due to India’s growing mobile phone user-base and TB burden, perhaps mHealth technologies may be a part of the solution to help reduce TB incidence. To our knowledge, a scientific study evaluating user experience and the factors influencing acceptance of a mHealth strategy for TB amongst health care clinicians in India has not yet been documented, therefore bringing upon the interest of our study in the public health platform.
CHAPTER 5 Research Question and Objectives
5.1 Question
Based on the context presented in the previous chapters, our study aims to answer the following two questions:
1. What is the user experience of the private academic clinicians in India while using a smartphone application for tuberculosis?
2. What factors influence the acceptability of a smartphone application for tuberculosis amongst private sector academic clinicians in India?
5.2 Objectives
The main objective of the study is evaluating the user experience and acceptability of a smartphone application – LearnTB – amongst private sector academic clinicians in India. This will be further evaluated through the following sub objectives:
1. Identify the user experience with the aim of improving the mobile application 2. Identify, with the help of TAM, the factors influencing adoption of the smartphone
application.
5.3 Hypothesis
Based on the theoretical background, and context presented above, our study aims to evaluate the following hypothesis, to support our research questions:
1. The usability of the mobile application can influence the user experience of the private sector academic clinicians.
2. The TAM constructs shall explain a significant proportion of clinicians’ intention to use the mobile application.
a. Perceived usefulness is positively correlated to intention to use b. Perceived ease of use is positively correlated to intention to use c. Perceived ease of use is positively correlated to perceived usefulness
CHAPTER 6 Mobile application
This chapter gives an indepth explanation of the smartphone application used in this study,
LearnTB. It permits the readers to visualize the application and understand its origin.
The smartphone application of interest for this study, LearnTB, was inspired by the contents of Let’s Talk TB, a free, online handbook aimed for general practitioners in India (available http://www.letstalktb.org). The handbook has been specifically created for the Indian medical context, and many chapters have been co-authored by Indian doctors. The LearnTB application, a collaboration between Mayo Clinic Center for Tuberculosis (Rochester, USA) and McGill International Tuberculosis Centre (Montreal, Canada), aims to educate Indian clinicians regarding the definition, diagnosis, treatment, management and counselling practices available for TB. The primary version of the application was created by Global Innovative Services Inc. (Maryland, USA) This study tested the pilot website (prototype) version of the application.
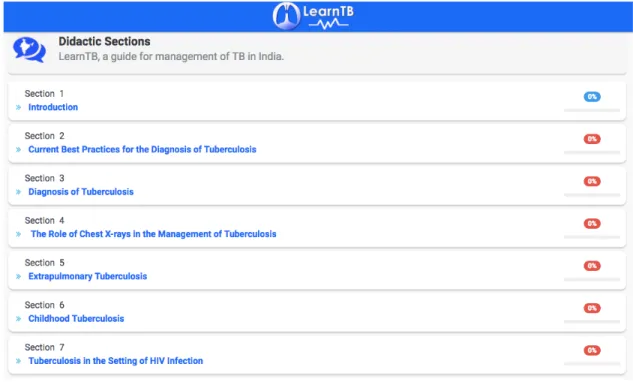
LearnTB presents numerous different sections regarding TB management, such as childhood
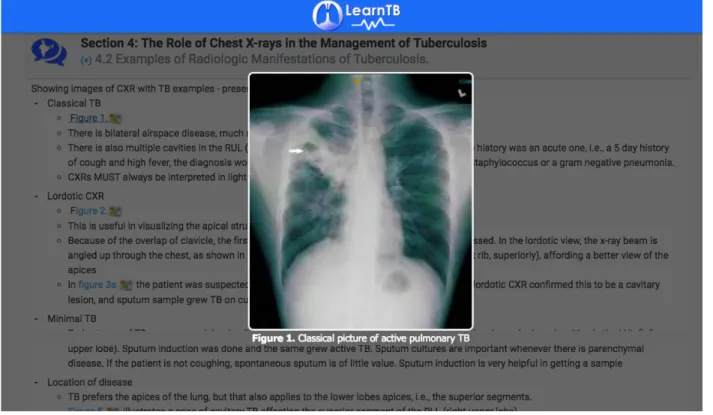
TB, latent TB infection, extra pulmonary TB, and common pitfalls of TB management (Figure 5). Each section is based on International Standards of TB Care, as well as WHO guidelines and Standards for TB Care in India (73, 74). When clicking on a specific section (ie. Childhood tuberculosis), participants are presented with subsections involving suspecting, diagnosing and treating TB for each respective case (Figure 6). Dosage tables, and specific names of drugs are also included to facilitate understanding and ensure comprehension. A subsection regarding chest x-rays for TB presents figures of different types of TB lesions to help visualize the extend and manifestations of TB disease (Figure 7). The section focusing on the TB HIV co-infection also includes frequently asked questions to help clinicians asses specific/special cases. In addition to reference material, most sections present
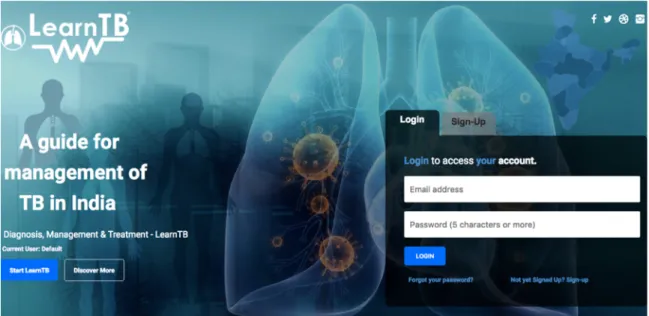
Figure 5: LearnTB application – home page
Figure 7: LearnTB application – figure of chest x-ray in Section 4 “Role of chest x-rays in the
CHAPTER 7 Methodology
This chapter illustrates all methods used for this research study. To facilitate comprehension, it has been separated into 6 detailed sections: study design, study setting, study population, data collection (part 1 and part 2), data analysis (part 1 and part 2), as well as ethics considerations and approvals. Hereinafter, the first part of the study will be named “usability (part 1)” and the second part, “acceptability (part 2)”.
7.1 Study design
As the main purpose of the study was to describe the user experience and acceptability of the
LearnTB smartphone application amongst private sector clinicians in India, a cross-sectional
study design with no comparator group was used. Cross sectional studies are used to describe a subpopulation within a reference population based on a specific outcome, at a given point of time (75). They do not evaluate associations over a period, thus causality cannot be inferred. Previous studies have used a cross sectional design for their user experience and/or acceptability evaluations as well, thus this study design was preferred for our study as well (53, 67, 68, 70).
7.2 Study setting
Both parts of the study took place at Kasturba Hospital Manipal, Manipal, India located in the south Indian state of Karnataka. Karnataka, located on the west coast of India, is one of the four large south Indian states with a population of 61.1 million (76). It has an overall TB case notification rate of 98 per 100 000 (77) and approximately 40 000 TB patients are treated in private clinics annually (78). It experiences one of the highest TB HIV coinfection epidemics in India. Karnataka is separated into 30 districts, one of which is the Udipi district which hosts Kasturba Hospital Manipal (Figure 8). The town of Manipal has a population of 280 000 which is largely comprised of Manipal University students, faculty and staff (79). Kasturba Hospital Manipal, a tertiary teaching hospital for Kasturba Medical College, Manipal University, has 2023 beds, 300 consultant doctors, 200 duty doctors, and 2200 support staff (80). It is ranked as the second best private medical college in India and is the first medical hospital in Karnataka to achieve a National Board Accreditation of Hospitals
(80). Overall, Kasturba Hospital Manipal comprises of 104 professors, 103 associate professors, 102 assistant professors, 66 senior residents, 685 post graduate students, 183 interns, and 1561 MBBS (medical undergraduate degree) students (81).
Figure 8: Map of Manipal, Karnataka, India (source : http://szusicon2017.com/travel/)
7.3 Study population & recruitment
Academic clinicians practicing at Kasturba Hospital Manipal were the target population for our study. All clinicians having completed their MBBS and working at Kasturba Hospital Manipal were eligible to participate in the study. The numbers presented in the section above (section 7.2) illustrate the large clinician population present at Kasturba Hospital Manipal. In India, one third of clinicians practice in the private sector and studies have shown that
research studies for TB (82). The latter, in addition to mismanagement of TB in the private sector, justifies the choice of the target population.
For the usability study (part 1), five participants were recruited in February 2017 through non probabilitistic convenience sampling. A sample size of 5 was chosen as previous studies have indicated that most errors (mean 85.5%) in technologies are identified by five participants (83, 84). Usability studies aiming to assess user experience problems in prototype technologies, such as LearnTB do not require large sample sizes (84).
For the acceptability study (part 2), 100 participants were recruited via non probabilistic convenience sampling as well as snow ball sampling between February 2017 and March 2017. A minimum sample size of 100 was sufficient as the sample size calculation was based on a theoretical outcome of a standard deviation of 1.07, evaluated by previous studies (67, 70). Type I error (a) of 5% and a margin of error of 3% were used. Participants were contacted informally through their unit heads, and asked to meet with the lead researcher TP to participate in the study. Non-probabilistic convenience sampling is often preferred when there are the following three criteria: (a) the target population is difficult to identify, (b) the target population is specific and have limited time, (c) the study is a pilot study (85). Our study responds to two out of the three previously mentioned criteria, thus non-probabilistic sampling was preferred. Furthermore, snow ball sampling was used for the second part of the study to increase the sample size. It is defined as a sampling strategy that researchers adopt when the target population is difficult to reach (85). Study participants were asked to relay the information about the research project to their peers to increase visibility of the research project. Based on observations made while in the field, academic clinicians are often a difficult target population as they are highly burdened with work in private hospital settings. For this reason, snow ball sampling was also used to help attain the desired sample size of 100 participants. TP was paired with an intern doctor at Kasturba Hospital Manipal who helped recruit participants for the study. Participants were contacted by their superiors through word of mouth and also through the use of mobile chatting applications such as
WhatsApp. These methods helped increase visibility of the project, enable snowball sampling and reach the desired sample size.
7.4 Data collection
Prior to each individual part of the study, all participants were given detailed consent forms indicating the goals and objectives of this study. Participants were asked to read and sign each consent form. All participants were assured of confidentiality and anonymity of responses. Theoretically, part 1 and part 2 of the study are supposed to be conducted consequtively to ensure that comments provided by the participants during the usability study can be incorporated and tested in the acceptability study. However, due to time constraints, our study conducted both parts simultaneously.
Part 1: Usability
The usability testing was done through a 9-statement, paper-based English questionnaire using SUS (Appendix C). The original SUS comprises of 10 statements, however one statement “the application was easy to use” was omitted as it would be repeated in the second part (acceptability) of the study. The content validity of the questionnaire was justified, as the statements were from the original version of a SUS questionnaire which has a high Cronbach alpha (a = 0.91) (86). A total of 5 participants were contacted to participate in this part of the study and all 5 (100%) responded to the questionnaires. Participants were given the application in its website format, on an iPad and asked to complete two tasks (Appendix D). The tasks forced the participants to use the LearnTB application, and understand the different functions within the application. Participants were given approximately 5 minutes to complete the tasks. Once completed, they were asked to rate 9 statements on a 5-point SUS scale ranging from “strongly disagree” (1) to “strongly agree” (5). Sociodemographic