Spasticity in disorders of consciousness: a behavioral study
Texte intégral
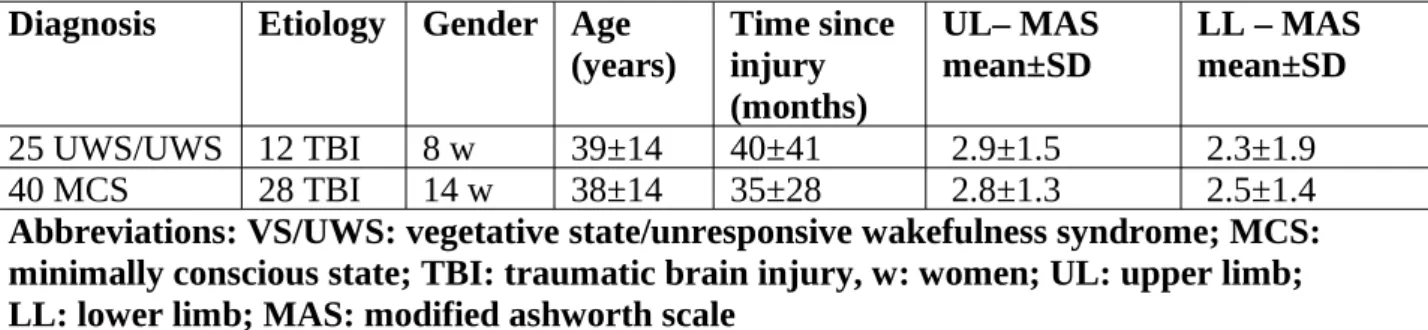
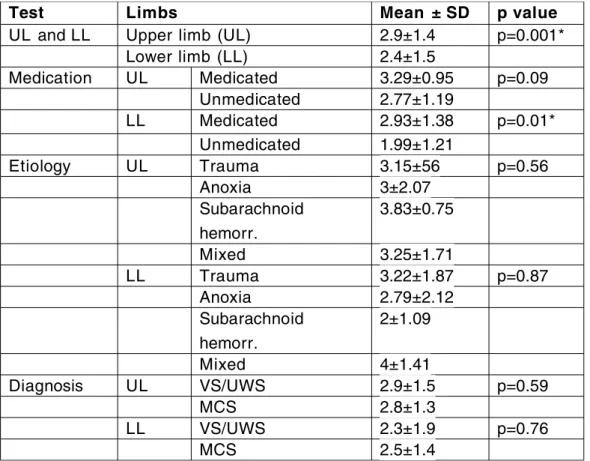
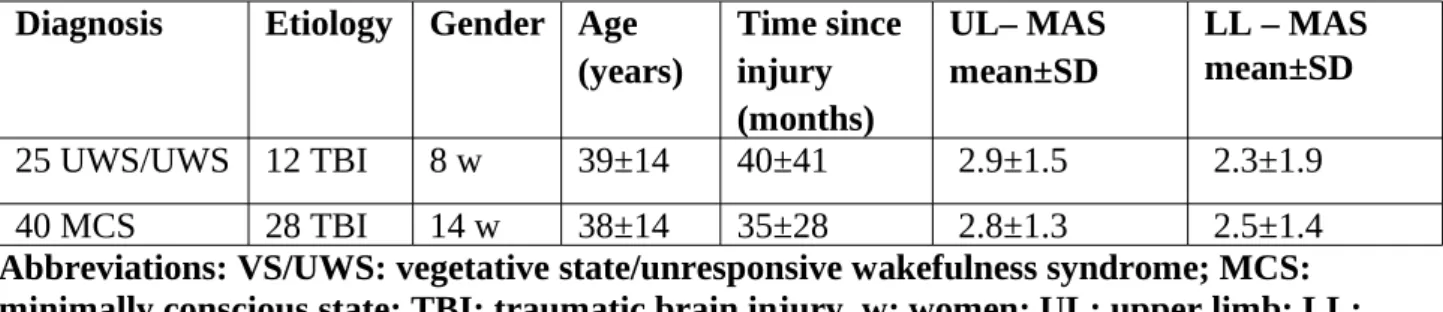
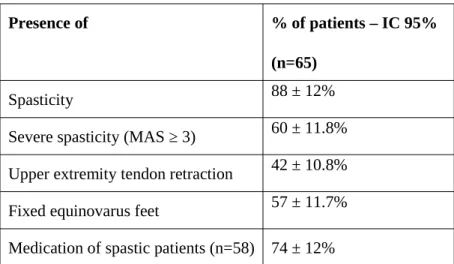
Figure
Documents relatifs
We tested for two additional contrasts an- alyzed by Smolka et al.: the difference in priming strength between Transparent and Opaque Deriva- tion (not significant in either
Scanned characters (blanks ignored) are com- pared with names of all 0BJECT types in program. Digits following a left parenthe- sis, or the rightmost d characters, are assumed
The End-of-File control word causes input processing to revert to the file that invoked, the current imbed file.. If the current file was not imbedded,
PSEUDONYMS: Pseudonyms can be used in Confer II conferences for items, responses, and messages, and participants can register in the conference under a
The server will generally send a list of valid flags, number of messages, and number of messages arrived since last access for this mailbox as unsolicited data, followed by an
The 12 full members shall be approved by vote of the Board of Trustees of the Internet Society (ISOC), while the IETF chair shall be approved by vote of the 12
Analyses of workforce data about the number of pediatric specialists in the USA and Australia show that data sets representing physicians often represent
As leader of the Fishermen's Protective Union whose political career followed a parallel course of decline with that of the c ountry as a whole, particularly
