GRANT HANDRIGAN
OBESITY AND BALANCE CONTROL
Thèse présentée
à la Faculté des études supérieures et postdoctorales de l‘Université Laval dans le cadre du programme de doctorat en Kinésiologie
pour l‘obtention du grade de Philosophiae Doctor (Ph.D.)
DÉPARTMENT DE KINÉSIOLOGIE FACULTÉ DE MÉDECINE UNIVERSITÉ LAVAL QUÉBEC 2013 © Grant Handrigan, 2013
Résumé
L'obésité affecte le contrôle de l'équilibre. Deux facteurs, biomécanique et sensoriel, contribuent à le réduire. Une masse augmentée, située au niveau de l'abdomen, provoque une augmentation du moment de force gravitationnel à la cheville. Une plus grande force musculaire est alors nécessaire, introduisant plus de variabilité dans le contrôle moteur, ce qui mène à des oscillations du corps plus importante. La deuxième composante qui n‘a pas encore été vérifiée, suggère qu‘elle soit la résultante des effets de l'augmentation de la masse corporelle sur les mécanorécepteurs plantaires. Ces mécanorécepteurs fournissent de l‘information liée à la position du centre de pression. La surcharge pondérale pourrait augmenter le seuil de sensibilité des mécanorécepteurs et ainsi réduire la qualité des
rétroactions sensorielles. Cela causerait des oscillations du corps de plus grande amplitude. Cette thèse explore ces hypothèses.
Afin d'évaluer si la force musculaire permet un meilleur contrôle de l‘équilibre, deux projets distincts ont été effectués. Le premier projet évaluait la manière dont la force musculaire et le contrôle de l‘équilibre étaient affectés par la perte de poids. Le deuxième projet consistait à mesurer le contrôle de l'équilibre dans un groupe d'individus athlétiques bien entrainés avec un indice de masse corporel (IMC) semblable aux personnes obèses. Les deux projets ont démontré que le contrôle de l‘équilibre n'était pas affecté par la force de contraction maximale des quadriceps dans la population obèse. Dans un troisième projet, nous avons évalué et constaté que l'obésité contribuait à réduire l'équilibre chez les
personnes âgées.
Deux autres projets ont été réalisés afin d‘étudier la contribution des afférences provenant de la voûte plantaire sur le contrôle de l'équilibre. Le premier impliquait un refroidissement de la voûte plantaire et mesurait son effet sur le contrôle de l'équilibre. À court terme, un effet sur la réduction du contrôle de l‘équilibre a été observé. Le projet final de cette thèse portait sur l‘effet à court terme d‘une masse ajoutée au corps, pour simuler l‘impact de l‘obésité, sur la sensibilité plantaire. Dans des conditions où la voûte plantaire subissait une pression accrue, nous avons trouvé une sensibilité plantaire réduite. Ces résultats supportent l‘hypothèse sensorielle, sans toutefois écarter l‘hypothèse mécanique, pour expliquer l‘association entre une réduction du contrôle de l‘équilibre et l'obésité.
Abstract
Obesity affects balance control. There are two possible contributing factors to this reduced balance control: biomechanical and sensory. The increased mass, that is centrally located on the abdomen, causes an increased gravitational torque about the ankle joint. This increased ankle torque requires greater muscular strength and this introduces greater variability into the control system and results in larger body oscillations. The second component that has not yet been identified is suggested to result from the effects that an increased in body mass has on the plantar sole mechanoreceptors. These mechanoreceptors participate in body sway awareness and it is thought that the additional mass of the body may alter the sensitivity of these mechanoreceptors and reduce the quality of the feedback afferent signal and this may then lead to larger body sway. This thesis explores both of these hypotheses.
In order to observe how muscular strength affects the mechanical contributions towards quiet standing we performed two separate projects. The first project evaluated how weight loss affected muscular strength and standing balance control. The second project involved measuring balance control in a group of athletic individuals who were well trained but had a body mass index (BMI) similar to obese individuals. Together, both projects demonstrated that balance control is not significantly associated by quadriceps maximal voluntary contraction strength in the obese population during normal quiet standing. In a third project, we evaluated whether obesity affects balance control in elderly females. To single out the role of obesity, balance control of normal weight elderly women was compared to that of obese elderly women. We found that obesity contributes to reduced balance control in elderly individuals. This has important implications as a falls risk factor in this population.
We also performed two projects investigating the sensory contributions to reduced balance control. The first project involved cooling the plantar sole and measuring balance control. A short term effect of reduced balance control was found. This demonstrates that reducing the sensation of the plantar sole affects standing balance control. The final project in this thesis measured the effects of two things on plantar sole sensitivity; the effects of adding a short term mass to the body and the position of the center of pressure relative to a point of stimulation. In conditions with increased pressure on the plantar sole we found
reduced sensitivity in the plantar sole. This has implications for explaining the reduced balance control in obesity. In conclusion, this thesis explores biomechanical and sensory contributions to standing balance control.
Acknowledgements
This thesis was a collaborative effort.I would like to say a special thanks to my supervisor Dr. Philippe Corbeil for his support throughout my PhD. I would also like to thank my co-supervisor Dr. Martin Simoneau and Dr. Normand Teasdale for their support. GRAME offered me an environment of unparalled support, independence and encouragement. This has been invaluable for me and I am grateful to have worked with you.
Marcel Kazsap and Michael Lefebvre assisted me with some of the more technical aspects of my PhD and I am grateful for their assistance.
Each project in this thesis required volunteer participants. I would like to thank these individuals who graciously donated their time.
The Newfoundland and Labrador Centre for Applied Health Research recognized the value of our work and supported me for the final year of my PhD. Thank you.
Over the past four years there have been a number of people who have been in the lab and I am grateful for all of their assistance and the good times that we spent together. I would like to specifically mention Martin Lavallière as we shared an office together for four years and never once had a disagreement!
To my parents, Ursula and Garrett, your support had no limits and for this I am grateful. To my brothers, Christian, Gregory, John Paul and Joshua, you have been supportive and each of you, in your own turn, have offered me advice when I needed it and a laugh when I needed one. Thank you.
Colin and Mark, thank you for the good times that we‘ve shared and here‘s to many more! Annie-Pier, tu as été là pour la partie la plus difficile de ma thèse et je suis reconnaissant pour ton soutien. Merci.
“Do not be too timid and squeamish about your actions. All life is an experiment.”
Table of contents
Résumé ... ii
Acknowledgements ... v
Table of contents ... vii
List of tables ... viii
List of figures ... ix
Chapter 1 - General introduction ... 1
Chapter 2 - Review of literature ... 4
1 - Balance control ... 4
2 - Balance control and obesity ... 33
Résumé – Chapitre 3 ... 42
Chapter 3 - Balance control is altered in obese individuals ... 43
Résumé – Chapitre 4 ... 49
Chapter 4 - Weight loss and muscular strength affect static balance control ... 51
Résumé – Chapitre 5 ... 71
Chapter 5 - The effects of muscle strength on center of pressure-based measures of postural sway in obese and heavy athletic individuals ... 72
Résumé – Chapitre 6 ... 85
Chapter 6 - The impact of obesity on balance control in community-dwelling older women ... 87
Résumé – Chapitre 7 ... 105
Chapter 7 - Short term alteration of balance control after a reduction of plantar mechanoreceptor sensation through cooling ... 106
Résumé – Chapitre 8 ... 121
Chapter 8 - Short term changes in plantar sole sensitivity during upright standing when an external load is added ... 122
Chapter 9 - Conclusion ... 141
List of tables
Chapter 4
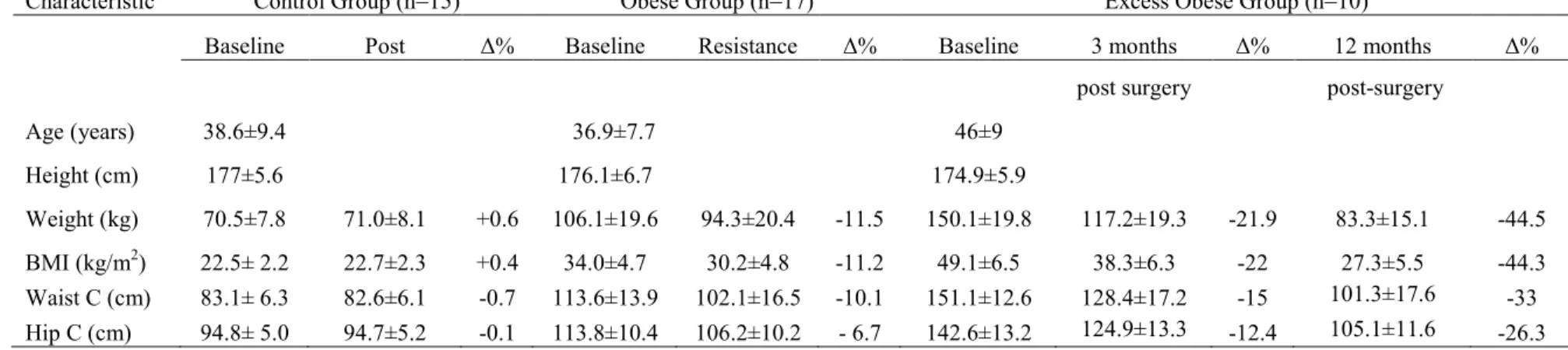
Table 1 – Subject characteristics 64
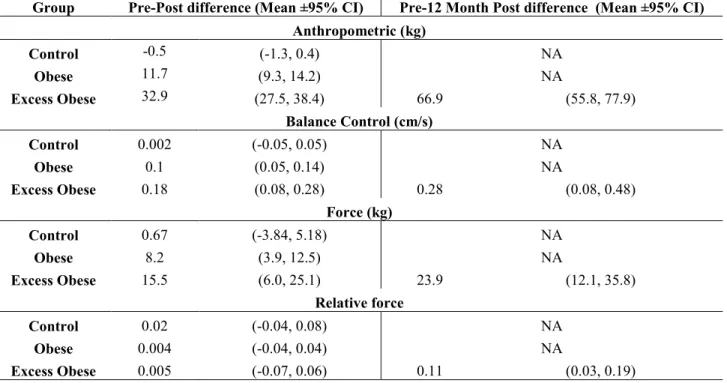
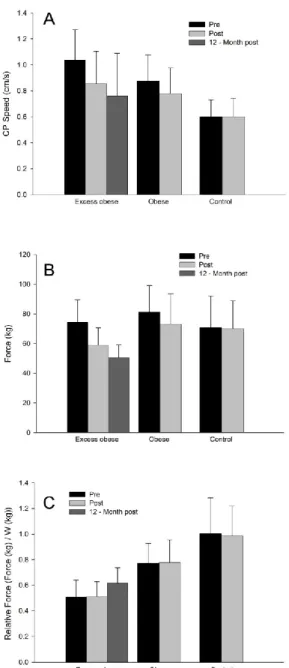
Table 2 – Pre-post dependent variable measures 68
Table 3 – Balance control measures 69
Chapter 5
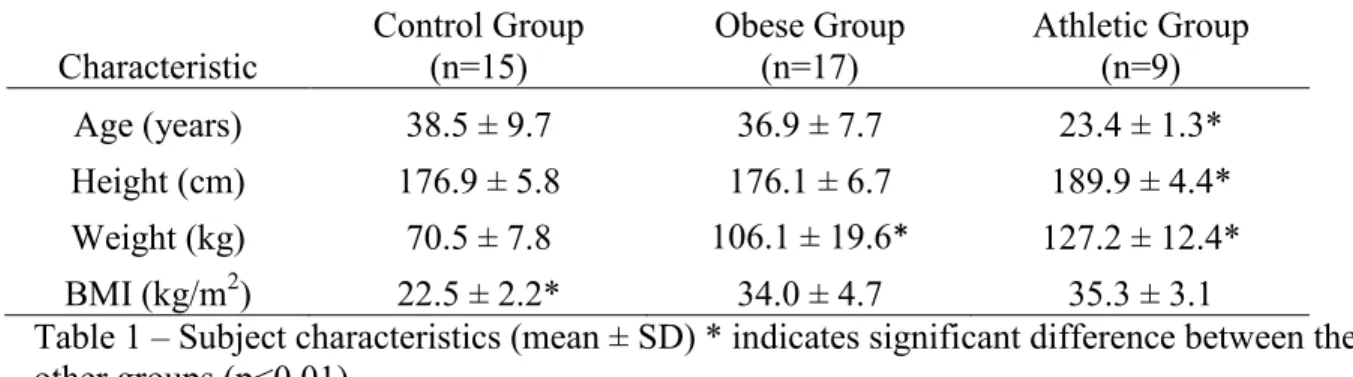
Table 1 – Subject characteristics 84
Table 2 – Absolute strength and relative strength 87
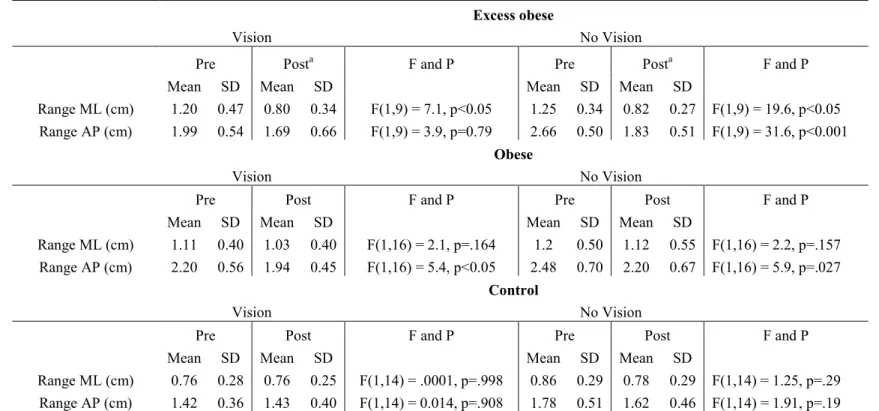
Table 3 – Medio-lateral and anterior- posterior (vision) 88
Chapter 6
Table 1 – Subject characteristics 101
Table 2 – Postural parameters 104
Chapter 7
List of figures
Chapter 2
Figure 1 – Scheme of the human ―inverted pendulum‖ for sway in the sagittal plane 16
Figure 2 – Summary of the different modes of control 22
Figure 3 – Plantar sole mechanorecptor distribution 29
Chapter 3
Figure 1 – Summary of CoP values 54
Chapter 4 Figure 1 –CoP speed 70
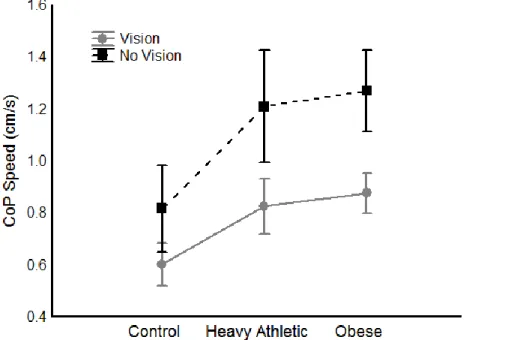
Chapter 5 Figure 1 – Vision and No Vision CoP 87 Chapter 6 Figure 1 –CoP speed 102
Chapter 7 Figure 1 –Experimental timeline 121
Figure 2 –CoP and EMG trial by trial results 124
Chapter 8 Figure 1 –Experimental setup 136
Figure 2 –Representative plantar sole pressure scans 139
Figure 3 –Amplitude force curves for representative subject 139
Chapter 1 - General introduction
The overarching theme of this thesis is human standing balance control, particularly in individuals who are overweight and obese. Why study balance control? There are two main reasons. The first is to understand the underlying sensorimotor control mechanisms that are used for maintaining standing balance. This information is useful for clinicians, practictioners and health. The second reason for studying balance control is to identify falls risk factors. Falling is a common occurrence in elderly persons and it can have a serious negative impact on the mobility and mortality of a person, particularly for an elderly person. Our aim is to explore biomechanical and sensory contributions to balance control. As balance control is a broad area of research in this thesis our specific inquiry was how obesity affected balance control. In order to accomplish this we developed and completed several experimental projects that had specific objectives. These projects are detailed in chapter three to eight.
There are two hypotheses to explain the reduced balance control in overweight and obese individuals. This thesis focuses on exploring specific aspects of these two broad hypotheses. The first is a mechanical contribution and the second is a sensory contribution. The mechanics of balance control are complex. In a simple form, standing balance control can be modeled as an inverted pendulum (Smith, 1957). Obese individuals have an
accumulated mass that is centrally located on the trunk (Menegoni et al., 2009; Power & Schulkin, 2008), which is away from the axis of rotation (ankle joint). This increased mechanical demand requires greater gravitational torque (generated at the ankle joint) to maintain equilibrium. In order to counter these demands increased muscular torque is necessary and is provided by increased amplitude of the motor commands. As a
consequence, it has been suggested that this introduces greater variability into standing balance control (Corbeil, et al., 2001). In addition to the biomechanical constraints, the added mass of obesity has also been suggested as a potential modifier of the sensory information that the plantar sole mechanoreceptors provide for standing balance control (Dutil et al., 2012; Handrigan et al., 2010; Hue et al., 2007; Teasdale et al., 2007).
Specifically, the plantar mechanoreceptors respond to tactile stimulation. It is proposed that the added mass in obese individuals reduces the sensitivity of the mechanoreceptors and therefore reduced the quality of the sensory information. The underlying string of thought
that connects each chapter in this thesis is to explore these hypotheses and to further our understanding of standing balance control. Below I will introduce each chapter and its specific contribution.
In the third chapter of this thesis, I address the debate in the scientific literature as to the effect of obesity on balance control (Blaszczyk, et al., 2009; Handrigan, et al., 2010). This chapter is a published letter to the editor of the Journal of Biomechanics and it is a scientific justification and defense of the work of several research groups on the effect of obesity on balance control. This letter was written in response to a published article that showed obese females had improved balance control compared to lighter weight
individuals – a result that is contrary to what most other researchers have found.
The fourth chapter in this thesis contains a publication that investigated the effect of weight loss on measures of balance control and muscular strength. This chapter is an expansion on previous work (Hue et al., 2007, 2008; Teasdale et al., 2007) and was part of a larger project. The previous work investigated the effects of weight loss on balance control and also at the effects of weight loss on muscular strength. In this publication, we investigated the combined effects of weight loss and reduced muscular strength on balance control.
In the fifth chapter of this thesis I describe a project that continued investigating the role of lower limb muscular strength in standing balance control for obese persons. In this project we selected a group of heavy athletic individuals that were obese (body mass index (BMI) greater than 30) but these individuals had significantly greater absolute and relative muscular strength than a control group of sedentary obese individuals. The objective of this project was to evaluate whether greater lower limb muscular strength improved balance control in obese individuals.
In the sixth chapter of this thesis I describe a project that investigated the effect of obesity on balance control in community dwelling elderly women. Aging is associated with reduced balance control. Our aim was to evaluate if obesity further exacerbates reduced balance control in this population.
In the seventh chapter of this thesis I describe a project that was a shift in focus from the mechanical hypothesis to the sensory contributions of balance control. The specific sensory system that interested us was the plantar sole mechanoreceptors. I
conducted a project that involved cooling the plantar sole by immersing the participants‘ feet in ice water. Our intent was to cool the sole and use this as a means to alter the quality of the sensory information from the plantar sole cutaneous mechanoreceptors and observe how this affected balance control.
In the eight chapter of this thesis I describe a project where I assess the sensitivity of the plantar sole mechanoreceptors. I used a custom force platform to test the plantar sole sensitivity during upright standing. The effect of an added mass on the plantar sole contact pressure and sensitivity as well as different postures (i.e., different center of pressure positions) was measured. Normal weight subjects were measured with and without an added mass. The added mass was used to simulate an obese individual. The aim of this project was to evaluate if there are short term changes in the plantar sole sensivity due to changes in body weight and plantar sole pressure.
Before presenting a detailed description of the results and conclusions of this thesis it is necessary to review the literature and provide an update on our understanding of standing balance control. The second chapter in this thesis is a description of balance control including the different mechanisms involved in the control and regulation of standing balance control.
Chapter 2 - Review of literature
1 - Balance control
1.1 Balance control: definition
Balance control is a fundamental activity of daily living. Upright standing is a position that serves as a basis for many of our movements. Performing this complex coordinated task, and for it to appear so simple, is the combined result of the integration of information from three primary sensory systems, the visual, vestibular and somatosensory systems and also the generation of appropriate neuromuscular responses. The contributing importance of the various sensory systems is situationally dependent. For example, the visual system is important for standing balance control but it becomes even more important during walking and obstacle avoidance. However, when you close your eyes in a neutral standing position your balance control is impaired compared to with your eyes open but you do not fall over. This adaptability, in the weight of the contributions, is essential but it also adds to its complexity. Furthermore, the human body during upright standing is constantly experiencing naturally occurring perturbations in the form of our own movements (e.g. beating heart, breathing). The central nervous system (CNS) manages these perturbations by feed forward and feedback control (Massion, 1994; Massion et al., 2004; Pai, Wening, Runtz, Iqbal, & Pavol, 2003). These actions are also known as postural adjustments (PAs) and are either anticipatory postural adjustments (APAs) or
compensatory postural adjustments (CPAs). Anticipatory adjustments are adjustments that are made prior to performing a voluntary movement (Bouisset & Do, 2008). APAs have a dual role that they are simultaneously a perturbation but also a counter-perturbation. The very act of initiating an adjustment pre-movement can cause a perturbation in the balance control system. At the same time this anticipatory movement was initiated in response to an upcoming voluntary movement (Bouisset & Do, 2008). CPAs are generally classified as either a fixed-support strategy or a change in support strategy (Maki & McIlroy, 1997). These strategies are covered in greater detail further in this review of literature. Both of these types of PAs act to maintain the body‘s centre of mass within its base of support (BoS) or to maintain an upright alignment of the various body segments
maintaining balance control, can also be thought of as a combination of passive and active components. The passive components are intrinsic mechanical properties of
musculoskeletal structures/tissues (e.g. tendon and muscle stiffness) and the active components can be summarized as the processes involved in motor control, for example, neuromuscular (e.g. muscle contractile characteristics, motor unit recruitment and neural coordination).
The active components of balance control can also be represented as muscular strength and power. During standing balance control a minimal amount of muscular strength is necessary to maintain balance control in normal healthy individuals. Some modeling work has been performed to investigate the amount (magnitude) of ankle torque that is produced for standing balance control and small voluntary perturbations (pulling task). The torque that is necessary for maintaining standing balance control in these two situations is modest in terms of the overall strength that a healthy individual is capable of providing, if forced. They are estimated to range between 10 and 80 N•m of ankle torque depending on how close the CoP approaches the safety margins of the foot which are the extremities (toe or heel) (Patton, Pai, & Lee, 1999). In healthy individuals (male mean age 53 years and female mean age 52 years), isokinetic mean peak ankle extension torque is rated as 33 N•m for male and 21.3 N•m for female, and, mean peak ankle flexion torque is 111.8 N•m for males and 76.4 N•m in females (Harbo, Brinks & Andersen, 2012).
Although the demands of standing balance control are low for young healthy individuals. In populations with disabilities, mobility impairments and disease, for example, in an obese or overweight population or elderly frail individuals, relative muscular strength may be more important. These topics are relevant to the thesis and are covered in much greater detail in their respective sections.
A simple definition of balance control is the maintenance of the body‘s CoM within the BoS (Maki & McIlroy, 1997). This definition is sometimes contested in dynamic tasks (such as walking) where the CoM may momentarily be outside the BoS. As well, the velocity of the CoM is also considered to be an important determinant of balance control, that is, a fast moving CoM may still be within the BOS but balance is lost and the CoM eventually falls outside the BOS (Pai & Patton, 1997). A related and highly correlated
variable of the CoM is the Centre of Pressure (CoP). The CoP is defined as the net point of location of the vertical ground reaction force vector (Winter, 1995). This thesis focuses on quiet standing balance control and defines balance control as maintaining the body`s CoP within its BoS. As there is some confusion in the research literature as to what is static and dynamic balance control it is necessary to clarify this situation. Standing balance control is often misleadingly termed ‗static‘ balance control. The regulation of standing balance control is not a static activity in the true sense of the word. Standing balance control is certainly a dynamic process necessitating continuous adjustments. In the research literature, for the most part, dynamic balance control refers to balance control during walking or recovery from an external perturbation and static balance control refers to quiet standing balance (Hrysomallis, 2011). As there are many different definitions of balance control, it seems appropriate to address this question as did Massion et al., (2004) and to explain the definitions of balance control in terms of its functions. Balance control has two main functions; these are antigravity control and the interface between perception and action. The antigravity function provides two main services, to provide structural support for all of the body segments and maintain upright stance, and to provide a support system for the moving segments of the body. The second function of the postural control system is that it provides an interface between the body and the external environment (Massion, 1994; Massion et al., 2004). Another functional definition of balance control is to ensure postural orientation and postural equilibrium (Horak, 2006). Here, postural orientation is defined similarly to the antigravity control of Massion et al., (1994, 2004); its principal role is body alignment with respect to gravity. Postural equilibrium is defined as the convergence of the sensorimotor actions with the goal of stabilizing the body‘s center of mass. While some of the specifics may differ in the two definitions, their basic components are the same. In summary, the two main functions of balance control are to maintain upright stance and body segment orientation with respect to gravity and to do this while interacting with the environment.
1.2 Balance control: regulation
A long standing view of balance control was that as an individual leaned forward stretching of the calf muscles occurred (Fitzpatrick, Burke, & Gandevia, 1996; Fitzpatrick,
Taylor, & McCloskey, 1992; Fitzpatrick, Rogers, & McCloskey, 1994; Gatev, Thomas, Kepple, & Hallett, 1999; Winter, Patla, Prince, Ishac, & Gielo-Perczak, 1998). This muscle stretching provoked the stretch receptors to signal that the body was leaning forward and that a reverse torque was needed to maintain stability. The primary roles of stretch receptors in the balance control musculature (calf muscle spindles and Golgi tendon organs) are detecting the length, speed, and tension in muscle tissue and then
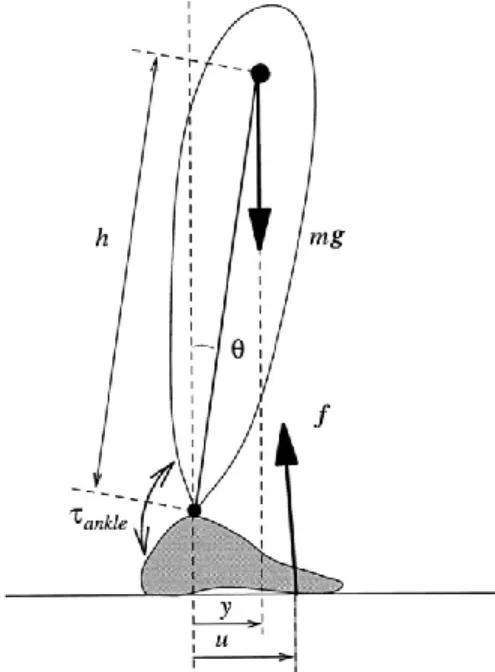
communicating this information to the CNS (Kandel, Schwartz, & Jessell, 2000; Proske, 2005). During balance control this is essential feedback that helps the body adjust its movement and provide appropriate spatial orientation and responses. Golgi tendon organs and muscle spindle receptors are primary contributors of this sensory information. The Golgi tendon organs are typically responsible for detecting muscular force and muscle spindles detect muscle length changes and speed. Balance control requires minimal muscular activity and presumably, for this reason, the Golgi tendon organs contribution to proprioceptive inputs during balance control is minimal. During standing balance control the ankle joint is considered the primary joint of rotation (inverted pendulum model see Figure 1) and the muscle stretch reflex (in the calf muscles) that occurs around this joint is thought to provide the essential information for maintaining balance control (Bloem, Allum, Carpenter, & Honegger, 2000; Loram, Maganaris, & Lakie, 2009; Nashner, 1976).
Figure 1 – scheme of the human ―inverted pendulum‖ for sway in the sagittal plane. From Morasso PG, Schieppati M, J Neurophysiol 1999;82:1622-1626.
For the inverted pendulum model it was once suggested that passive
musculoskeletal processes (inherent stiffness) alone contributed adequately to maintain balance control (Nashner, 1976; Winter et al., 1998). These authors explained that reflexes (after the neuromuscular delays) were responsible for the maintenance of standing balance control, specifically the springlike nature of the muscle actions around the ankles. This model is also known as the ‗stiffness model‘. As there are a variety of values (% of the total gravitational torque ‗mgh‘ ‗m‘ is body mass, ‗g‘ is gravitational acceleration and ‗h‘ its CoM above the ankle joint) suggesting how much the stiffness model contributes to standing balance control, Loram et al. (2007) set out to measure just how much of balance is controlled by stiffness and intrinsic musculoskeletal properties. These authors found that the amount or contributions of stiffness and intrinsic musculoskeletal properties invariably depends on the distance of the CoM away from the vertical line of gravity. For larger CoM displacements or greater body deviation from the vertical it is necessary to increase active components of balance control. For example, a CoM position of 2-3 cm in front of the ankle can be supported entirely by passive ankle torque. However, most individuals maintain their CoM approximately 4-6 cm in front of the ankle joint and this requires approximately 12-18 N•m of active torque (both legs combined) (Loram et al., 2007). Other research supports these results (Morasso & Sanguineti, 2007).
Another model of balance control that has been developed is known as the feedback control of balance. The feedback model of balance control states that the corrective torques for maintaining standing balance (against the gravitational vector) occur in a feedback system and that the sensory systems contribute to maintaining the body‘s position and adapting to changes in the environment
(Kiemel, Oie, & Jeka, 2006; Peterka, 2000; van der Kooij & de Vlugt, 2007). This is different than the stiffness control of balance in that balance control is not thought to be modulated by reflexes and the inherent stiffness of the system. There are various levels of complexity that have been developed in the feedback model of balance control, including models that contain feedback loops with sensory integration and neuromuscular time delays integrated (Mergner, 2007).
Another model of balance control has been developed based on a series of studies that measured in vivo muscular contractions during standing balance control with dynamic
ultrasound imaging (Loram & Lakie, 2002; Loram, Maganaris, & Lakie, 2004, 2005a, 2005b). As the body leaned forward the muscles contracted and as the body leaned
backwards the muscles stretched. They observed muscle contractions that were contrary to what was expected. This research by Loram and colleagues contradicts the assertion that the muscle spindle and Golgi tendon organ feedback from the calf muscles is a primary feedback model for balance control. The paradoxical contractions (negatively correlated muscle contractions with the motion of the body) of the calf infer that balance control is either an active process or that another sensory source is the primary feedback model for balance control (Loram et al., 2009). What then is this sensory source? These authors assert that a muscle that crosses the ankle joint and that has periods of minimal activation (thus periods with reduced background noise interference) would be a prime candidate for providing accurate sensory signals (via muscle spindle and Golgi tendon activation). Through observing (once again with the ultrasound technique) the surrounding muscles of the ankle joint, Loram and colleagues (Di Giulio, et al., 2009) suggest that the deep compartment of the tibialis anterior muscle (muscle spindle information) inputs a
significant source of proprioceptive information for the regulation of balance control. The Golgi tendon organs also play another role in maintaining balance control. As stated above the Golgi tendon organs provide sensory information regarding the level of muscular force produced in a muscle. During passive swaying and inactivated muscular activity (Proske & Gregory, 2002) (of the postural muscles in the ankle joint) the Golgi tendon organs would likely be capable of providing adequate sensory information to contribute to maintaining balance control (Di Giulio et al., 2009). These authors are cautious to remind that the tibialis anterior is not always the primary source of information for balance control. Balance control muscle coordination is a dynamic process with muscles potentially reversing roles as the CoM changes in relation to the BoS (Di Giulio et al., 2009).
In a commentary on these paradoxical muscle contractions published in the Journal of Applied Physiology, Fitzpatrick and Gandevia (2005) highlighted the significance of this work. They suggested that prior to this information, normal body sways were thought to occur from external perturbations and reduced sensory information. They now suggest that a significant cause of the observed body sway is a result of the ‗catch-and-throw ballistic muscle activation‘ that Loram and colleagues recorded. In their estimation, there is a
significant contribution from higher centers in the CNS and the cerebellum is potentially where this control occurs and that it acts in a predictive manner
(Fitzpatrick & Gandevia, 2005).
In summary, there are several different models of balance control regulation such as the stiffness model (primarily passive), the feedback model (with sensory integration) and the most recent method of balance control that is known as an intermittent control of standing balance (Bottaro, et al., 2008; Loram, et al., 2011; Morasso & Sanguineti, 2002; Peterka, 2002; Peterka & Loughlin, 2004).
1.3 Cognition and balance control
Experimental trials that investigate the role of attention/cognition on balance control have demonstrated evidence to support that balance control is not simply an automatic task but that it has a cognitive contribution. In a review article by Fraizer and Mitra (2008) the body of work performed on cognition and balance control is separated into two categories. The first category contains studies that show cognition is affected when balance is
perturbed (either mechanically or visually). The second category contains studies that show balance can be perturbed, but is not always, by simultaneously performing cognitive tasks. Here, we describe work from both categories.
Andersson et al., (2002) designed a study to investigate the effect of cognitive load on postural control using a 2 x 2 design of conditions with and without cognitive loading and vibratory calf stimulation. The cognitive loading consisted of backward counting as fast and as accurately as possible (step size of 7) for twenty seconds. Balance control was measured with the mean anterior-posterior and lateral torque variance. A summative score was given to the cognitive task outcomes and it was found that when postural control was disrupted by calf vibratory stimulus (increased anterior-posterior and lateral mean torque variance) cognitive task performance worsened. These authors suggested that their results indicated that balance control and cognitive processing share similar resources. In a study conducted by Teasdale et al., (1993) it was found that as the sensory information available was reduced (vision/no vision and normal/foam surface) postural task performance
decreased in the elderly, but not the young subjects, and more cognitive processing was evidenced through increased reaction time. There are several other studies that support
these results and are detailed in reviews by Fraizer and Mitra (2008) and Woollacott & Shumway-Cook (2002).
The studies that investigated if balance control can be perturbed by performing cognitive tasks do not show the same sort of consensus as those studies that show
disturbing balance negatively affects the performance of cognitive tasks (Fraizer & Mitra, 2008; Prado, Stoffregen, & Duarte, 2007). In general, it requires challenged balance control to observe a decrease in cognitive task performance. For example, a study performed by Mitra (2003) that used a classical conjunction search to modify cognitive loading during two different foot postures (open -10cm apart and closed – feet pressed) found that participants swayed more (increased medio-lateral and anterior-posterior sway) as the cognitive task load increased. However, not all studies show this sort of association, for example a study performed by Siu and Woollacott (2007) found no differences in balance control (mean total CoP path length) between three different (and increasingly difficult) cognitive tasks. The subjects were young healthy individuals and the cognitive task
consisted of a visual spatial memory task. It appears that despite decreased performance in the cognitive task balance control was unaffected. Some of the inconsistencies in the literature possibly stem from limitations in the experimental design of these ‗dual-task‘ studies. Fraizer and Mitra (2008) point out that there are several limitations to these studies that are often overlooked such as the reference or baseline comparison values, task
prioritization (instructions giving to participants) and the different quantification of balance control. Differences in any of these three aspects of the experimental design may partially account for the lack of consensus in the literature for dual-task studies (Fraizer & Mitra, 2008). Despite these limitations the dual-task paradigm is useful for revealing important cognitive and CNS contributions towards balance control.
Understanding that the CNS contributes to balance control also comes from studies that measure brain activity and balance control (Goble et al., 2011) as well as movement analysis of individuals that have brain lesions and injuries (Lalonde & Strazielle, 2007; Takakusaki, Oohinata-Sugimoto, Saitoh, & Habaguchi, 2004; Visser & Bloem, 2005). Compelling evidence is provided by clinical neurological studies that show balance control impairments associated with neurological disorders. For example, in individuals that have lesions in their basal ganglia balance impairments are commonly found. Parkinson‘s
disease is one of the most common examples of a lesion in the basal ganglia (substantia nigra). With Parkinson‘s disease there is a multitude of balance impairments that are apparent, for example, falling is common with more than 50% of individuals with Parkinson‘s falling two or more times a year (Balash et al., 2005). Other examples of impaired balance control in parkinsonians are a marked difficulty to turn about the vertical axis and also a characteristically stooped posture (Visser & Bloem, 2005). In addition, individuals with spinocerebellar ataxias are also characterized by impaired balance control (Van de Warrenburg, Bakker, Kremer, Bloem, & Allum, 2005).
It was once thought that balance control was modulated by spinal reflexes (Winter et al., 1998) and spinal reflexes are known to act independently of the brain. As our
understanding of balance control has moved forward from a simple reflex controlled model to one that involves higher cognitive processes so does our appreciation of the role the brain has in balance control (Jacobs & Horak, 2007; Whelan, 2009). It is important to consider a whole body approach to balance control and this includes the CNS.
1.4 Modes of control
The CNS controls standing balance and its controlling actions can be separated into two primary modes of control. These modes are known respectively as anticipatory and compensatory (Maki & McIlroy, 1997) with the compensatory control also sometimes known as feedback mode (Whelan, 2009). Both modes of control attempt to contain the CoM within the boundary of the BoS. Anticipatory control is often associated with voluntary movements and adjustments can be made in an anticipatory manner in order to counter the imbalance that is predicted to occur. A common term in the research literature for describing anticipatory control is anticipatory postural adjustments (APAs).
Anticipatory control is also considered an automatic process that is formed through learning and needs little direct attention. Compensatory control is often a response to an external unexpected perturbation and it is more associated with cognitive processing. Together, these modes of control help anticipate and respond to perturbations with the
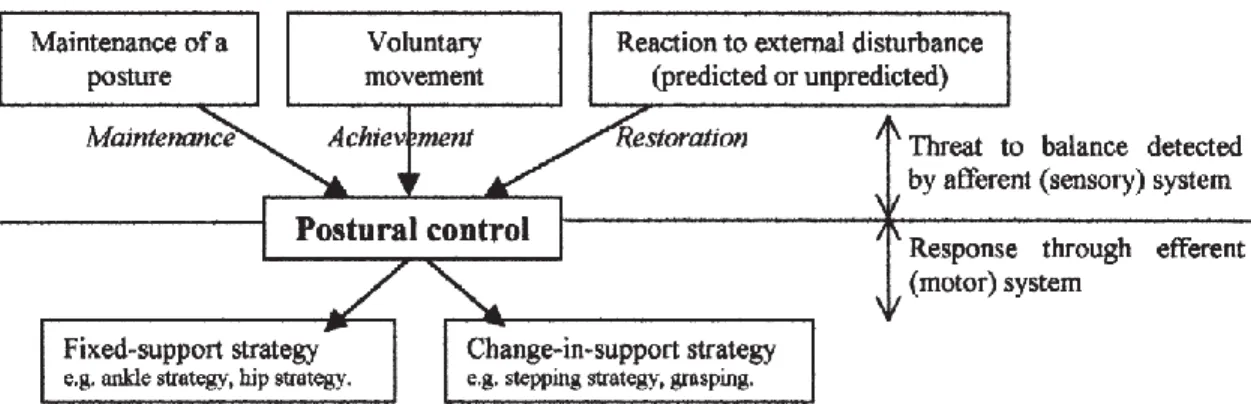
ultimate goal of maintaining balance (see Figure 2 for a summary).
Figure 2 – summary of the different modes of control. Adapted from Pollack, Durward, Rowe and Paul (2000).
1.4.1 Fixed support strategies and change in support strategies
Fixed support strategies are usually defined as static standing balance with no changements in the BoS.The simplest model of upright standing balance control, in a fixed support situation, is that of the inverted pendulum with body rotations occurring around the ankle joint (Smith, 1957; Nashner 1976) in a fixed stance. This is reductionist and only considers one degree of freedom (anterior-posterior). This model considers the ankle as the primary axe of rotation for small perturbations and firm support surfaces. The hip has also been identified as contributing towards stabilization, particularly during larger
perturbations or on compliant surfaces (Horak & Nashner, 1986). Both strategies can be used as a means of balance control. It is also commonly accepted that during double limb support the ankle, knee and hip all have contributory roles (Kepple, Siegel, & Stanhope, 1997). Perturbations are often used to examine balance responses because it is presumed that they reveal the compensatory mode of balance control (Gatev et al., 1999). Horak and Nashner (1986) used an experimental setup that modulated the length of the surface support and incorporated forward and backward support surface perturbations into their study design. They found that the ankle strategy was primarily used for balance control during the backward and forward surface support perturbations while standing on a normal length platform. However, the hip strategy was primarily used for balance control (during the same perturbations) when the surface support was shorter in length. In a study performed by Hwang et al. (2009), on an unstable surface, forward perturbations at two different speeds were used to examine the strategies used in a compensatory manner. It was found
that the ankle strategy was used for the slow speeds (0.1m/s) and that a combined ankle and hip strategy were used for the faster speed (0.2m/s) perturbations. In a study performed by Sasagawa et al. (2009), that investigated the contributions from the hip joint towards balance control during quiet standing, no clear correlations were found between the CoM movements and the ankle and hip joint displacements. When the CoM movements were compared with the accelerations of the ankle joint it showed a poor tracking of the CoM. However, upon integrating the hip joint accelerations into the model (combined hip and ankle) a much better CoM tracking was apparent. This suggests that the hip joint contributes in a significant manner towards standing balance control (Sasagawa et al., 2009). These authors refer to the combination of ankle and hip joint movements for anterior-posterior balance control as a double-link inverted pendulum.
There also exists ‗change in support strategies‘ for compensatory balance control (Maki & McIlroy, 1997). These strategies encompass the hip and ankle strategies Changes in support strategies require a change in foot position or upper limb movements in order to maintain balance control (Maki & McIlroy, 1997). Maki and McIlroy (1997) reviewed the literature on ‗fixed in support strategies‘ and ‗change in support strategies‘. Readers are encouraged to consult this review as this topic is not directly relevant to this thesis and is therefore not covered in detail.
In summary, it appears that humans have several strategies available to regulate balance control and that it is adjustable in nature. This concept is referred to as redundancy and explains the flexibility and adaptability of human motor control under many different conditions (Franklin & Wolpert, 2011).
1.5 Sensory contributions to balance control: vision
As mentioned briefly, the information for processing in the CNS comes from three sensory systems; the visual, vestibular and somatosensory systems. Each of these systems provides complimentary information that contributes for balance control regulation. The vision effect of balance control is one of the most common observations in the balance control literature, that is, balance control is reduced when visual information is removed (Day, Steiger, Thompson, & Marsden, 1993; Edwards, 1946; Paulus, Straube, & Brandt, 1984). In a study completed by Bles et al., (1980) that investigated the effect of the distance
of a visual cue on balance control, it was found that at distances up to 5m there is a linear increase in balance control disturbances (measured by RMS in both medio-lateral and anterior-posterior directions). More sway disturbance was observed in the fore/aft direction than the lateral and from 5 to 75 m there were no discernible greater effects of visual cue distance on balance control perturbation. In a similar manner, it has been found that increases in body oscillations can be provoked by varying the visual stimulus. Using a projected linear vection scene, Lestienne et al. (1977) demonstrated the occurrence of a marked postural readjustment in 80% of their subjects (n=30). The postural readjustments were changes in body inclination in the anterior-posterior direction that corresponded directly to the direction of vection (forwards or backwards).
Modulating the amount and type of vision also affects balance control in a
predictable manner (Buchanan & Horak, 1999; Guerraz & Bronstein, 2008). For example, Buchanan and Horak (1999) used translational platform displacements to observe that during fast frequencies (1.0 and 1.25 Hz) vision was used for fixing the head in space and maintaining CoM within the BoS. At the slowest frequencies (0.1 and 0.25 Hz) vision was less important and presumably proprioceptive elements from the lower limbs contributed adequately towards stabilizing the CoM within the BoS. It is suggested that the visual contributions become more important when the balance control conditions become more challenging. In addition, Guerraz and Bronstein (2008) found visually induced postural responses in response to vection (visual stimulus that simulates movement) in ten healthy subjects. Specifically, they found that vection produced an increase in the mean and
standard errors of lateral body translations (measured with a marker on C7). In summary, it appears that vision (eyes open or eyes closed) and the type of visual cue affects balance control in a predictable manner. This suggests that vision is an important sensory contributor towards standing balance control.
1.5.1 Sensory contributions to balance control: vestibular
The main role of the vestibular system is to provide information about body position and body orientation in response to changes in movement, specifically those that involve accelerations and decelerations (Corso, 1981). In a study that measured postural reflex responses in normal healthy individuals and compared them to individuals who displayed
hypo- and hyperfunction of their vestibular system it was found that the vestibular system contributes to modifications of muscle tone and postural reflexes (Molina-Negro, Bertrand, Martin, & Gioani, 1980). The vestibular system also helps maintain balance and posture; it involves coordinating information about the position of the head and eyes. Head motion is detected and adjustments are made to maintain visual stability in moving and stationary surrounding environments. Peripheral vestibular organs located in the inner ear coordinate both angular and linear motions of the head and this permits coordinated and stable vision and perceptions of body orientations, that is, when these systems are fully intact and functional (Walther & Westhofen, 2007).
During dynamic tasks the vestibular inputs contribute important sensory
information. Known thresholds for movement detection with regards to the axes of the vestibular organs are 0.003 rad at a velocity of 0.001 rad • s-1. It has also been shown that as movement velocity increased (three fold) the movement detection thresholds shifted
downward and smaller movements were detectable (Fitzpatrick & McCloskey, 1994). Space flight re-entry studies suggest that the principal role of the vestibular system is the detection of gravitational vector (Black, 2001). Upon the astronauts reintroduction into an environment with gravity there is a period of adaptation that they undergo before resuming normal postural control. Experienced astronauts appear to adapt at a quicker rate than novice astronauts. Ground based studies show that the reference position and
magnitude of the gravitoinertial vector are used as a reference for the CNS (Kaufman, Wood, Gianna, Black, & Paloski, 2001). Kaufman et al. (2001) exposed nineteen healthy subjects and eight vestibular deficient subjects to a centripetal acceleration of 1g (9.81 m •s2) for ninety minutes on a centrifuge (0.8 m) in order to understand how the vestibular system adapts in rotating environments. CoP was affected in the normal healthy subjects post centripetal accelerations, however, this was not found in the vestibular deficient subjects suggesting the important contributions of the vestibular system as a reference for balance control.
Although the vestibular system has an important role in movement, during static upright standing balance control, its role is minimal (Fitzpatrick & McCloskey, 1994; Fitzpatrick, Rogers, & McCloskey, 1994). Fitzpatrick et al. (1994) designed an
vestibular system during standing balance control. Condition A was a control condition where the subjects stood still on a custom designed platform that measured body sway (ankle movements were taken as a measure of body sway) with a spring attached to a strain gauge and on the lower limb (i.e., below the knee). Condition B was a splinted condition were the subject was strapped to a board in order to prevent body movement (inhibit vestibular contributions) and an equivalent body mass was attached to the individual‘s ankles and controlled by their ankle movements. This setup was designed to simulate an inverted pendulum. Condition C had the individual splinted but in a different way than in condition B. In condition C the individual was splinted such that the joints (ankle, knee and hip) were secured to minimize movement at these points but the body was still able to move and thus use vestibular information for regulating balance control. In this experiment the subjects were able to control an equivalent body mass without vestibular, visual inputs and feet proprioception (Condition B – eyes closed – feet anesthesized). The authors argued that this suggests balance control can be maintained with only sensory information from the lower leg muscles and that vestibular input does not contribute significantly during quiet standing balance.
For individuals with deficits in the other sensory systems, the vestibular system may act in a compensatory manner (Horak, 2006; Horak & Hlavacka, 2001). Horak and Hlavacka (2001) investigated vestibular contributions during standing balance control in healthy individuals and those with peripheral neuropathy. To vary vestibular contributions four different levels of vestibular galvanic stimulation were used. The peripheral
neuropathy participants showed greater CoP displacement (anterior-posterior) than the control subjects during galvanic stimulation and especially at the greatest intensity. These authors suggest that this shows an increased sensitivity to the galvanic stimulation and that this is because the vestibular system is more sensivitive in the peripheral neuropathy individuals in order to compensate for their somatosensory loss. This adaptive nature suggests that the vestibular system plays a role and that its contributions can be modulated when necessary. For example, the vestibular system contributions also become more important in conditions that are increasingly unstable, particularly when vision and touch are reduced (Horak, Buchanan, Creath, & Jeka, 2002). Horak et al. (2002) used platform translations (12 cm) and rotations (± 1.2°) at different frequencies in bilateral vestibular
loss patients and then compared their anterior-posterior displacement of the trunk, head and index finger as well as their anterior-posterior CoP excursion with age-matched controls. The vestibular impaired individuals displayed more anterior-posterior trunk displacements and CoP excursions when compared with the age-matched controls.
From these studies it appears that the vestibular system has an important input into standing balance control during dynamic tasks however it is still unsure how important the vestibular contributions are during static upright standing. This is evident from dynamic experimental trials that attempt to remove (or confuse) the vestibular information as balance control is generally impaired. Evidence that the vestibular system contributes to balance control also comes from studies involving vestibular loss patients. In summary, it appears that the vestibular system is capable of adapting to different environments and that the gravity vector is the primary reference for the vestibular system orientation during balance control. However, during upright standing balance in healthy individuals its role is thought to be minimal.
1.5.2 Sensory contributions to balance control: somatosensory
The somatosensory system is not a specific system with dedicated organs or a system that resides in a specific region of the body as do the visual and vestibular systems. The somatosensory system has a presence throughout the entire body and is involved in many body functions. For example, sensory receptors can be found in the skin, joints and bones. Its primary role is to sense changes in joint kinematics. As the body responds to changes in our environment that threaten our homeostatic state appropriate responsive actions are executed. In the CNS, the primary area of sensory processing occurs in the somatosensory area that is located in the contralateral hemisphere. This sensory
information is then transferred from sensory area of the cerebral cortex to the motor area. The motor area can be divided into two main areas, the supplementary motor areas and the primary motor cortex. The supplementary motor areas are responsible for selecting what voluntary movements to perform while the primary motor cortex is responsible for
executing the motor commands. The cerebellum is responsible for fine tuning the planned movements with the actual movements resulting in appropriate motor responses (Medina & Coslett, 2010; Serino & Haggard, 2010). There are a great variety of functional units of the somatosensory system and these are distributed throughout the body. Some examples
include, but are not limited to, baroreceptors (pressure), mechanoreceptors (pressure), nociceptors (pain), proprioceptors (position and velocity), and thermoreceptors (temperature). Each of these receptors has its own function and provides unique and important information for central processing, reflex modulation and can contribute to balance control, where appropriate. The receptors that are most relevant to balance control in normal conditions are stretch receptors (muscle spindles and Golgi tendon organs), joint receptors and cutaneous mechanoreceptors (Latash, 2008; Maurer, Mergner, & Peterka, 2006; Mergner, Maurer, & Peterka, 2002; Windhorst, 2007). In an extensive review on this subject Windhorst (2007) suggested that the sensory receptors for balance control be classified into two main categories, main load receptors and accessory load receptors. Within the main load receptors there are two classifications i) true load receptors which are the Golgi tendon organs in the lower limb muscles and, ii) body support receptors which are the cutaneous mechanoreceptors in the plantar sole. For the accessory load receptors there are also two types of receptor classifications, these are i) neuromuscular receptors that are the muscle spindles from the lower limbs and, ii) joint receptor afferents which are composed of the Ruffini endings and Pacinian corpuscles. These all contribute in an important manner to standing balance control. In essence, these sensory receptors all provide information that is processed and if this information is adequate, standing balance control is maintained. These sensory signals all contain some degree of noise, have
potential shifting activation/deactivation thresholds and provide feedback for appropriate re-weighting (sensory re-integration) of the signals if required (Maurer et al., 2006). In short, these provide a wide variety of information that is coordinated and combined with the other sensory systems for adequate balance control.
1.5.3 Sensory contributions to balance control: cutaneous mechanoreceptors
The plantar sole contains sensory receptors that contribute to standing balance control. These sensory receptors primarily respond to mechanical stimululation. There are many different sensory receptor types: Merkel cells, Meissner corpuscles, Pacinian corpuscles, Ruffini receptors, and free nerve endings are the primary receptors (Vega, García-Suárez, Montaño, Pardo, & Cobo, 2009). There exists a variety of sensory receptors because of the many different functions they provide. For example, they provide
information on the quality, magnitude and location of tactile stimuli (Ribot-Ciscar, Vedel, & Roll, 1989). Using microneurography research techniques Inglis and colleagues (Inglis, Kennedy, Wells, & Chua, 2002; Kennedy & Inglis, 2002) investigated the role of the cutaneous receptors in the foot as well as their distribution and behaviour. These authors found that the afferent inputs from the plantar sole mechanoreceptors provide useful information for balance control and walking. In terms of their distribution and behaviour, approximately 70% of the mechanoreceptors in the plantar sole were fast adapting (type Fast Adapting I & Fast Adapting II), the remaining were slow adapting (Slow Adapting I & Slow Adapting II) (see Figure 3).
Figure 3 – plantar sole mechanoreceptor distribution. From Kennedy PM, Inglis JT, J Physiol 2002, 538(Pt. 3):995-1002.
Balance control requires continuous sensory information being relayed from the plantar sole and processed in the CNS. The high percentage of FA type mechanoreceptors in the plantar sole seem a natural fit for performing this sensory role. As these sensors are distributed throughout the soles of the feet, and are particularly dense in sections of the plantar sole that are in constant surface contact (e.g. heel), they may provide sensory information necessary for higher centers in the CNS to create a pressure distribution map within the body‘s BoS. In a similar manner, when describing possible active mechanisms of support, Morasso and Schieppati (1999) also highlight the potential importance of the plantar sole mechanoreceptors in standing balance control. They say that the plantar sole
cutaneous receptors perform three functions that are related to the ground reaction force vector: 1) the vertical antigravity force vector, 2) the horizontal force component (shear forces), and 3) the projection of the centre of mass in relation to the BoS. All three of these functions provide important information for the active regulation of balance control. The shear (horizontal) force vector is smaller when compared with the vertical vector but it is still detectable by the plantar sole mechanoreceptors, as the changes in the shear forces are proportional to the COM-COP difference then the receptors need to be responsive to a stimulus that is continuous and rapidly adjusting. The most common type of
mechanoreceptor in the plantar sole is fast adapting. In light of this discovery, these mechanoreceptors seem appropriate for performing the rapid sensory detections of a constantly moving CoP. The Pacinian corpuscles have been suggested as the primary mechanoreceptor to fill this role (Morasso and Schieppati, 1999).
A significant amount of work has been done on the roles of the various sensory systems during standing balance control. The principal means of advancing the
understanding of their contributions is often through attenuating or stimulating the sensory system (e.g., cooling the plantar soles to attentuate the cutaneous mechanoreceptors sensory feedback or high frequency tactile vibration appled to the feet) and then observing changes in balance control (Horak, 2006).
1.5.3.1 Plantar sole sensory inhibition
There exists a wide variety of methods used to identify the contributing role of the plantar mechanoreceptors to maintaining balance control. Several methods have been proposed to achieve sensory inhibition including cooling the plantar sole, foam
posturography, ischemic anaesthesia and pressure cuffs. In order to stimulate the sensory feedback from the plantar sole one can apply a vibratory stimulus, heat, white noise and spiked insoles. Each of these methods has advantages and limitations. Below we describe some of the available literature and the insights these studies have provided into the plantar sole contributions to balance control.
Cooling the plantar sole is a common method to inhibit the sensory feedback by increasing the sensory threshold for stimulus detection (Magnusson, Enbom, Johansson, & Pyykkö, 1990; McKeon & Hertel, 2007a; McKeon & Hertel, 2007b; Patel et al., 2011;
Schlee et al., 2009; Stål et al., 2003). It is also sometimes referred to as hypothermic
ischemia. The mechanism responsible for the increased sensory threshold is thought to be a reduction in the gain of the mechanical to electrical stimulus transmissions. It is not thought to affect the impulse transmissions that occur with the nerve endings. In general, it is
expected that an increase in the sway path will be observed when the plantar sole is cooled. The results in the literature are clear with regards to the effect that cooling has on the sensitivity of the plantar sole. However, this reduced sensitivity does not directly translate into reduced balance control. McKeon and Hertel (2007), with cooled feet and no vision condition, showed a reduction in COP excursion area and no changes in traditional COP sway parameters. While Patel et al., (2011) found that cooling the plantar sole lead to approximately a 200% reduction in cutaneous vibratory detection but no differences were observed for monofilament testing. They interpreted these results to indicate that the pressure detection of the plantar sole is still intact when cooled and it can contribute
adequately to balance control regulation. It seems that cooling the plantar sole is a means of changing the vibratory perception but this does not affect standing balance control. This seems counterintuitive considering that it has been suggested that the majority of the mechanoreceptors in the sole are fast adapting and these are most likely to contribute to updating balance control (Inglis et al., 2002; Kennedy & Inglis, 2002).
Using a foam standing surface is also another means of altering the sensory
information coming from the plantar mechanoreceptors. Arguably this is the most common method used as sensory inhibition in standing balance control (Patel et al., 2011). It has been suggested that using a foam standing surface inhibits our sensation of foot pressure change and distribution (Wu & Chiang, 1997) and thus affects our sense of orientation (Patel, Fransson, Lush, & Gomez, 2008). In addition, the foam surface also reduces the efficiency of intermittent (active and passive elements) standing balance control regulation by reducing the stiffness of the standing surface as this will impact on the transfer of energy between the body and the surface. The foam characteristics are important to consider when measuring its impact on standing balance control. Patel and colleagues (2008) measured the impact of three different foams (characterised by the measure of their elasticity) on
standing balance control. Using the frequency of body movements to quantify balance control they showed a difference between the three foams for both the high (greater than
0.1 Hz) and low (less than 0.1Hz) frequency ranges of the body movements. This further demonstrates complications with the comparison of results between protocols that do not use foam with the same physical characteristics.
Ischemic anaesthesia, as a method of plantar sole inhibition, can be performed two ways; it can be induced by an injection of medication that reduces the sensation in the plantar sole or it can be induced a pressure cuff that reduces circulation to the feet (Diener, Dichgans, Guschlbauer, & Mau, 1984; Mauritz & Dietz, 1980). Diener and colleagues (1984) used a platform that swayed at low frequencies (0.3 Hz and below) and high frequencies (greater than 0.3 Hz) to test the effect that reduced afferent proprioceptive information had on the maintenance of balance control. They found that for the low frequencies, reduced sensation below the ankle greatly affected the balance control of individuals (many of their subject‘s fell). For the high frequencies, it appeared that information from above the pressure cuff was sufficient for maintaining balance control, presumably from muscle receptors in the trunk and neck. Mauritz and Dietz (1980) used ischemia and an eyes closed condition to reduce proprioceptive inputs from the legs and vision, they subsequently measured balance control. Using Fourier transforms on the body sway oscillation data a 1Hz sway was observed in the anterior-posterior axis. This sway (in the absence of ankle proprioceptive and visual feedback) suggests that the vestibular system acts in a compensatory manner to maintain balance control when proprioceptive inputs are limited. There are two main limitations with using ischemia to reduce sensory input i) it does not only remove the tactile elements of the plantar sole but it also removes proprioceptive information from the muscles and tendons (Kavounoudias, Roll, & Roll, 1998) and ii) it alters muscle contraction.
1.5.3.2 Plantar sole sensory stimulation
The second means of understanding the sensory contributions to standing balance control comes from studies that stimulate the plantar sole and observe the differences in balance control. Kavounoudias et al. (1998) used mechanical vibration (100 Hz) to activate the planter mechanoreceptors. These authors observed changes in body tilt that were opposite in direction to the areas of the foot that were stimulated. These results were later repeated by the same authors using mechanical vibratory frequencies ranging from 20-80
Hz (Kavounoudias, Roll, & Roll, 2001). In addition, these authors suggested that ankle muscle proprioception and plantar sole proprioception act in a complimentary manner during balance control regulation. The upwards limit of detectable vibratory stimulus in the plantar sole is thought to be around 250 Hz (Schlee, Reckmann, & Milani, 2012). More recently, this effect has also been observed using plantar sole vibration and ankle tendon vibration to show that the spindle afferents in these areas contribute to standing balance control (Thompson, Bélanger, & Fung, 2011).
Similar to a mechanical vibratory stimulus textured surfaces such as spiked insoles that are in contact with the plantar sole have also been used as a means of stimulating the plantar sole mechanoreceptors during standing balance control (Corbin et al., 2007; Maki et al., 1999; Palluel et al, 2008; 2009; Watanabe & Okubo, 1981). Presumably the mechanism of action is stimulated proprioceptive (increased sensory information) receptors on the soles of the feet lead to neuromuscular changes that result in altered balance control. A change in balance control with the application of spiked surfaces has been observed during gait (Kelleher et al., 2010; Nurse et al., 2005) but this has not been shown during standing balance control for a young asymptomatic group (Hatton et al., 2009; 2011). This may be a result of standing balance control being too easy of a task for these individuals. A positive effect of spiked insoles has been demonstrated in elderly persons (Maki et al., 1999; Palluel et al., 2008; 2009). Palluel et al. (2009) showed that in a group of heathy elderly
participants (n=19) five minutes of standing with spiked insoles (increased tactile
sensitivity enhancement) improved measures of postural sway. Specifically, these authors found decreased CoP surface and anterior-posterior root mean square post insoles. Similar results were found in healthy young controls although not to the same extent suggesting potential sensory reweighting difficulties in the elderly persons or that the sensory thresholds are higher in the elderly and therefore do not respond in the same way as the younger individuals.
From these studies it is clear that the plantar sole contributes to balance control during upright standing. It is important to not become trapped into thinking that any one factor or mechanism causes reduced balance control. Using an approach that looks at the entire system as a functional unit will provide the best information for understanding how the plantar sole contributes to balance control (Woollacott, 2007).
1.6 Balance control measurement: CoM and CoP displacements
The displacement of the centre of mass (CoM) or the displacement of a highly correlated measure (i.e., a projection of the CoM) known as the centre of pressure (CoP) (Balasubramaniam & Wing, 2002; Ruhe, Fejer, & Walker, 2010) offer reliable and valid measures for assessing balance control. Both of these methods are commonly used as a measure of balance control.
The CoM is a point in space that represents the sum of the CoM of the body segment inertial parameters (Gard, Miff, & Kuo, 2004; Winter, 1995). It is a measure of balance control and is known as the controlled variable that represents the body‘s sway. The balance control system‘s main function is to control the CoM within the BoS in order to maintain balance. The CoP represents the point of application of the average measured pressures that are redistributed across the plantar sole that result from ground reaction forces applied during quiet standing. The CoP is not to be confused with the centre of gravity (CoG) as the CoG represents the vertical ground projection of the CoM
(Winter, 1995). There is a CoP under each foot and there is a net CoP. To measure each individual CoP two force platforms are necessary whereas to measure the net CoP only one force platform is required. Researchers generally use the net CoP because it can be
measured with a single force platform and if an inverted pendulum model is adopted it accurately captures the body‘s balance control and provides insights into the modes of control. The CoP under each foot provides interesting information in specific populations that have exhibit pathologies or disabilities exhibiting asymmetries of the lower limbs. The CoP is measured because it gives us information about how the body controls the
placement of the CoM (and the CoG). The CoP over and undershoots the CoM (CoG) movements because its actions reflect the control of the CoM (Lafond, Duarte, & Prince, 2004). Over a longer period of time the CoP and CoG mean trajectories are equal.
Measuring the CoM is a complex process that usually involves many body markers and multiple cameras to assess each of the body segment parameters and calculate the body‘s global CoM. This method is precise and is usually considered to give the best approximation of the body‘s true CoM (Hof, 2005; Winter et al., 2003). Markerless motion capture systems are also in development and offer promising initial results (Corazza et al., 2006; Corazza & Andriacchi, 2009). In a short communication published in the Journal of
Biomechanics Corazza and Andriacchi (2009) describe how to perform a markerless motion capture that provides a 3D representation of a human. These authors used eight VGA cameras to create a model (‗visual hull‘) and calculated the center of mass by assuming that the body had equal density throughout all of the segments and therefore found the center of the body volume of each segment as representative of the CoM. In order to verify their technique they compared the measurements of the CoP (derived from the markerless motion capture CoM) with the CoP measured by a force platform and found strong correlations (R>0.90) between both values.
Another method for measuring balance control was developed by Zatsiorsky and King (1997) is called the ‗zero-point-to-zero-point double integration method‘ and calculates the CoM from CoP force platform measures. There is a five step calculation process to their method (Zatsiorsky & King, 1997). For this method, it is assumed that when the horizontal ground reaction forces equals zero the system is stable (CoP and CoM are in sync). This method was validated using videography during one-legged stance. One-legged stance increases the CoM displacements normally observed during double-leg stance. Yet another method was developed to estimate the CoM of the body from CoP measurements (Caron, Faure, & Brenière, 1997). This method is also known as the low pass filter method (LPF) and the estimated horizontal CoM is computed by running a low pass filter on the CoP frequency signal (Fast Fourier transformation). Lafond et al. (2004) compared the ‗zero-point-to-zero-point double integration method‘, the low pass filter method (LPF) and the kinematic method. CoP measures were taken with a force platform and CoM measurement was performed with a 13 segment anthropometric model. These authors found a better agreement between the kinematic method and the LPF method than the ‗zero-point-to-zero-point double integration method‘ and the kinematic method. These other methods can be accurate and valid depending on the context and research questions. It is also possible to use the difference between the CoM and CoP (CoM-CoP) as a measure of balance control (Yu et al., 2008). This difference is thought to represent the error or overcorrection in the balance control system and causes the horizontal
displacements of the CoM. Furthermore, the CoM accelerations are also highly correlated with the CoM-CoP difference and are able to discriminate between different populations (Yu et al., 2008), suggesting another method to assess balance control.