Three Essays on Spatial Health Econometrics
Thèse
Bodel Aymele Gnintedem
Doctorat en économique
Philosophiæ doctor (Ph. D.)
Three Essays on Spatial Health Econometrics
Thèse
Bodel Aymele Gnintedem
Sous la direction de:
Guy Lacroix, Directeur de recherche Jean Dubé, Co-directeur de recherche
Résumé
Cette thèse présente trois essais sur l’économie de la santé de la population québécoise, y compris la santé des nouveau-nés. Elle introduit dans les analyses les outils de l’économétrie spatiale en apportant une attention particulière à la corrélation spatiale entre les caracté-ristiques socioéconomiques (notamment le revenu) et de la santé des individus (obésité) et des nouveau-nés. L’unité d’analyse c’est les secteurs de recensement et les individus vivants dans la province du Québec. Dans notre étude nous proposons une analyse beaucoup plus fine des déterminants du revenu et des résultats de santé chez les nouveau-nés. La principale motivation de notre recherche vient du fait qu’il est généralement admis que la consommation des services de santé et des biens néfastes pour la santé varient de façon significative avec le revenu des individus. Les individus plus riches ou plus pauvres auront tendance à consommer plus ou moins ces biens et services. Cependant, le revenu lui-même varie dans le temps et dans l’espace. Ces dimensions spatiales et temporelles doivent être prises en compte dans la modélisation des relations entre des caractéristiques démographiques, socioéconomiques et la santé des individus. L’introduction d’une analyse spatio-temporelle dans les questions d’éco-nomie de la santé nous permettra de tenir compte des corrélations spatiales et temporelles afin de mieux estimer et déterminer les raisons probables de la variation de nos variables d’intérêt selon l’échelle géographique des différentes études. D’un point de vue politique, cette approche permettra à l’avenir d’anticiper et de prendre des mesures préventives en ce qui concerne la santé de la population québécoise. La modélisation de l’état de santé innove en ce qu’elle intègre les caractéristiques de l’environnement immédiat des individus de même que les corré-lations spatiales dans les caractéristiques inobservables. Ces deux volets des déterminants de la santé sont généralement négligés ou omis dans des études économiques et économétriques portant sur les questions de santé publique.
L’objectif principal de cette thèse est donc d’introduire la modélisation des interactions spatiales dans l’analyse des questions de santé publique. L’idée étant que, comme le stipule la première loi de la géographie, tout interagit avec tout mais deux choses voisines ont plus de chances d’entrer en interaction que deux choses lointaines. Les chapitres de cette thèse sont liés par l’intégration d’une dimension spatiale dans l’analyse des corrélations. De façon spécifique, le premier chapitre s’intéresse à la relation entre l’obésité, mesuré à travers l’indice
de masse corporelle (IMC) et les résultats du marché du travail (revenu et nombre d’heures travaillées) dans une perspective spatio-temporelle. Nous utilisons les données de l’Enquête Nationale sur la Santé de la Population (ENSP). Les résultats de ce chapitre nous permettent de constater la présence au Québec d’une corrélation entre le revenu des individus et ceux de leurs voisins. Cela montre l’influence spatiale que le voisinage a sur un individu. La non prise en compte de cet aspect aurait pu conduire à une conclusion incorrecte sur la relation entre le niveau de revenu et l’obésité. Ceci nous a également permis de tester séparément la présence des deux phénomènes spatiaux que sont l’autorégression et l’autocorrélation en modélisant explicitement le fait que les résidus peuvent être liés entre eux. L’on note également une sous-estimation des effets marginaux du modèle non spatial par rapport au modèle spatial. Cette sous-estimation varie entre 5% et 17%. Un raffinement des estimations a donc été effectué grâce au modèle spatial. S’agissant de la relation entre obésité et les résultats du marché du travail, nos analyses permettent d’observer qu’au Québec, les personnes obèses travaillent plus d’heures que les personnes ayant un IMC normal. L’obésité n’a pas d’incidence sur le revenu des personnes qui y travaillent. Les modèles estimés utilisent des variables dépendantes continues. Le deuxième chapitre évalue la relation entre le revenu du secteur de recensement où vivent les mères et les résultats défavorables de naissance (prématuré et faible poids). Ce chapitre, au meilleur notre connaissance, se distingue de la littérature existante en ce sens qu’il utilise deux modèles différents : en plus d’un modèle probit bivarié spatial, nous utilisons également un modèle spatial SUR, qui est compatible avec l’introduction d’une variable spa-tiotemporelle décalée dans la modélisation. Notre analyse a été réalisée avec les données de nouveau-nés admis et nés à l’unité de néonatologie du Centre Hospitalier de l’Université Laval (CHUL). Nos résultats montrent l’existence d’une corrélation positive entre les nouveau-nés prématurés et ceux ayant un faible poids à la naissance au niveau individuel et au niveau des secteurs de recensements. L’introduction de la variable spatio-temporelle retardée dans la modélisation spatiale SUR montre que l’âge gestationnel décalé dans le temps et dans l’espace affecte positivement l’âge gestationnel des nouveau-nés. Les résultats montrent également que l’âge gestationnel et le poids d’un nouveau-né sont influencés positivement par ceux de leurs voisins. Cela montre l’influence spatiale que le voisinage a sur les mères. Le fait de ne pas prendre en compte l’effet de l’influence de comportements de certaines mères sur d’autres aurait pu entrainer l’omission d’éventuelles corrélations spatiales dans les caractéristiques in-observables qui influencent les résultats défavorables de naissance. Le fait que ces résultats aient été obtenus en estimant un modèle probit bivarié et un modèle spatial SUR indique la robustesse de la corrélation. Une comparaison des résultats du modèle probit bivarié spatial et du modèle spatial SUR a été effectuée. De plus, nous notons que, quel que soit le modèle utilisé dans l’étude, un faible niveau de revenu dans le secteur de recensement est associé à un risque élevé d’accouchement prématuré et de faible poids à la naissance.
Le troisième chapitre traite de la probabilité des nouveau-nés de contracter des infections nosocomiales ou d’être victimes d’incidents médicaux lorsque leurs mères vivent dans la région
métropolitaine de recensement du Québec. L’objectif de ce dernier chapitre est de savoir si l’environnement immédiat de la mère de l’enfant et ses caractéristiques peuvent expliquer les risques associés aux infections nosocomiales et aux incidents médicaux. Ces relations ont été peu analysées dans la littérature. La principale contribution de ce chapitre réside dans le fait que la littérature qui s’intéresse à cette question a très souvent omis de considérer l’impact de la proximité de certaines mères sur d’autres. Ces interactions pourraient avoir des effets sur les infections nosocomiales de leurs nouveau-nés. Nous effectuons notre analyse avec les données du chapitre précédent. Un modèle probit bivarié spatial a également été utilisé pour mieux capter la corrélation entre les incidents médicaux et les infections nosocomiales contractées par les nouveau-nés. Les résultats de ce chapitre nous permettent de constater que les facteurs au niveau des secteurs de recensement qui ne sont pas observés et captés par les effets spatiaux n’influencent pas les infections nosocomiales et les incidents médicaux de façons connexes. Plus précisément, les secteurs de recensement où les nouveau-nés souffrent d’infections no-socomiales ne sont pas susceptibles d’avoir les mêmes nouveau-nés ayant subi des incidents médicaux. Les résultats montrent également que les prématurés et les nouveau-nés de faible poids à la naissance sont plus susceptibles de présenter à la fois des infections nosocomiales et des incidents médicaux. Les nourrissons transférés de la maternité à l’Unité de Soins Intensifs Néonatals (USIN) sont plus susceptibles de contracter une infection nosocomiale et d’expé-rimenter un incident médical. En outre, les enfants nés dans des secteurs de recensement à revenu élevé ont tendance à être moins vulnérables aux infections.
Abstract
This dissertation presents three essays on the health economics of the Quebec population, including newborn health. It introduces the spatial econometrics tools into the analyses, paying particular attention to the spatial correlation between socioeconomic characteristics (notably income) and the health of individuals (obesity) and newborns. The unit of analysis is the census tracts and individuals living in the province of Quebec. In our study, we propose a much more refined analysis of the determinants of income and health outcomes among newborns. The main motivation for our research comes from the fact that it is generally accepted that the consumption of health services and goods that are harmful to health vary significantly with the income of individuals. Richer or poorer individuals will tend to consume these goods and services to a greater or lesser extent. However, income itself varies over time and space. These spatial and temporal dimensions need to be taken into account when modelling the relationships between demographic, socioeconomic and health characteristics of individuals. The introduction of spatial and temporal analyses into health economics issues will allow us to take into account spatial and temporal correlations in order to better estimate and determine the likely reasons for the variation in outcomes of interest across at different geographic scales. From a policy perspective, this approach will allow to anticipate and take preventive measures in the future with respect to the health of the population of Quebec. Health status modelling is innovative in that it integrates the characteristics of individuals’ immediate vicinity as well as spatial correlations in unobservable characteristics. These two components of the determinants of health are generally neglected or omitted in economic and econometric studies of public health issues.
The main objective of this dissertation is therefore to introduce the modelling of spatial interactions into the analysis of public health issues. The idea is that, as stated in the first law of geography, everything interacts with everything, but two things that are close are more likely to interact than two things that are far away. The chapters of this dissertation are linked by the integration of a spatial dimension in the analysis of correlations. Specifically, the first chapter focuses on the relationship between obesity, measured through body mass index (BMI) and labour market outcomes (income and number of hours worked) from a spatiotemporal perspective. We use data from the National Population Health Survey (NPHS).
The results of this chapter allow us to observe the presence in Quebec of a correlation between the income of individuals and that of their neighbours. This shows the spatial influence that neighbourhood has on an individual. Failure to take this aspect into account could have led to an incorrect conclusion about the relationship between income level and obesity. This also allowed us to separately test for the presence of the two spatial phenomena of autoregression and autocorrelation by explicitly modelling the fact that the residuals may be related to each other. In addition, we find that the marginal effects of the non-spatial model were underestimated compared to the spatial model. This underestimation ranges from 5% to 17%. A refinement of the estimates was therefore made using the spatial model. With respect to the relationship between obesity and labour market outcomes, our analyses show that, in Quebec, obese individuals work more hours than individuals with a normal BMI. Obesity has no impact on the income of those who work there. The estimated models use continuous dependent variables.
The second chapter assesses the relationship between income in the census tract where mothers live and adverse birth outcomes (premature and low birth weight). This chapter, to the best of our knowledge, differs from the existing literature in that it uses two different models: in addition to a spatial bivariate probit model, we also use a spatial SUR model, which is compatible with the introduction of a lagged spatiotemporal variable in the modelling. Our analysis was performed with data from neonates admitted and born at the neonatology unit of the Centre Hospitalier de l’Université Laval (CHUL). Our results show the existence of a positive correlation between premature newborns and low birth weight babies at the individual and census tract levels. The introduction of the delayed spatiotemporal variable in the SUR spatial modelling shows that the spatially and temporally lagged gestational age positively affects the gestational age of newborns. The results also show that the gestational age and weight of a newborn are positively influenced by those of their neighbours. This shows the spatial influence that neighbourhood has on mothers. Failure to take into account the effect of the influence of some mothers’ behaviours on others could have resulted in the omission of possible spatial correlations in unobservable characteristics that influence adverse birth outcomes. The fact that these results were obtained by estimates of both the bivariate probit model and the spatial SUR model indicates the robustness of the correlation. A comparison of the results of the spatial bivariate probit model and the spatial SUR model was performed. In addition, we note that regardless of the model used in the study, low income in the census tract is associated with a high risk of preterm birth and low birth weight.
The third chapter deals with the likelihood of newborns contracting nosocomial infections or suffering medical incidents when their mothers live in the Quebec census metropolitan area. The objective of this last chapter is to determine whether the child’s mother’s nearby environment and characteristics can explain the risks associated with nosocomial infections and medical incidents. These relationships have barely been analyzed in the literature. The main contribution of this chapter lies in the fact that the literature on this question has typically
failed to consider the impact of the proximity of some mothers on others. These interactions could have effects on nosocomial infections in their newborns. We conduct our analysis with the data from the previous chapter. A spatial bivariate probit model was incorporated to better capture the correlation between medical incidents and nosocomial infections acquired by newborns. The results of this chapter show that factors at the census tract level that are not observed and captured by spatial effects do not influence nosocomial infections and medical incidents in related ways. Specifically, census tracts where newborns suffer from nosocomial infections are not likely to have the same newborns with medical incidents. The results also show that premature and low birth weight infants are more likely to have both hospital-acquired infections and medical incidents. Infants transferred from the maternity ward to the Neonatal Intensive Care Unit (NICU) are more likely to develop a nosocomial infection and experience a medical incident. In addition, children born in high income census tracts tend to be less vulnerable to infections.
Table des matières
Résumé iii
Abstract vi
Table des matières ix
Liste des tableaux xi
Liste des figures xii
Remerciements xv
Avant-propos xvi
Introduction 1
1 Is There A Private Cost for Obesity in Quebec ? A Spatial Panel Analysis 7
1.1 Résumé . . . 7
1.2 Abstract . . . 8
1.3 Introduction. . . 9
1.4 Literature Review. . . 12
1.5 Presentation of Data and Descriptive Analysis of Variables . . . 18
1.6 Methodology . . . 25
1.7 Empirical Results . . . 28
1.8 Conclusion . . . 33
Du chapitre 1 vers le chapitre 2 35 2 Neighbourhood Effects and Birth Outcomes : A Spatial Analysis. 36 2.1 Résumé . . . 36
2.2 Abstract . . . 37
2.3 Introduction. . . 38
2.4 Literature Review. . . 41
2.5 Data and Descriptive Analysis. . . 47
2.6 Methodology . . . 50
2.7 Empirical Results . . . 55
2.8 Conclusion . . . 62
3 A Spatial Biprobit Model for the correlation Between Nosocomial
In-fections and Medical Incidents in Newborns 66
3.1 Résumé . . . 66
3.2 Abstract . . . 67
3.3 Introduction. . . 68
3.4 Literature Review. . . 71
3.5 Presentation of Data and Descriptive Analysis of Variables . . . 74
3.6 Methodology . . . 78 3.7 Empirical Results . . . 80 3.8 Conclusion . . . 83 Conclusion 85 Bibliographie 89 A 102 A.1 Tables . . . 102 B 104 B.1 Figures . . . 104 C 106 C.1 Figures . . . 106
Liste des tableaux
1.1 Attrition rate from cycle 1 to 3 for the NPHS . . . 19
1.2 Attrition rate from cycle 4 to cycle 9 for the NPHS . . . 20
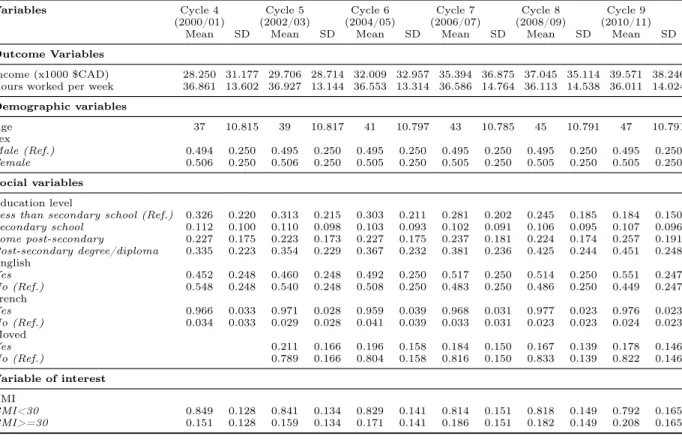
1.3 Descriptive statistics of the selected variables . . . 24
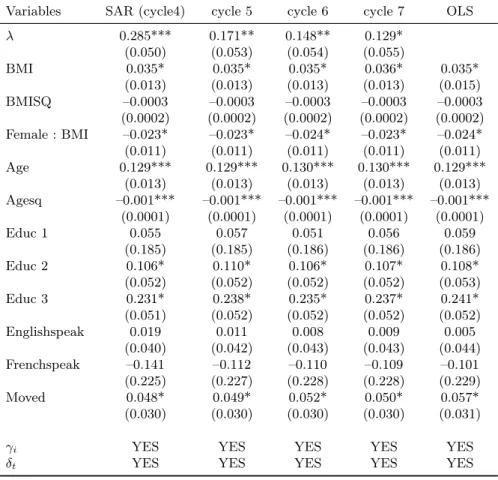
1.4 Estimation results of income model (model 1). . . 30
1.5 Estimation results of employment model (model 2) . . . 32
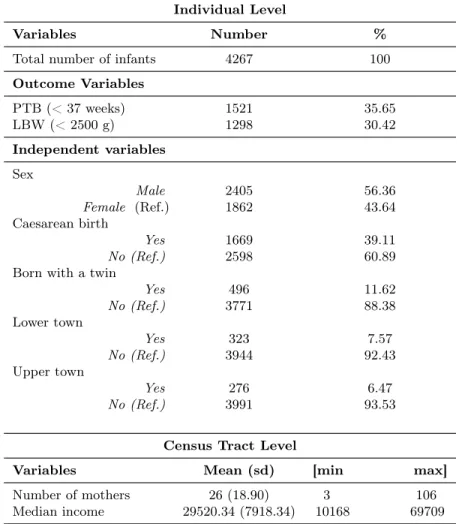
2.1 Summary of individual and census tract level characteristics in the CMA of Quebec. . . 49
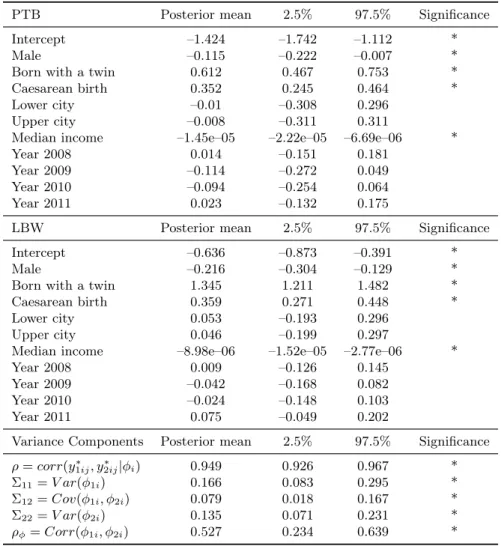
2.2 Estimates of parameters of adverse birth outcomes by the spatial Bayesian biprobit model. . . 56
2.3 Estimates of parameters of adverse birth outcomes by the spatial SUR model . 60 3.1 Socioeconomic characteristics by place of residence . . . 76
3.2 Summary of individual and census tract level characteristics in the CMA of Quebec. . . 77
3.3 Estimates of parameters of NIs and MIs by the spatial Bayesian biprobit model 81 A.1 Evolution of income in the NPHS . . . 102
A.2 Evolution of number of hours worked in the NPHS . . . 102
A.3 Moran’s Test. . . 102
Liste des figures
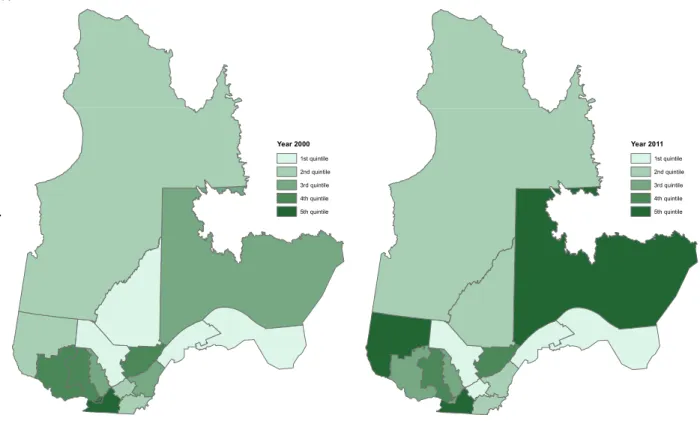
1.1 Quintile of regions by average income in the province of Quebec in the years
2000 and 2011 . . . 23
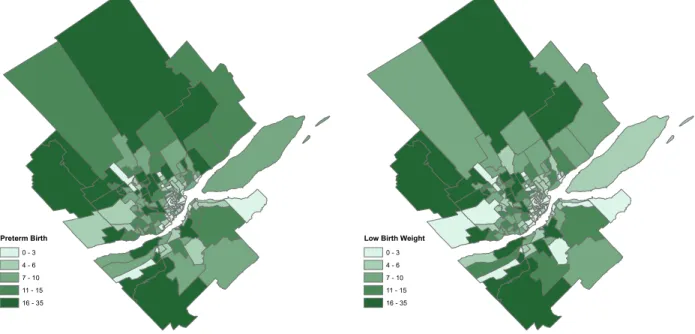
2.1 Number of preterm birth and low birth weight by CT in the CMA of Quebec. 48 2.2 Markov chain of income for PTB. . . 58
2.3 Markov chain of income for LBW. . . 58
3.1 Number of NIs and MIs among newborns in the NICU of CHUL by CT in the CMA of Quebec. . . 75
B.1 Markov chain of sex for PTB. . . 104
B.2 Markov chain of sex for LBW.. . . 104
B.3 Markov chain of twin for PTB. . . 105
B.4 Markov chain of twin for LBW. . . 105
B.5 Markov chain of caesarean birth for PTB. . . 105
B.6 Markov chain of caesarean birth for LBW. . . 105
C.1 Markov chain of pregnancy age for MIs. . . 106
C.2 Markov chain of pregnancy age for NIs. . . 106
C.3 Markov chain of weight for MIs.. . . 107
C.4 Markov chain of weight for NIs. . . 107
C.5 Markov chain of lower city for MIs. . . 107
C.6 Markov chain of lower city for NIs. . . 108
C.7 Markov chain of upper city for MIs. . . 108
C.8 Markov chain of upper city for NIs. . . 108
C.9 Markov chain of Income for MIs. . . 109
To my mothers whom I deeply miss, Ms. Dongo born Sylvie Kenfack Ngueguim and Ms. Ngnintedem born Jacqueline Ndonfack Tanke, I know you would have been proud of me ; To my beloved Laurette Raissa Tsobeng Ndongmo, for all the affection and love you have always given me ; To my fathers Etienne Dongo and Jérôme Ngnintedem, for having always advised me, supported and guided me on the perilous road of life.
Everything is related to
everything else, but near things are more related than distant things.
Remerciements
The accomplishment of this work has been made possible only by the combination of sev-eral efforts. Throughout my academic studies in Laval University’s Department of Economics, I have had the support of many people. First of all, I would like to thank my advisor, Profes-sor Guy Lacroix for his supervision, the relevance of his criticism and the advice that allowed me to refine this work as much as possible. I learned much from his frequent feedback that he provided despite his many other engagements. I also thank my co-advisor Professor Jean Dubé for his availability, his remarks and his suggestions which have undeniably contributed to the writing of this dissertation. I can not thank the both of you enough.
I deeply thank the administrative and teaching staff of the Department of Economics for the quality of the training we students receive. I especially thank Philippe Barla, Sylvain Dessy, Markus Herrmann, Benoit Carmichael, Carlos Ordas Criado, Bernard Fortin, Vincent Boucher, Marion Goussé, Martine Guay, Josée Desgagnes, Diane Nadeau, Jacinthe Morin and Ginette Therrien. I also thank the CRREP (Centre de recherche sur les risques, les enjeux économiques, et les politiques publiques), the QICSS (Quebec Inter-University Center for Social Statistics), the Industrial Alliance Research Chair on the Economics of Demographic Change and the School of Social Sciences for financial support of my doctoral studies.
I benefited from fruitful exchanges and advice from members of the GéoStat Center at Laval University. This allowed me to progress easily in my research and to constantly improve this work. My thanks go to: Marie-Andrée Drouin, Stéfano Biondo and Gaston Quirion.
My gratitude also goes to my entire family, near and far, for its unconditional support. I also thank my fellow students for their solidarity and cooperation. I am thinking of Nicolas Corneau-Tremblay, Carolle Kempa, Elfried Faton, Marie Albertine Djuikom, Koumou Gilles, Setou Diarra, Nono Simplice, Ngarsandje Guelmbaye, Mbea Bell, Ali Yedan, Christelle Wanko, Stephane Kwentchieu, Jean-Blaise Kalala, Anifa Mchanga, Ibrahima Sarr, Marius Sossou, Sylvia Grove, Théophile Bougna, Nathalie Sonkeng and Isaora Dialahy.
Avant-propos
This dissertation is the result of seven years of research. During my training as a statis-tician and economist at the Institut Sous-régional de Statistique et d’Économie Appliqué (ISSEA) in Yaoundé, Cameroon, I showed an interest in quantitative analyses and Bayesian statistics, which was strongly supported by my teachers in econometrics (linear model metrics, qualitative variable econometrics, panel data econometrics and time series econo-metrics). These experiences are the basis of my desire to develop original empirically-based solutions for specific problems. This is what motivated me to apply to the doctoral program in economics at Université Laval.
Upon meeting Guy Lacroix, the individual who would become my thesis director, in the fall of 2013, and after having read some of his research, most of which focused on peer effects, professor Lacroix made it clear to me that he wished to refocus his research toward health while doing advanced, cutting-edge quantitative analysis. This increased my interest in working with him because after the death of both of my mothers (my birth mother and also my guardian) due to illness, I had decided to make a health-related research contribution in their memory. This was an opportunity for me. It was therefore with great pleasure and enthusiasm that professor Lacroix and I discussed the recent document “Le Fardeau Économique de l’Obésité et de l’Embonpoint ” from the Institut National de Santé Publique du Québec (INSPQ), which was published in August 2013 and to which he had contributed as a member of the scientific committee. From that moment, I had an idea of how I could fit into an area of research related to obesity. This discussion and article became the starting point for my dissertation, the main objective of which was to introduce proximity modeling (the influence that individuals can have on others) in order to respond to public health questions (obesity, adverse birth outcomes, nosocomial infections and medical incidents). It also became clear that in my dissertation, I would model the spatiotemporal relationships between demographic, socioeconomic and health status characteristics of individuals. Before reaching the main objective of my dissertation, which allowed me to discover the importance of the spatial dimension in health, however, I would face several difficulties.
I met my co-director (Jean Dubé) in 2015 at the 83rd Congress of the Association Fran-cophone pour le Savoir (ACFAS). During the presentation of my preliminary results from
Chapter1, professor Dubé made pertinent comments that allowed me to significantly improve my methods and results. I asked him to be the co-director of my dissertation. During the research that was to come, my dissertation (all three chapters) focused solely on obesity. After my co-director agreed to work with me, he suggested that I not use the same National Popula-tion Health Survey (NPHS) database for the other two chapters. Indeed, the fact that the set of spatially-related characteristics of individuals changes with the cycles of the NPHS for static analysis, which was not taken into account in Chapter 1, is considered to be a limitation of the study in Chapter1. In order to avoid having the same limitations as in the other chapters, it was decided to use data from the Neonatal Intensive Care Unit of the Centre Hospitalier de l’Université Laval (CHUL) which is focused on health issues such as: adverse birth outcomes, nosocomial infections and medical incidents. Despite these adjustments, I faced many other challenges in carrying out my research. The main one was the non-availability of some vari-ables in the databases we used. Despite the study path being long and laborious, it was very rewarding. Indeed, I learned a great deal, and I was also introduced to the job of researcher.
The scholarships awarded by the Industrial Alliance Research Chair on the Economic Issues of Demographic Change, and also the Centre de Recherche sur les Risques, les Enjeux Economiques et les Politiques Publiques (CRREP) (formerly known as the Centre Interuni-versitaire sur le Risque, les Politiques Économiques et l’Emploi (CIRPÉE)), have helped me to carry out my research. My participation in several conferences and symposiums has also allowed me to improve many of methods and results. Note that we would like one or more chapters of this dissertation to appear as articles in peer reviewed scientific journals. I am the principal author of these three dissertation chapters.
Introduction
Good health can be considered as a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity (WHO,2012). Health is very important for the development of individuals in a society. Our health is intimately linked to our economic situation, and both are strongly influenced by socioeconomic factors that are part of a set of conditions called the social determinants of health. These social determinants of health are the circumstances in which people are born, grow, live, work and age, and the systems in place to deal with illness and disease (WHO, 2012). They have a major impact on health outcomes, especially for the most vulnerable populations. Health is therefore an important part of people’s lives. Without significant precautions, some individuals or groups of people could face public health problems including : obesity, adverse birth outcomes (low birth weight and prematurity), nosocomial infections (NIs) and medical incidents (MIs). The main objective of this dissertation is to introduce the modelling of spatial interactions to the analysis of these public health problems. This introduction is motivated by the first law of geography which states that : “Everything interacts with everything, but two close objects are more likely to do so than two distant objects”. This first law of geography is the basis of the fundamental concepts of spatial dependence and spatial autocorrelation that we test and correct for in three essays in health economics. These public health issues are important because, in Canada, the aggregate indirect costs (absenteeism, disability and premature death) caused by obesity is around $3.2 billion per year (Anis et al., 2010). In addition, it has been shown that poor health at birth affects cognitive development and can also lead to academic and social problems (Currie et al. (2010) ;Figlio et al.(2014)). NIs are a major cause of complications in health care, resulting in increased mortality and morbidity, prolonged hospitalization and a significant increase in health care costs (Berry, 2010). Human and financial costs associated with these infections and MIs are considerable due to their morbidity and high mortality. Indeed, according to a study by the Canadian Institute for Safety in Care (Etchells et al.,2012), the cost of a hospital infection in Canada is between CAD $2, 265 and CAD $22, 400. The cost of NIs for the Quebec health system is estimated at about $180 million per year (MSSS,2017).
Several factors are associated with the above-mentioned public health problems and the main ones are : biological factors (heredity, predisposition and others), behavioural and
life-style factors (nutrition, hygiene and others), socioeconomic factors (income, education level and others) and factors related to the place of residence (the individual’s immediate vicinity) of the individual. The environment in question here is defined as all the elements that consti-tute the neighbourhood of individuals, households and other groups that are likely to interact with it directly or indirectly (Guérin-Pace and Collomb,1998). Health economics research has devoted considerable attention to the role of some of these individual factors associated with the above mentioned public health problems. However, the links between where individuals live, and these public health problems is very poorly documented. It is in the analysis of these linkages that this dissertation fits. The state of health of a person could depend on his/her position in the social hierarchy and place of residence. Researchers in various countries have reported that place of residence is associated with health beyond individual-level risk factors (Diez-Roux et al. (2000) ; Pickett and Pearl (2001) ; Kawachi and Berkman (2003)). Consi-deration of the influence that an individual’s neighbourhood has on his or her health status is an important aspect of modelling to be taken into account. The space in question here is a social space, producing human groups that organize and enhance it to meet fundamental objectives such as habitat, exchanges and communication1. As a geographical concept, space is defined by the form (type and structure of “distances”, organization of space, magnitude of statistical links between things) that relations between places take, whether for an indivi-dual, a group or a geographical entity2. Overlooking space could take data out of its spatial context ; it would mean hearing only one part of the story. Floch (2012) and Elhorst(2010), for example, show the importance of spatial analysis techniques in empirical studies. Long ignored in empirical studies requiring the use of geographical data, these spatial econometric techniques are now increasingly being applied and make it possible to study the presence and impact of geographical spillover effects on economic behaviour (Le Gallo,2002).
Economic and econometric reasons, notably linked to spatial autocorrelation, can be at-tributed to the renewed attention paid to the inclusion of spatial aspects in analyses. One example is the development of new lines of research that take into account economic inter-actions. Indeed, new geographical economy emphasizes spatial externalities, agglomeration economies and all other forms of spillover effects (Duranton,1997). Spatial econometric tech-niques also make it possible to take into account other types of interactions between agents such as social norms or neighbourhood effects. Geographical entities are most often spatially autocorrelated. This means that entities that are close to each other tend to be more similar than those that are farther away. This feature means that, for a particular observation, the process generating the data is influenced by dependent variables in neighbouring observations. Spatial autocorrelation therefore differs from temporal autocorrelation, which is unidirectio-nal since only the past influences the future. On the other hand, spatial autocorrelation is multidirectional since everything is related to everything (Le Gallo, 2002). This generalized
1. http://geoconfluences.ens-lyon.fr/glossaire/espace
interdependence has the consequence of making the methods of addressing spatial autocorre-lation more complex. This interdependence between observations causes marginal effects to differ from those in classical modelling. Exploration and analysis of spatial aspects of these relationships has several important economic implications. In particular, it allows better targe-ting of geographical areas where priority interventions are needed, for example to reduce rates of public health problems. As mentioned above, there are many econometric reasons for using spatial models, since descriptive analyses highlight proximity effects and spatial correlations. According to Dube and Legros(2014), there are many advantages of using methods intended for spatial data : i) avoiding parameter estimation bias ; ii) avoiding inefficiency and iii) avoi-ding prediction bias. Methodological refinement must be balanced against the economic issue and the complexity of these new models, particularly in terms of interpretation. Throughout the rest of the dissertation, the expressions “immediate vicinity”, “nearby environment” and “neighbourhood” will be considered to have the same meaning. From this meaning follows the definition of the neighbourhood effect, which is according to Vallet (2005), the result of a set of processes by which the nearby environment affects health, economic situations and behaviour (delinquency, violence or depression, individual development and academic results, among others).
An individual in general does not live isolated in society. Indeed, he/she is called upon to exchange and interact with other individuals in his/her immediate vicinity (both work-related or personal life). When these interactions take into account the conditions and practices of individual and social life that are related to the geographical position of individuals as is the case in this dissertation, geographical proximity could determine the intensity of social interac-tions. Thus, the spatial interaction of an economic agent with other heterogeneous agents may lead to collective behaviours or an aggregate pattern. Relationships between values observed in nearby geographical spaces have long been of concern for geographers and, in the recent past, for economists as well.Tobler (1970) summarized this problem in a formula often referred to as the first law of geography, mentioned in the first paragraph. This dissertation models the spatiotemporal relationships between demographic and socioeconomic characteristics and the health of individuals. Health modelling is innovative in that it integrates the characteristics of individuals’ nearby environment as well as spatial correlations in unobservable characteristics. These two components of the determinants of health are generally neglected or omitted in econometric studies of public health issues that use georeferenced data.
Geolocated data contains information on the location of individuals, in addition to the values of the variables. By using spatial data, we run the risk of having an absence of inde-pendence between geographical observations. Researchers have become increasingly interested in considering spatial aspects in the analysis of economic issues over the last two decades (Benko, 2008). This could be explained by an interest in regional and urban economies or by an increased availability of geolocated data. Spatial econometrics is used to incorporate the dependence between proximate observations. It deals with interaction effects within and
between geographical units, such as postal codes, neighbourhoods, rural districts, towns and cities, provinces/states or countries, states or countries. To illustrate interactions between in-dividuals and their estimated effects, several models are estimated in this dissertation based on different databases over different periods. It is generally observed that the samples of data collected according to the geographical unit of analysis (regions, census tracts, dissemination area, counties, dissemination islands, points of space) are not independent. Indeed, nearby observations tend to have similar values. Since the correlation that might exist between indi-viduals results from social interactions, it is important to take into account the spatial aspect in modeling. Therefore, the geographic location and spatial environment of each individual or region must be taken into account when analyzing social disparities in health as is the case in this dissertation. In this work, I test in general whether there is spatial correlation between the health outcomes and income of individuals. Spatial data can be used in several fields, for example in epidemiology with the modeling of the spread of a contagious disease. They can also be used in criminology (identify locations of crime and its dissemination) and in real estate (predict housing prices). In this dissertation, as mentioned before, we will use them in the field of health. We will pay particular attention to the following public health issues : obesity, adverse birth outcomes (low birth weight and prematurity) and health conditions in hospitals (nosocomial infections and medical incidents). Indeed, few studies using geolocated data have addressed these public health issues. We have, for example, Chu and Ohinmaa (2016),Larose et al.(2016),Henry and Kollamparambil(2017),Kim and von dem Knesebeck (2018), Brunello and D’Hombres (2007),Greve (2008), Cawley et al. (2005) and Garcia and Quintana-Domeque(2006) who analyzed the relationship between income and obesity without exploring the possibilities of using spatial modeling. Similarly, Joseph et al. (1998), Wilkins (1990),Pearl et al. (2001),Panico et al. (2015) and Martinson and Reichman(2016) instead analyzed the relationship between socioeconomic status (educational attainment or income) and adverse birth outcomes without exploring the possibilities of using spatial modeling. In the same vein,Clark et al.(2004),Berry(2010),Stavroudis et al. (2008) andLerner et al.(2008) analyzed the relationship between poor hospital health conditions (nosocomial infections and medical incidents) and adverse birth outcomes without also exploring the prospects of spatial modeling. Throughout this dissertation, emphasis will be placed on the importance of spatial interactions between individuals with regard to health issues.
This dissertation, which is organized into three chapters, explores socioeconomic and de-mographic relationships with certain public health issues in Quebec. Body mass index (BMI) is the health indicator used in the dissertation to determine whether an individual is obese. Chapter one discusses the relationship between income and obesity. Overweightness and obe-sity are defined as a BMI of greater than or equal to 25 and 30, respectively. With the rising rate of obesity in Canada in general, and in Quebec in particular, there are currently concerns about the health costs associated with obesity. Obese people are more likely to suffer from chronic diseases such as diabetes, hypertension and heart disease. These people therefore use
more health care than people of normal weight. Thus, the costs of health care due to obe-sity may well increase. The prevalence of obeobe-sity has been on the rise in Quebec since 1987 (INSPQ, 2012). There is reason to believe that the use of public health care resources, and therefore health care costs related to obesity, may also increase in the years to come. In fact, in 2010, 16.4% of the population in Quebec was obese (INSPQ, 2012). In addition, between 1987 and 2010, Quebec increased from one in three adults (34.6%) to one in two being over-weight or obese (50.5%). According to (INSPQ, 2012), low-income adults are more affected by obesity than those with a high income. It is in this context that we would like to know whether obesity is a source of discrimination among continuously employed people in Quebec. The previous question has not yet been addressed in the economic literature in the context of spatial analysis. The spatial approach to this relationship is the one adopted in this chapter. In this chapter, two hypotheses were tested. The first concerns the correlation between income and obesity, and the second concerns the correlation between the number of hours worked and obesity.
Chapter two analyzes the relationship between adverse birth outcomes and the income of census tracts (CTs) in which mothers live. Infants weighing less than 2500g are considered low birth weight and infants born at less than 37 weeks gestation are considered preterm birth (WHO,2012). According to Statistics Canada (2016), 5.6% of babies born in 2000 and 6.3% in 2013 had a low birth weight. During the same period, the proportion of premature newborns went from 7.3% to 8%. In Quebec, these rates averaged 5.7% for low birth weight and 7.4% for premature births between 2000 and 2013 (INSPQ,2010). In this study, we use data with higher-risk cases from the Neonatal Intensive Care Unit (NICU) of the Centre Hospitalier de l’Université Laval (CHUL). Recently, it has been shown that poor health at birth is associated with lower scores for cognitive development and also many schooling and social problems (O’Campo and Urquia,2012). Taking care of premature births and low birth weight is very costly for public health in Quebec. Joseph et al. (1998),Guildea et al. (2001), Krieger et al. (2003),Liu et al.(2010) andCampbell et al.(2018) believe that these adverse birth outcomes are correlated with household income. These relationships have not been thoroughly discussed in the literature and we do this by exploring the benefits of our spatial data. Research in spatial econometrics is currently oriented towards incorporating spatial effects into qualitative variable and spatiotemporal models (Anselin(1988b) ;Anselin et al.(2013)). We incorporate these spatial effects as part of this dissertation in chapters2and 3. The hypothesis that there is a correlation between the median income of the census tracts where mothers live, and each type of adverse birth outcomes was tested in this chapter. The spatial biprobit and spatial SUR (seemingly unrelated regressions) models were used to analyze the correlation. We introduce a spatiotemporal lagged variable in the SUR spatial modeling to show the importance of spatially and temporally lagged gestational age on the gestational age of newborns. The introduction of this variable in the SUR spatial modeling is our main contribution in this second chapter of the thesis. Doing this SUR analysis provides a thorough explanation of the analyzed relationships.
Chapter three examines the relationship between adverse birth outcomes, the income of CTs in which mothers live and the health conditions of newborns (nosocomial infections and medical incidents) in the neonatology unit. An infection is said to be nosocomial when it occurs more than 48 hours after admission3. A medical incident is any action or failure to
act that adversely affects an infant. Health conditions at birth have a major impact on the life course of an individual. Newborn, low birth weight and preterm infants are susceptible to nosocomial infections and medical incidents. Nosocomial infections and medical incidents are a major category of adverse events in the health care system in Canada (Aziz et al., 2005). Nosocomial infections are a worldwide problem and are one of the leading causes of death and morbidity among hospitalized patients (WHO,2002). In Canada, Zoutman et al. (2003) estimate that 220, 000 nosocomial infections occur each year, causing 8, 000 related deaths. Stavroudis et al. (2008) find that there is a correlation between medical incidents and low birth weight or premature infants. Income disparities are associated with the premature death of 40, 000 Canadians a year, or 110 premature deaths per day (Tjepkema et al., 2013). The risk of contracting a nosocomial infection varies according to the patient’s profile, the level of hygiene, or the care provided. When the patient is a newborn, as in this chapter, management is even more delicate. The germs responsible for nosocomial infections most often originate from the patient himself or herself, and then staff or medical devices that come in contact with the patient at a later point re-introduce it in a way that ultimately causes that same patient their infection4. In saying the germs come from the patient, for the purposes of this chapter this could be the mother of the newborn or her immediate vicinity. This is one of the main reasons for the rationale and motivation for spatial analysis in this chapter. These different observations encourage us to ask the following question : Do newborns have a higher chance of contracting nosocomial infections or suffering medical incidents when their CT income is low ? How about when they have a low birth weight or preterm birth ? These relationships have been less covered in the literature. The empirical analysis of these relationships was made using geolocated data while exploring whether their use results in superior statistical outputs. It is with the data from the previous chapter that this analysis was performed. We also use a spatial biprobit model to analyze the correlations.
3. http://www.cclin-arlin.fr/nosopdf/doc04/0013685.pdf
4. https://www.inserm.fr/information-en-sante/dossiers-information/
- Chapitre
1
-Is There A Private Cost for Obesity in Quebec ? A
Spatial Panel Analysis
1.1. Résumé
Ce chapitre évalue le coût privé de l’obésité au Québec. La croissance remarquable de l’obésité au cours des dix dernières années laisse penser que le Québec pourrait faire face à des coûts sociaux importants en termes de services de santé et de réduction de la productivité des travailleurs dans un avenir à court et à moyen terme. L’analyse est réalisée à partir des données de l’Enquête Nationale sur la Santé de la Population et couvre la période des cycles de 4 à 9. L’objectif de cette étude est double : évaluer la relation spatio-temporelle (i) entre l’obésité et le revenu, et (ii) pour les personnes travaillant au Québec, l’obésité n’a pas de conséquences sur leurs revenus ; entre l’obésité et la performance du marché du travail, en tenant compte des différentes interactions pouvant survenir entre les individus. Plus précisément, l’obésité a-t-elle des conséquences sur le revenu et le nombre d’heures travaillées ? La principale innovation de l’étude est la prise en compte de la dimension spatio-temporelle de ces relations et des analyses au niveau individuel. Nous utilisons un modèle spatial panel (modèle spatial autorégressif) aux données restreintes au niveau de la province de Québec au Canada. Nous constatons que : (i) il existe une autocorrélation spatiale des revenus entre individus au Québec ; (ii) pour les personnes travaillant au Québec, l’obésité n’a pas de conséquences sur leurs revenus ; et (iii) par rapport aux hommes, l’effet de l’indice de masse corporelle est plus faible chez les femmes. Contrairement aux études précédentes, on constate qu’au Québec les personnes obèses travaillent plus d’heures que les personnes ayant un indice de masse corporel normal.
Mots-clés : Indice de Masse Corporelle (IMC), Revenu, Tests d’autocorrélation spatiale, Matrice exponentielle négative, Économétrie spatiale, Modèle autorégressif spatial.
1.2. Abstract
This chapter assesses the private cost of obesity in Quebec. The remarkable growth of obesity over the past ten years implies that the province of Quebec could face significant social costs both in terms of health services and reduced worker productivity to the more or less imminent future. The analysis is performed from the National Population Health Survey and covers the period of cycles 4 to 9. The objective of this study is twofold : to evaluate the spatial and temporal relationship (i) between obesity and income, and (ii) between obesity and labour market performance, accounting for the different interactions that may occur between individuals. More specifically, does obesity have consequences for income and the number of hours worked ? Taking into account the space-time dimension of these relationships and analyses at the individual level is the main innovation of the study. We apply a spatial panel model (Spatial Autoregressive model) to data from the province of Quebec in Canada. We find that : (i) there is a spatial autocorrelation of incomes across individuals in Quebec ; (ii) for people working in Quebec, obesity does not have consequences on their incomes ; and (iii) relative to men, the effect of body mass index is lower for women. Unlike previous studies, we observe that in Quebec obese people work more hours than people with normal body mass index.
Keywords : Body Mass Index (BMI), Income, Spatial autocorrelation tests, Negative exponential matrix, Spatial econometrics, Spatial autoregressive model.
1.3. Introduction
Obesity can be defined as an excess of adipose tissue that is distributed throughout an individual’s body in a way that is detrimental to his or her health1. The obesity epidemic has reached major proportions worldwide. According to Dietz (2011), global obesity rates have doubled in the last three decades. His research also states that 5% of men and 8% of women worldwide were obese in 1980. By 2008, those rates had nearly doubled, and 10% of men and 14% of women were obese, corresponding to 205 million and 297 million persons respectively. In that same year, 1.5 billion adults were considered overweight, which is a pre-condition of obesity (Dietz, 2011). This picture of obesity is further developed by Golubic et al. (2013), whose article specifies that in 2005 over 400 million adults were obese around the world. In addition, their projections indicated that, by 2015, the prevalence would increase to more than 700 million. In 2005, the estimated obesity rates among men and women in England was 21.3% and 24.8%, respectively. In 2007 − 2008, 32.2% of adult men and 35.5% of adult women were obese or overweight in US (Flegal et al.,2010). Moreover, 67.7% of the adult U.S. population is overweight or obese, and approximately 34% is obese (Flegal et al., 2010). In contrast, over 1976 − 1980 roughly 46% of the U.S. population was overweight or obese and 15% was obese (Flegal et al.,1998). As for Canada, in 2008, 62% of all adults were reported as being overweight or obese (CIHI and PHAC,2011).Katzmarzyk(2002) shows that obesity rates increased from 5.6% in 1985 to 14.8% in 1998. Several years later,Vanasse et al.(2006) indicates that in 2003, 15.2% of Canadian individuals aged 20 years or over were considered obese. Overall, the Canadian prevalence of adult obesity has increased substantially from 6% to 18% between 1989 and 2011 (Twells et al.,2014). Vanasse et al. (2006) also revealed the heterogeneity of obesity in different regions of Canada, ranging from 6.2% in Vancouver to 47.5% in native areas.
It is known that obesity has several co-morbidities, which are long-term chronic diseases that evolve slowly with time (WHO (1997) ; NHLBI (1998) ; Blouin et al. (2014)). It is im-portant to recall that a disease is an alteration in the state of health manifested by a set of signs and symptoms that can be perceived directly or indirectly, corresponding to general or localised, functional or lesional disorders, due to internal or external causes and involving some change over time2. Obesity has also been shown to be associated with increased health care utilization, decreased productivity, increased chronic disease and shorter life expectancy (Kpelitse et al.,2014). These consequences are more pronounced for morbid obesity. According to Kpelitse et al. (2014), the most chronic diseases that stand out in Quebec and the rest of Canada are : heart disease, diabetes, cancer, hypertension, asthma and lung disease. These diseases are tremendously expensive sicknesses affecting economic outcomes of these obese persons, such as income and employment. Obesity not only increases morbidity and mortality
1. https://www.inserm.fr/information-en-sante/dossiers-information/obesite
rates, but also imposes an increasing economic burden on individuals as well as on the state. Otherwise stated, obesity causes major indirect and direct costs.Trogdon et al.(2008) define direct costs as the costs associated with the provision of health services and indirect costs as costs associated with lost productivity of obese or overweight workers. Those costs can mainly be associated with absenteeism, disability and premature mortality. For example, comparing annual health care costs of an obese individual to those of individuals with a normal body mass index (BMI) shows an additional cost ranging from 14.7% for men in Ontario (Janssen et al., 2009) to 54% for woman in Australia (Reidpath et al., 2002). Other studies do not quantify the individual-level costs, but rather those for the entire population. For example, it is estimated that obesity cost 630.1 million dollars to the health system in Alberta in 2005, equivalent to 2.8% of health spending in this province (Moffatt et al.,2011). In this study, we focus on indirect and private costs. An important indirect cost is the impact of adult obesity on labour market outcomes such as income and hours worked. The objective of this first chapter is therefore to examine the relationship between obesity (measured through BMI) and labour market outcomes (income and number of hours worked) from a spatiotemporal perspective. It would be interesting to understand the impact of obesity on the labour market outcomes of working age adults in Quebec. Regarding indirect and private costs in Quebec, in tables A.1, A.2in appendix we observe that the gap between the income of obese and non-obese workers has been increasing over time in Quebec. We also observe that the gap between the number of hours worked by obese and non-obese persons is almost the same in Quebec.
Evidence shows that obesity could potentially have a substantial private cost. Caliendo and Lee(2013) andMosca(2013) have identified two main mechanisms through which obesity could adversely affect labour market outcomes. First, health problems associated with obesity could reduce productivity and increase absenteeism from work. Second, there could be discri-mination by employers against obese individuals. This could notably be the case where health insurance premiums paid by employers are higher for obese people, especially in countries such as the United States. This second reason is less applicable in Canada because the Canadian health care system provides free of charge medical and hospital services to citizens without the employer having to assume the costs. Regardless of the payment mechanism, clearly there could be a decrease in income or in the number of hours worked.
Many factors influence obesity. In addition to our individual genetics and life choices, the environment in which we are born, grow up, live, work and age also has a significant influence on whether we are obese or not. It is in this environment that we learn and share certain habits and behaviours. The environment we are referring to here is the set of elements that make up the neighbourhood of individuals, households and other groups that are likely to interact directly or indirectly with it (Guérin-Pace and Collomb, 1998). Several studies have been conducted on the effect of obesity on labour market outcomes, but the results vary by country and socioeconomic group. For example, Chu and Ohinmaa (2016), Larose et al. (2016),Henry and Kollamparambil(2017),Kim and von dem Knesebeck(2018),Brunello and
D’Hombres (2007), Greve (2008), Cawley et al. (2005) and Garcia and Quintana-Domeque (2006) analysed these relationships without exploring the prospects for using spatial model-ling. Although informative on the relationship between obesity and labour force participation, most studies ignore the impact of spatial interactions between individuals in the analysis of the relationships. The objective of this chapter is to re-evaluate this relationship by introducing spatial analysis, an aspect that is not well developed in the literature. The description of the phenomenon of proximity between individuals or objects was popularized by Tobler (1970) with what is now known as the first law of geography : “Everything interacts with everything, but two close objects are more likely to do so than two distant objects”. In recent years, spa-tial analysis of health issues has had some renewed interest among economic and geographic researchers. Failure to consider the immediate vicinity of individuals in the analysis of these relationships fails to indicate spillovers or the effect that individuals/neighbours might have on others. This first chapter is innovative in that it models, for the first time, the influence of geographical proximity on the relationship between income and obesity, on the one hand, and the number of hours worked and obesity, on the other. Spatial proximity influences the results with, for example, different marginal effects. It is in this field of research that this dissertation chapter is positioned.
One of the main reasons for paying particular attention to spatial autocorrelation is theoretical and is based on the development of new lines of research that take into account economic interactions between economic agents. Specifically, new geographical economy em-phasizes spatial externalities, agglomeration economies and any other form of spillover effects (Duranton, 1997). Spatial econometric techniques can also take into account other types of interactions between agents such as social norms or neighbourhood effects. Another important reason for the interest in spatial autocorrelation can be the increasing availability of spatial data. The spatial dimension is needed to model spatial correlation in behaviour. According to Dube and Legros(2014), this correlation (spatial autocorrelation of income) takes two forms : first, a “contagion” effect, namely that the income of individuals is a function of the average income of individuals living nearby. The second form of spatial correlation is more traditional and takes into account similarities in behaviour due to variables that are unobservable for the analyst but observable for individuals. Spatial autocorrelation therefore differs from tempo-ral autocorrelation which is unidirectional since only the past influences the future. On the other hand, spatial autocorrelation is multidirectional since everything is related to everything (Le Gallo,2002). The space in question here refers to the notion of geographical space, which is a social space, produces human groups that organize and enhance it to meet fundamental objectives such as housing, exchanges and communication3. Space as a geographical concept is defined by the form of relationships between places, whether for an individual, a group, or a social group4. According toDube and Legros(2014), there are many advantages to modelling
3. http://geoconfluences.ens-lyon.fr/glossaire/espace
with spatial data : i) avoiding parameter estimation bias ; ii) avoiding inefficiency ; iii) avoiding prediction bias and iv) modelling spillover effects. Space is therefore a major player in this problem. Spatial exploration of the analysis of these two relationships has several important economic implications, one of which is to better target the administrative regions of Quebec in which priority intervention will be required to reduce obesity rates, for example.
Given the importance of obesity and the chronic diseases it generates on one hand and geographic space where people live on the other, the main questions of our study, in a spatial-panel context, are : Does being obese have an effect on the personal income of individuals in Quebec over the 12 years from 2000 to 2011 ? And, does being obese affect the number of hours worked of individuals over the 12 years from 2000 to 2011 ? More specifically, does obesity have consequences for income and the number of hours worked ? This first chapter of the dissertation analyses whether obesity is a potential source of socioeconomic discrimination that Quebecers face in the labour market. This study is important for several reasons. First, this study could serve as an important tool for decision making in public health. Indeed, this will allow us to know whether the health costs related to obesity in the province of Quebec mainly come from the demand for health care or from lost productivity. Second, this study also provides general clues on how to reduce the impact of obesity on income, on the health system and the economy. The correlation between obesity and income derives its importance in this study simply from the fact that obesity in Canada has increased dramatically in recent years, from 6% in 1989 to 18% in 2011 (Twells et al.,2014). This study is done using spatial analysis and will be different from other research, which is mostly done without geolocated data. Long ignored in empirical studies, spatial econometric techniques are now increasingly being applied to study the presence and impact of geographical spillover effects on economic behaviour. The main objective of this work is to assess the correlation between obesity and income, and between obesity and the number of hours worked, in Quebec taking into account the different spatial interactions occurring between people in Quebec. To achieve this goal, we need to explore obesity (measured by BMI) in the labor market over time and space in Quebec. Specifically, we can test whether obese workers earn less or have a smaller number of hours worked due to health-related constraints.
The remainder of the chapter is organized as follows. Section 1.4 provides a literature review of the relationship between obesity and labour market outcomes (income and number of hours worked). Section1.5describes the dataset used and provides descriptive statistics. In Section1.6, we present the spatial panel econometric models before presenting the results in Section1.7. Finally, Section1.8concludes and offers some policy recommendations.
1.4. Literature Review
The direct cost of obesity has been the subject of many studies, but the indirect cost of obesity has been relatively understudied, particularly in the Canadian health literature.
From reports on the economic burden of the obesity produced by Health Canada,Blouin et al. (2014) estimated that, in Quebec, the combined costs of absenteeism, disability and premature mortality due to overweightness and obesity reached $800 million per year.Anis et al.(2010) estimated that, for Canada, the aggregate indirect costs (absenteeism or reduced productivity at work, disability and premature death) caused by obesity attained $3.2 billion per year. Likewise, Finkelstein et al.(2010) calculated that in the United States, reduced productivity at work led obesity to generate an economic loss of nearly 31 billion per year. These previous studies show us that obesity could impact the trajectory of individuals. The impacts that will be analyzed here are related to individuals’ labour market outcomes. The literature on the associations between obesity and labour market outcomes points to three possible angles of analysis : the effect of obesity on labour market outcomes (discrimination and/or productivity), the effect of labour market outcomes on obesity, and the effect of a third factor on obesity and labour market outcomes (for example, individual time preference). This study is in the first group : the analysis of the effect of obesity on labour market outcomes. Kim and von dem Knesebeck (2018) explored the direction of the relationship between income and obesity by specifically assessing the importance of the social relationship (lower income is associated with higher risks of future obesity) and the relationship going in other direction. The results of their study suggested that there was more consistent evidence of the relationship going in other direction. Therefore, further examination of inverse causal processes is necessary to understand the relationship between income and obesity. Studies on the genetics of behaviour indicate that approximately half of variation in BMI is due to non-genetic factors such as individual choices and environment (Henry and Kollamparambil,2017). In order to review the literature regarding the association between obesity and labour market outcomes, research was conducted in several countries, particularly OECD countries, as the results may be more relevant to the Canadian population. Very few Canadian studies on the relationship between obesity and its consequences on labour market outcomes (income and employment) exist. These include studies by Chu and Ohinmaa (2016), Larose et al. (2016) and Kpelitse et al. (2014).
Due to the difficult nature of their derivation, few studies have used instrumental va-riables based on the location of individuals (locality). For example,Huffman and Rizov(2014) in post-Soviet Russia andChu and Ohinmaa (2016) in Canada used an instrument based on geographic area. Variables such as gender, age, occupation type, education and marital status were the main factors they used in their analyses. The results of Huffman and Rizov (2014) showed an inverted U-shaped effect of BMI on the probability of employment for both men and women. No evidence of a wage penalty for a higher BMI was found. Overall, the results show negative effects of obesity on employment only for women, but not on wages. Howe-ver, regression results from the study byChu and Ohinmaa (2016) for women showed strong negative associations between BMI and personal income among obese women. A one-unit in-crease in BMI in women is associated with a 0.6% dein-crease in personal income according to
the model specification chosen, regardless of race. This review of the literature shows that, beyond the classical factors studied, to the best of our knowledge no studies have examined the role that geographic proximity may play. Factors not considered by the aforementioned authors as influences on individual income, such as the income of an individual’s neighbours, fails to capture spillover effects and could result in prediction bias. However, the data used by the authors provide the possibility to explore the use of such a variable. Spatial proximity could have influenced the results with, for example, a different impact on marginal effects. No significant association was found between BMI and income for overweight and obese men. Rather, positive associations have been observed in individuals with normal BMIs, but these associations are not robust across all model specifications. The instrument used in this model-ling is based on area (locality). One motivation for using this instrument is that the average BMI and obesity prevalence rates in the respondent’s home area will capture environmen-tal influences affecting attitudes and behaviours related to the determinants of obesity. The advantage of such a variable is that it is easy to obtain. Taking into account the proximity between individuals in the way done by the authors is not optimal because it does not allow an ideal methodological refinement of the proximity between individuals. Using the variable (income of neighbours) that we suggested above would avoid parameter estimation biases and inefficiency. Although necessary and very important, the use of this variable requires additio-nal calculations, for example the construction of the spatial weighting matrix. The authors also used a lagged variable of BMI, in the range of 4 years, to make comparisons with previous studies such as that of Morris (2006). Like Morris (2006), the study by Chu and Ohinmaa (2016) found no evidence of any causal effect between obesity and personal income using the desired causal model.
Other studies such as Cawley (2004) and Larose et al. (2016) have instead used lagged BMI values as instrumental variables in their analyses. The main factors used in their studies were : gender, age, race, ethnic group, number of children, immigration status, education level and regional (urban and rural) indicators. In addition to ordinary least squares estimation, Cawley (2004) used one lagged variable, lagged 7 years variable and found that BMI is as-sociated with lower wages for white women. This result could be explained mainly by the fact that obesity lowers wages either because of reduced productivity or because of weight-related discrimination in the workplace. The negative relationship between BMI and wages observed for other ethnic and gender groups seemed to be due to unobserved heterogeneity. This unobserved heterogeneity would have been accounted for using a spatial analysis that would consider the spatial correlation of unobserved effects and spatial interactions between individuals. However,Larose et al.(2016) instead used 2−, 4− and 6−year lags of BMI in their analysis of the relationship between obesity and labour market outcomes. They showed that obesity is not significantly associated with employment participation, but that it is associated with a reduction in hourly wage rates and annual income among women by approximately 4% and 4.5%, respectively. In addition, they found evidence (at a 10% significance level) that
obesity in Canadian men was associated with a 2% reduction in earnings. It would have been preferable to do a multidirectional analysis rather than a unidirectional analysis as was in fact the case. Indeed, everything is spatially connected. The authors could have exploited the availability of their geographic data (although only available at the postal code level) to take advantage of this multi-directional analysis. This could have improved the marginal effects of the relationship between obesity and labour market outcomes.
The latest Canadian study in this literature review is that of Kpelitse et al. (2014) who used cross-sectional data to study the effect of household income on obesity. Variables such as age, marital status, immigration status, education, household size, hours worked per week and geographic variables were used by the authors in their modelling. Neighbourhood unemployment rate and household income are the instruments used to identify the causal effect. Their causal model suggests that a 1% increase in household income leads to a 0.76% and 0.27% decrease in the probability of being obese for men and women, respectively. Contrary to theoretical expectations, no evidence of a larger negative effect of income on BMI and obesity for more educated individuals was found. One of the advantages of our study over that of Kpelitse et al.(2014) is the use of personal income rather than household income. In addition, the longitudinal nature of our database allows us to account for changes in our variables of interest over time. Indeed, panel data, rather than cross-sectional data, are recommended to control for unobserved heterogeneity because a panel structure allows to control for individual-specific effects.
The effect of obesity on labour market outcomes has been analyzed in several continents such as : Europe (Böckerman et al. (2019), Caliendo and Gehrsitz (2016), Huffman and Ri-zov (2014), Johnston and Lordan (2014), Härkönen et al. (2011), Lindeboom et al. (2010), Greve(2008),Brunello and D’Hombres(2007),Garcia and Quintana-Domeque(2006),Morris (2006), Cawley et al. (2005)) ; America (Kosteas (2012), Renna and Thakur (2010), Cawley et al. (2005), Cawley (2004), Baum and Ford (2004), Pagan and Davila (1997)) and Africa (Henry and Kollamparambil (2017), Some et al. (2016)). The results of these studies vary between countries and socioeconomic groups. Although most cross-sectional and longitudinal results in the literature suggest that both positive or negative results on labour market out-comes could be found depending on method and context, in populations, these studies did not take into account unobserved factors that may lead to inaccurate estimates. Inconsistencies in the theoretical and methodological analysis of these unobserved factors are an example of elements that could lead to inaccurate estimates. The need to take into account elements that may generate biases of unobserved heterogeneity is therefore important. Henry and Kollam-parambil (2017) and Some et al. (2016) analyzed these relationships in South Africa and, in addition to the variables of interest, the main factors studied were : age, gender, ethnicity, marital status, household size, education and perceived health. Probit and tobit models and then a Gaussian mixture model to account for endogeneity were used by Henry and Kollam-parambil(2017) whileSome et al.(2016) used instrumental variable models only. Using panel