View of Is Next-Generation Sequencing Appropriate for the Clinic?
Texte intégral
Figure
Documents relatifs
The in vitro e ffects of 4 arylimidamides (DB811, DB786, DB750 and DB766) against the proliferative tachyzoite stage of the apicomplexan parasite Besnoitia besnoiti were
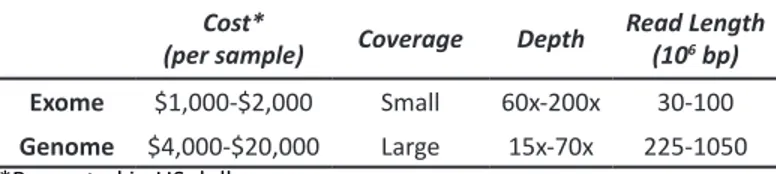
Here, we review the use of the current high-throughput sequencing platforms with a special focus on the associated challenges (regarding sample preparation and
Entropy-satisfying scheme for a hierarchy of dispersive reduced models of free surface flow... dispersive reduced models of free
As in the previous section, we follow and adapt the proof scheme for the linear bandit algorithms analysis to derive polylogarithmic distribution-dependent regret upper bounds
Montoro, Chow, Chrestin, Duan, Galand, Garcia, Kolesnikova-Allen, Le Guen, Leclercq, Lekawipat, Omokhafe, Pujade-Renaud, Putranto, Sales, Seguin, Teerawatanasuk. IRRDB NATURAL
To assess the capacity of the method to detect and identify different enteroviruses in samples containing mixtures, we performed two types of experiments: (1) mixed samples
Here we introduced a complete protocol called V-ASAP for whole- genome virus sequencing based on multiplex PCR and amplicon se- quencing, and a new reference-free analytical
We used an array including ALPL gene, genes of differential diagnosis COL1A1 and COL1A2 that represent 90% of OI cases, SOX9, responsible for CD, and 8 potentially modifier genes
